Article Text

Abstract
Background From a health and safety perspective, it is critical to use adequate, evidence-based breast screening guidelines. The aim of this quality improvement project was to improve physicians’ compliance with breast cancer screening guidelines to enhance the mammography screening rate among eligible women; this was achieved through the implementation of multifaceted changes to the hospital’s processes and the improvement of physicians’ attitudes towards the guidelines.
Methods The project used the Plan-Do-Study-Act method to implement the changes. This was a pre-post evaluation study. The data were collected from patients’ charts. The primary outcome of interest was the rate of physician compliance with mammography screening guidelines before and after the implementation of the process changes. A literature review was conducted to determine which women should be identified as eligible for mammography screening.
Intervention The interventions targeted physician knowledge and hospital processes. Improving doctors’ expertise was achieved by implementing the US Preventive Service Task Force recommendation for mammography screening every 2 years for women aged 50–74 years. The process modifications included the establishment of a system that would be effective in identifying at-risk patients and reminding physicians at the point of care.
Results Over the course of this study, 825 patients met the criteria for breast cancer screening. The rate of physician compliance with the breast cancer screening guideline increased from 2% to 69% after 23 weeks, and the control charts demonstrated a reliable process.
Conclusion This project examined the relationship between different interventions (identification of the eligible patient, reminder alerts and physician knowledge) and physician compliance with mammography screening guidelines. The results suggest a positive link between the study variables and physicians’ compliance with mammography screening guidelines.
- implementation science
- evidence-based medicine
- efficiency
- organisational
- patient safety
- quality improvement methodologies
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- implementation science
- evidence-based medicine
- efficiency
- organisational
- patient safety
- quality improvement methodologies
Introduction
Problem description
Breast cancer is the leading cause of death for women worldwide,1 especially when it presents in the late stages.2 The evidence suggests that the detection of breast malignancy in early stages improves the curability and survival rates.3 Many guidelines suggest mammography screening as the gold standard for the early diagnosis of breast cancer in eligible females.4 Surprisingly, there is consistent evidence that physicians are non-compliant with breast cancer screening guidelines.5 Within the authors’ hospital, physicians rarely advised mammography screening in 2019. A retrospective review of mammography screening appointments confirmed that only 2% of eligible patients received advice from their primary physicians. Consequently, less than 1% of eligible patients underwent mammography screening in the same period. Likewise, in accordance with the baseline survey, only 4 out of 24 physicians were aware of the latest updates regarding breast cancer screening guidelines.
Available knowledge
Current evidence suggests mammography as a crucial tool for the screening of breast cancer.6 According to data from the WHO,6 mammography screening helps reduce the mortality rate of breast cancer by 20%.6 The US Preventive Services Task Force (USPSTF) recommends that mammography screening for breast cancer commence at 50 years of age and end at 74 years of age and occur every 2 years in asymptomatic women who do not have a genetic predisposition or history of chest radiation.7 This recommendation has been adopted widely among healthcare institutions worldwide.8 However, many physicians do not recommend mammography screening to their patients,9 resulting in women’s poor participation in screening endeavours.10 According to Plourde et al,11 physicians’ beliefs and attitudes towards breast cancer screening guidelines play a critical role in the provision of mammography screening medical advice given to patients.11 Physicians’ lack of compliance with evidence-based guidelines is a result of several barriers, including time constraints, absence of system reminders, lack of patient insurance coverage and physician health literacy related to breast cancer screening, leading to average performance.4 9 12 13 Therefore, numerous interventions have been developed to address these barriers, aiming to improve physicians’ adherence to breast cancer screening guidelines.14
Project rationale
Synthesising information on the outcomes of previous studies, the study team used multiple analytical tools to determine the scope of intervention in their institute. The authors used Donabedian’s structure-process-outcome model to examine the healthcare system within the hospital.15 The main interventions in this project were the establishment of a capable system to identify at-risk patients and remind physicians at the point of care and improve physicians’ knowledge and attitudes towards breast cancer screening guidelines.
Specific aim
The quality improvement project discussed in this article was conducted to establish whether the active implementation of breast cancer screening guidelines in the primary care setting could improve the compliance of physicians with evidence-based recommendations. Appropriately, the primary objective was to increase the rate of physician compliance with mammography screening at the point of care for eligible patients from 2% to 60% by the end of May 2020.
Methods
Study setting
This study was conducted in a primary care centre (PCC) at the oldest and largest non-profit private hospital on the island of Bahrain. The PCC provides primary care and wellness services. The centre was purposively selected because it sees a high volume of outpatients seeking well-being (on average more than 300 visits per month) and because the centre was implementing only the USPSTF breast cancer screening guideline during the evaluation period. Additionally, the national accreditation for the PCC was due. Hence, implementing breast cancer screening guidelines would help the hospital become aligned with the high accreditation standards16 and provide evidence for compliance with evidence-based guidelines.17
Intervention
Rectifying identified problems requires finding the root cause and then selecting the proper interventions.18 The problem in this project was that physicians rarely advised patients to undergo mammography screening. The authors used the fishbone tool to scrutinise the problem thoroughly and determine the causes of the problem.19 The team determined multiple causes for inadequate physician compliance with breast cancer screening guidelines (see online supplemental appendix 1: Fishbone). Together, the team conducted a voting session with stakeholders to identify the vital few causes of inadequate compliance to be addressed by employing the Pareto principle; the Pareto principle is capable of distinguishing 20% of causes that are accountable for 80% of a problem.20 The vital few causes of inadequate compliance with breast cancer screening guidelines were (1) no reminder at point of care, (2) no identification process for eligible women, (3) confusion regarding breast cancer screening guidelines, and (4) time constraints during consultation (see online supplemental appendix 2: Pareto chart). Then, with the assistance of the countermeasure matrix tool (see online supplemental appendix 3), the authors distinguished the proper interventions for each cause21 (see online supplemental appendix 3). Therefore, the interventions aimed to address physicians’ expertise and hospital processes by implementing the guideline and creating a reminder system, respectively.
Supplemental material
The team outlined an implementation plan by using the Plan-Do-Study-Act (PDSA) model for improvement (MFI),22 which is essential in the implementation stage.23 Moreover, the authors embraced the Kirkpatrick four-level evaluation model to assess education since each level of the model informed the authors about the effectiveness of the educational programme.24 The following section describes the MFI and the conducted PDSA cycles.
Model for improvement
The MFI has two stages: (1) key issues that must be addressed before the commencement of the PDSA method, and (2) experimenting with the changes by using the PDSA method. The key issues are setting the aims, establishing the measurement and selecting the changes, which are essential steps before testing the changes.22 The study used the MFI for the project because of its effectiveness in healthcare improvement projects.23
PDSA 1: improving physicians’ knowledge
Key issues before PDSA
Studies have shown that improving physicians’ knowledge about breast cancer screening guidelines is associated with a change in attitudes and behaviour towards the guidelines and improves the recommendation rate to patients by 15%.4 25 In the same vein, the PDSA 1 intended to improve the knowledge of primary care physicians. Hence, the team decided to use a continuous medical education (CME) lecture as a method to improve the knowledge of physicians.26 Moreover, to determine the effects of CME, Kirkpatrick and Kirkpatrick27 established four levels of training evaluation. The four-level training model initially assesses the reaction of participants to the lecture. Next, level 2 examines attendees’ knowledge before and after the lecture. Level 3 evaluates the behaviour of the learners after the educational programme, and finally, level 4 assesses the results of the training at the organisation level.27
During the interim evaluation, the authors performed the level 1 and 2 evaluations while the evaluation of the physicians’ behaviour was done in later stages. Level 1 was assessed by using a reaction survey while knowledge was evaluated by using an online pretest and post-test methodology.
Testing the changes
Plan
As part of the planning process, there was a series of consultative meetings between the study team and experts (general surgeons, gynaecologists and family physicians) to reach consensus on breast cancer guidelines. On reviewing the different guidelines, the team and experts decided to follow the USPSTF guideline due to its efficiency and effectiveness.7
Do
The primary investigator prepared the lecture and the online test consistent with the adopted guidelines. The team reviewed the educational material and communicated with the educational department to make the CME a mandatory lecture for all physicians and sent the prelecture/postlecture online test. At the beginning of December 2019, the lecture was delivered two times, 1 week apart, to reach all candidates.
Study
A reaction survey28 was distributed on the delivery of the lectures, and the findings showed that 56% of physicians were satisfied with the delivery style. Furthermore, 24 out of 24 physicians become aware of the latest updates regarding breast cancer screening guidelines in accordance with the prelecture/postlecture online tests.
Act
After all the changes were established in the later stages, the behaviour of the physicians after the training was evaluated.
PDSA 2: identifying eligible patients at the point of care
Key issues before PDSA
According to the literature, system reminders help enhance the uptake rate of the guidelines among physicians and improve the compliance rate of patients with mammography screening.26 29 Hence, the aim of this PDSA was to establish an efficient process that could identify eligible patients and remind physicians at the point of care.
Furthermore, evidence has shown that early engagement of stakeholders is associated with less resistance and generates momentum.30 Therefore, the main change in this step was engaging allied health staff in the identification process by empowering and training stakeholders about the new changes. During the interim evaluation, initially, the team assessed level 2 of the Kirkpatrick model by using the pre-post test. The behaviour of allied health staff was tracked in later stages by evaluating the identification rate of eligible patients by allied health staff.
Testing the changes
Plan
There was a meeting between the study team and Pimary care center (PCC) staff (receptionists, registered nurses and doctors) to identify the bottleneck of the current process and propose an appropriate change. On examining the current process, the attendees determined that the hospital system did not provide any suggestions for identifying eligible patients for screening or remind physicians at the point of care.
Accordingly, the planning team established a new step in favour of patient identification that would remind physicians. The process would start from the time of registration; when the eligible patient registered in the hospital’s system for a regular visit, the receptionist would mark the patient’s registration paper with the eligibility stamp, indicating the eligibility of the patient for mammography screening. During the triage period, the nurse would receive the stamped registration paper and document the need for mammography screening alongside the triage note. Finally, at consultation time, the patient would arrive at the consultation room where the doctor’s role would be to advise the eligible patient about the mammography screening. Then, the physician must document the appropriate International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) in the patient records, represented by the code for special screening for neoplasms of the breast, which is Z12.3.31
Do
The primary investigator prepared the new process map for the identification process. In December 2019, the team used the morning huddle with allied health staff to introduce the changes.
Study
Following the briefing, the primary investigator assessed the staff’s understanding of the new process by asking the following question to the 19 staff pretraining and post-training: Do you know your role in this project? While none of the staff were aware of their roles in the project prior to training, all of them were able to pinpoint their roles after training. This evaluation was consistent with the second level of the Kirkpatrick model.
Act
The behaviour of receptionists and nurses was tracked over time on a weekly basis, and corrective measures were performed concurrently to maintain a high level of allied health staff compliance with the process.
Study design and data collection
A pre-post study design was used to measure the efficiency of the physician education and process put in place to enhance physician compliance with breast cancer screening guidelines. The baseline (preintervention) data were collected by the study team at the hospital between January 2018 and August 2019. The postintervention evaluation was integrated with the Study component of the PDSA. The team conducted weekly meetings for the interim evaluation. The data were collected between 1 December 2019 and 9 May 2020. An audit tool was developed to capture the generated data from the aforementioned implementation.
The data points were chosen to determine the measures that would reflect the change. The team identified three data points and their sources: (1) the number of eligible patients, which was collected from patient registers; (2) the number of patients identified by allied health, which was collected from the nursing book; and (3) the number of recommendations given to eligible patients by the physicians, which was collected from the ICD-10 register from the electronic medical record (EMRs). The data were collected by senior receptionists and senior registered nurses. Prior to the data collection, the participants received an explanation of the project. The data were stored in a Microsoft Excel sheet. The assessment of the quality of the collected data was the responsibility of the nurse in charge. The nurse in charge audited the data for accuracy on a regular basis by comparing the data to the documented sources.
Measures
The measures were selected to determine the behaviour of physicians and allied health staff during the training and process changes. The study team used summative (outcome) and formative (process) measures to assess the performance.32 The formative measures included the number of eligible patients identified by allied health staff while the summative measure included the number of recommendations given to eligible patients.
Outcome measure: compliance of physicians with guidelines at the point of care
The primary outcome measure was the compliance of physicians with breast cancer screening guidelines by advising eligible patients. The target was to reach 60% compliance with a 6-month period. Physician compliance was defined as offering mammography screening to each eligible patient presented to the clinic. On the implementation of the multiple PDSA cycles, the study team initiated an audit of patients’ medical charts. The main data points were the number of eligible patients who had registered in the hospital system during the study period and the number of mammography screening recommendations given to eligible patients. The senior nurse searched for physicians’ documentation of ICD-10 Z12.3 in patients’ medical charts, which indicated that mammography screening advice had been given to the patient. The data were analysed weekly and discussed with the project stakeholders to improve the performance and approach the target.
Process measure: compliance of allied health staff with the identification process
The identification process in this project was the responsibility of receptionists and nurses at registration and triage stages, respectively. Accordingly, assessment aimed to determine the degree to which staff complied with the new process following the training. Hence, the team used two process measures, namely (1) compliance of receptionists with the identification steps of the process, and (2) compliance of nurses with reminder alert steps of the new process. The target for the receptionist and nurses was 60% compliance with the respective process measures.
Receptionist compliance was defined as the identification rate of eligible patients at registration and was determined based on the number of highlighted eligible patients out of the total number of patients. Nurse compliance was defined as documentation of the indication for mammography screening in the triage note.
Analysis
The objectives of this study were evaluated before and after the interventions, and the results were displayed by using statistical process control charts.33 We used Nelson’s rules to contrast variation due to special and common causes34 since the improvement scope is variation dependent. While special causes require the investigation of the unpredictable cause and making a correction, common variation indicates the stability of the process.34 The data were stored in a Microsoft Excel sheet according to confidentiality policy, and data analysis was performed by the study team with the help of QI Macros software (2017).
Results
Physician compliance
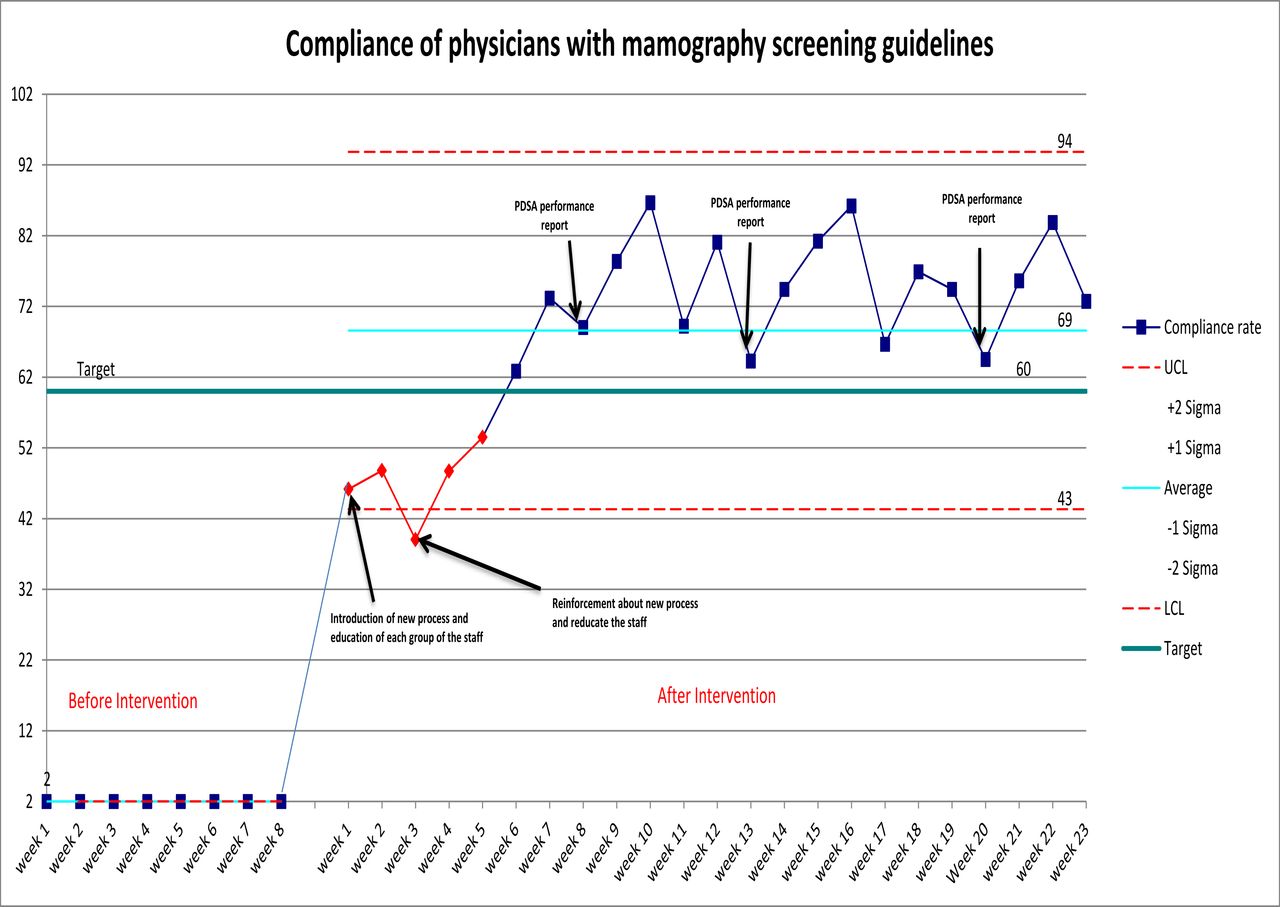
Over the course of this study, 825 patients met the criteria for breast cancer screening. Recommendations given by physicians to eligible patients at the point of care were tracked, and the rate of compliance with the guidelines by doctors increased from 2% to 69% after 23 weeks. The control charts for physician compliance with breast cancer screening guidelines are presented in figure 1. We evaluated the overall impact of various changes on the rate of physician compliance with mammography screening. The phenomenal growth of the compliance rate after implementing the changes can be seen clearly in the chart. However, in December 2019, following the introduction of the CME and notation of patient eligibility for screening in patient charts, week 3 showed an assignable point that indicated an unstable process. The study team used peer-to-peer education methods for physicians as an effective way to encourage physician participation35 and retraining of allied health staff and performance feedback36 as reinforcement actions to improve physician compliance. Then, the graph showed that there had been a steady increase in the compliance rate, which exceeded the target in week 7 after the interventions. The chart then demonstrated common variations rather than special causes, which indicated a reliable process.
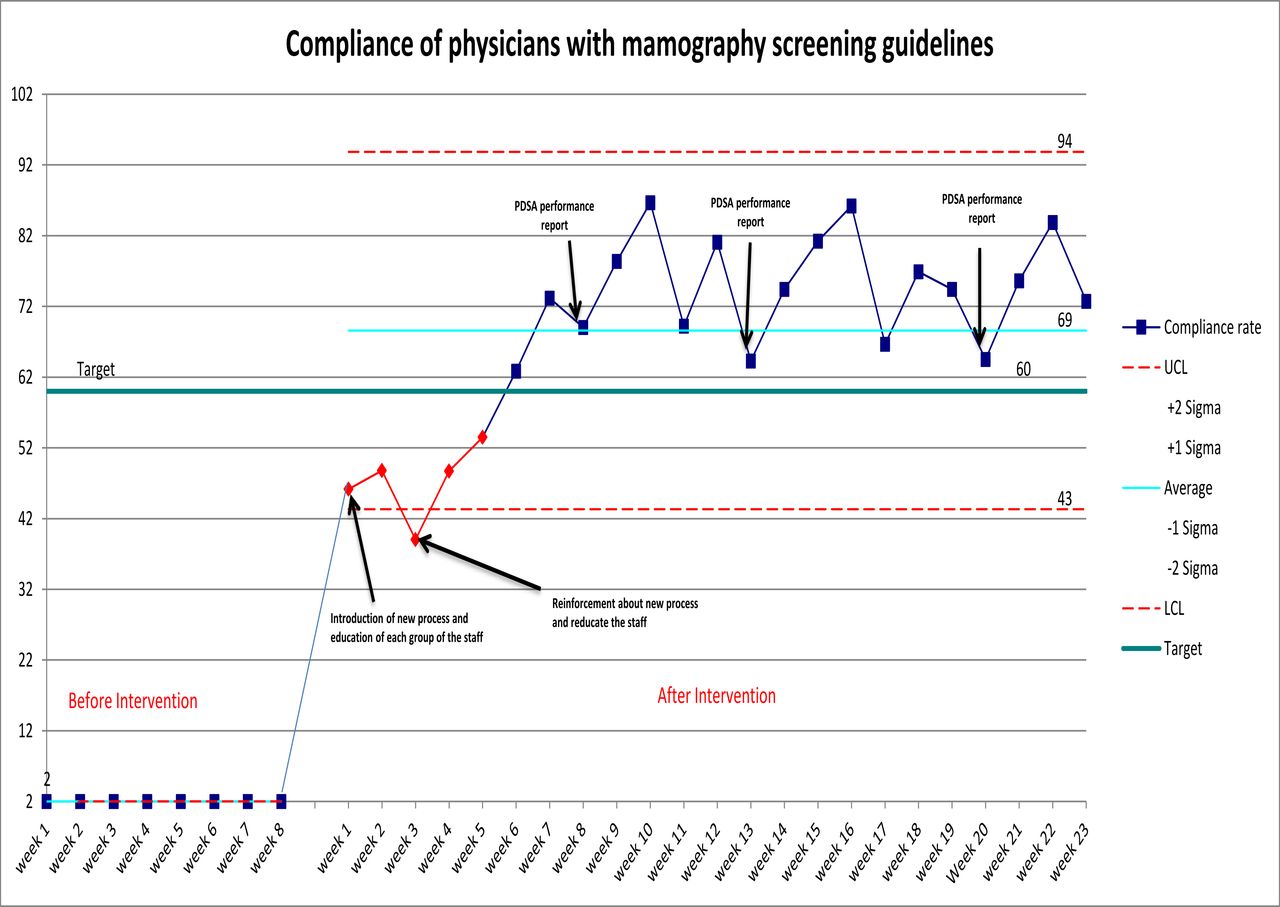
Control chart of physician’s compliance rate. PDSA, Plan-Do-Study-Act.
Receptionist compliance
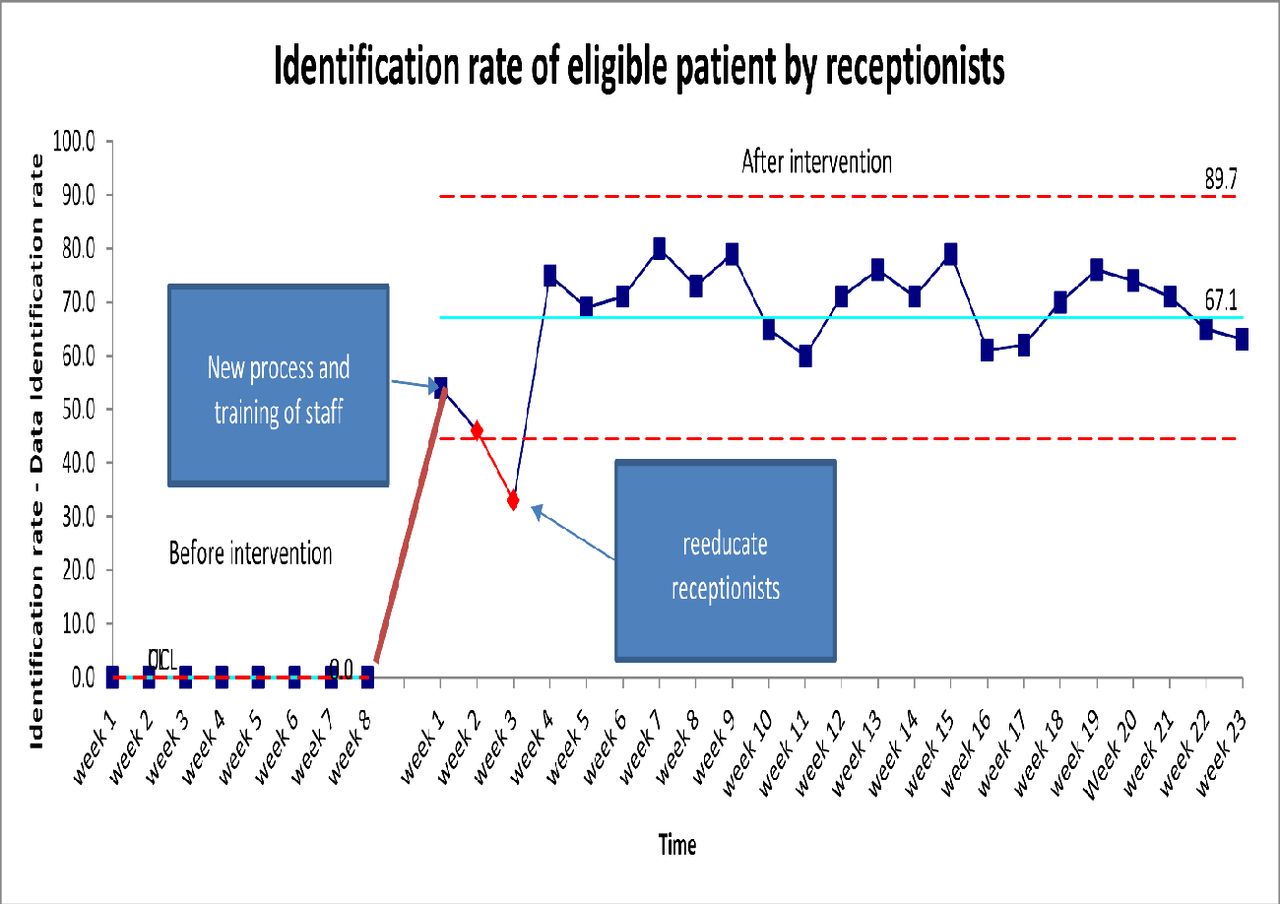
The control chart in figure 2 demonstrates the difference in behaviour before and after the training. The average reminder rate increased by 67% compared with the reminder rate before the intervention. Initially, the curve showed instability, but after the CME, performance feedback and re-education were provided. The chart showed only random variation, which indicated the stability for the new process.

Control chart for identification rate by receptionists.
Nurse compliance
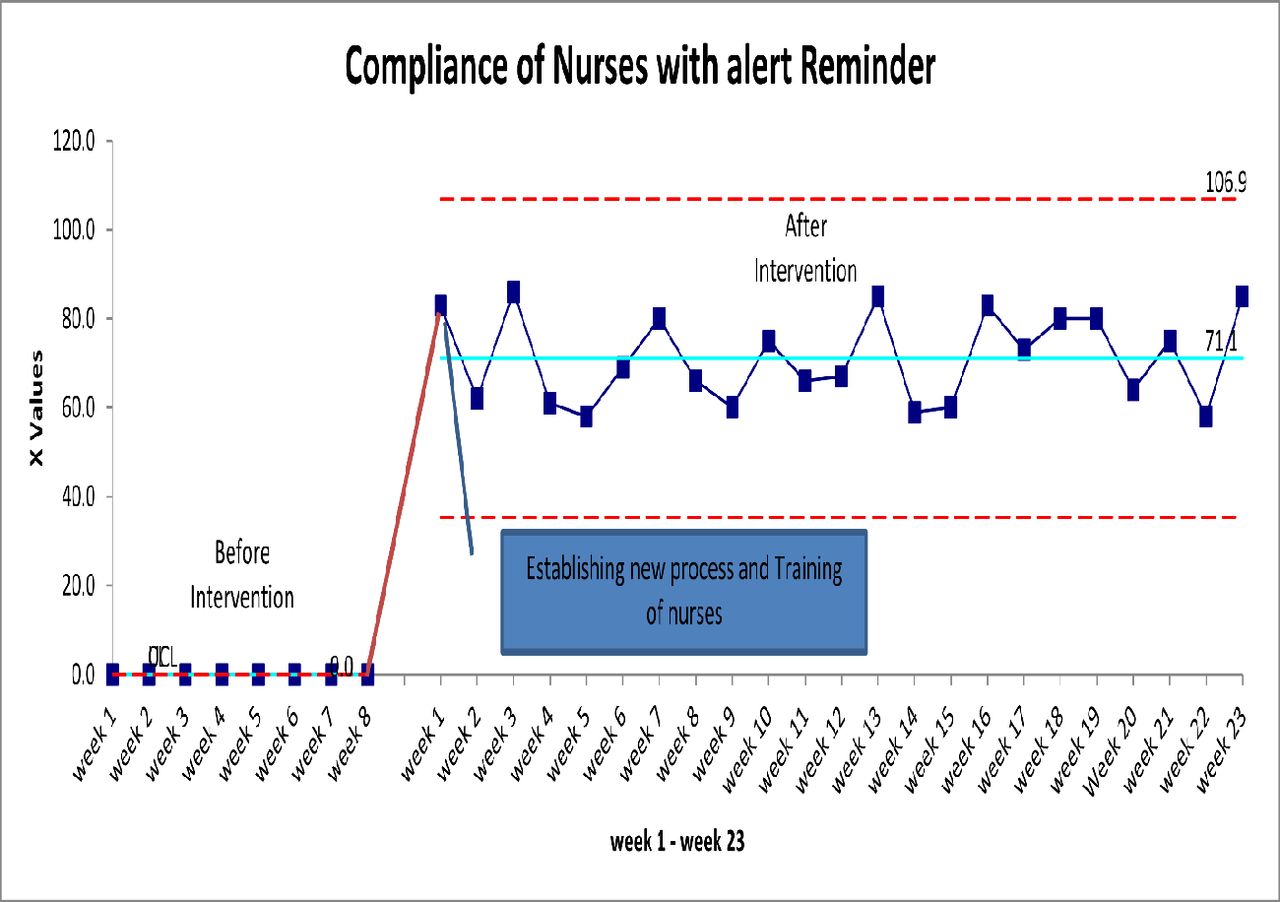
The control chart in figure 3 demonstrates the difference in behaviour before and after the training. The average reminder rate increased by 79% compared with the reminder rate before the intervention. Moreover, the control chart shows only random variation, which indicates stability for the new process.

{kind=link}
{kind=link}
{kind=link}
Control chart for alert reminder by nurses.
Discussion
Summary
We observed a significant, substantial improvement in the rate of physician compliance with breast cancer guidelines following the introduction of physician educational programmes and reminder alerts. The results of the intervention matched those observed in earlier studies by emphasising the role of a reminder alert in translating the research into practice29 37 38; the results were also consistent with previous studies illustrating that physician education is associated with better compliance with evidence-based recommendations.4 25
Interpretation
Multiple interventions were launched simultaneously to underpin the appropriate streamlining of changes. The impacts of the multiple changes were analysed by determining their effect on physician behaviour regarding the selected breast cancer guideline. This study aimed to assess the impact of the active implementation of the guideline on physician compliance rate.
The absence of reminder alerts and lack of a process to identify eligible patients were contextual causes of the non-compliance of physicians with breast cancer screening guidelines in the hospital. Moreover, the literature review provided evidence for the usefulness of reminder alerts in promoting preventive medicine recommendations.26 29 Accordingly, the reminder alert process was implemented. The results of the study matched those observed in earlier studies by emphasising the role of reminder alerts in translating research into practice, showing a strong association between reminder alerts and physician compliance with mammography screening guidelines. In conclusion, using reminder alerts and following the guidelines at the point of care help disseminate evidence-based recommendations.
Studies have shown that improving physicians’ knowledge about breast cancer screening guidelines is associated with a change in physicians’ attitudes and behaviours towards the guidelines and improves the recommendation rate to patients.4 25 In this study, the results of the intervention further support the importance of improving physicians’ knowledge. According to the control chart, the adherence of physicians to the USPSTF breast screening guideline improved remarkably after the CME. This result confirms the positive relationship between education and the implementation of screening guidelines.
Limitations of the study
Our study has multiple limitations. Although the findings highlight a pathway for the implementation of evidence-based recommendations, the project is context dependent. Hence, the generalisability of the study results is problematic. Moreover, the scope of this study is limited to the healthcare system and physicians. One major drawback of this approach is that a considerable amount of literature has been published on patient and cultural factors due to their impact on overall compliance with mammogram screening. Accordingly, the impact of physician compliance with guidelines on screening rates requires further studies and research to establish the association.
Conclusion
This project examined the impacts of different interventions on physician compliance with screening. According to the results, the link between the study variables (identification of eligible patients, reminder alerts and knowledge of physicians) and physicians’ compliance with mammography screening guidelines was remarkable, as compliance improved from 2% preintervention to 69% postintervention. However, patient behaviour following physician counselling was not assessed in this study. Accordingly, a further study with more focus on the impact of physicians’ advice on patients should be conducted to determine the factors influencing the overall mammography screening rate.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Ethics approval
This project was approved by the hospital’s ethical committee and complied with the confidentiality and privacy policy; access to patient information was given to two licensed doctors who signed the confidentiality policy and worked at the PCC and were not allowed to share patient data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RMA was the project lead and led the team in the proposed changes. MS was the consultant of the project. SE-N was the coordinator of the project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.