Article Text

Abstract
Introduction Laboratory blood testing is one of the most high-volume medical procedures and continues to increase steadily with instances of inappropriate testing resulting in significant financial implications. Studies have suggested that the design of a standard hospital admission order form and laboratory request forms influence physician test ordering behaviour, reducing inappropriate ordering and promoting resource stewardship.
Aim/method To redesign the standard medicine admission order form-laboratory request section to reduce inappropriate blood urea nitrogen (BUN) testing.
Results A redesign of the standard admission order form used by general internal medicine physicians and residents in two large teaching hospitals in one health zone in Alberta, Canada led to a significant step reduction in the ordering of the BUN test on hospital admission.
Conclusions Redesigning the standard medicine admission order form-laboratory request section can have a beneficial effect on the reduction in BUN ordering altering physician ordering patterns and behaviour.
- quality improvement
- continuous quality improvement
- cost–benefit analysis
- efficiency
- organisational
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The Canadian public health system is faced with the challenge of providing effective patient-centred care while maintaining economic sustainability. Laboratory blood testing is one of the most high-volume medical procedures and continues to increase steadily with instances of inappropriate testing.1–3 Between 16% and 56% of laboratory testing is estimated to provide no clinical value.2 Laboratory test collection and processing accounts for approximately 4% of the Canadian public healthcare budget.3 Inappropriate laboratory testing includes all tests ordered of which, regardless of result, do not change the patient care management.4 In hospitals, the practice of daily blood draws has become a norm and enabled through bundling of tests and order sets.5
Overutilisation of laboratory testing although highly variable in magnitude, is present in a variety of clinical settings and most commonly initiated during the first medical assessment.2 Moreover, it has increasingly become routine for many laboratory investigations to be ordered without clear clinical indications from history and focused physical examination.6 This overutilisation is demonstrated to an even greater extent in teaching hospitals as the orders are primarily written by residents, who have been found to order unnecessary laboratory investigations at a higher rate than staff physicians.7 This is not only financially costly, but can also contribute to negative patient experiences such as discomfort, further unnecessary testing and anaemia.8 9
Significant reductions in laboratory ordering have been reported through interventions of education and job aides, to redesigning standard admission order sets, laboratory forms or software as well as multimodal approaches.10–17 There can be risks associated with these interventions that target reductions in laboratory test order such as physicians under ordering when clinically required and missing possibly relevant information for the patients diagnosis or management.18 The blood urea nitrogen (BUN) test or the urea test is commonly ordered with creatinine, often adding little value to patient management at significant cost.19 The issue necessitating this quality improvement (QI) study was a provincial laboratory test use report that identified one health region in the province of Alberta, Canada had the highest total annual BUN testing which represented 48% (672 000 tests or $3.6 million dollars) of the provincial BUN volume which was approximately 1.4 million tests at a cost of approximately 7.1 million dollars (BUN estimate cost per test—$5.00.20 This health region was paper based, used a medicine admission order form with common laboratory tests bundled (electrolytes, BUN and creatinine) with a single checkbox and provided no test order frequency options. Every laboratory test has associated costs in our system for reagents, labour, equipment calibration and thus having these common tests grouped with BUN which was often not of significant clinical value19 raised expenses needlessly.
Further, within this health region one hospital A, had started a QI project 1 year earlier focused on reducing lab test ordering in general internal medicine (GIM) units. Hospital A interventions included targeted resident education sessions prior to unit rotation, a job aide outlining common clinical indications for ordering the BUN test shared with both attending and resident physicians and to heighten physician awareness of the admission laboratory test order frequency, several unit process adjustments were made (ie, highlighting the lab Kardex, and placing the lab Kardex onto the doctors clip board) to prompt timely adjustments as required.20
The objective of this study was to evaluate the decline in BUN testing due to admission order form redesign at two teaching hospitals’ GIM units in one health region. Our expectation was that the admission order form redesign would highlight factors influencing physician ordering practices and to encourage a future culture of physician ordering practice in teaching hospitals for sustained reductions in unnecessary BUN ordering.
Methods
Setting
This project was carried out at two teaching hospitals A and B in western Canada within the GIM units. The two hospitals are located in the same health region and city, have a similar patient population and the number of GIM units per hospital were 5 and 6 units. In addition to the staff physicians these hospitals have rotating medical students and residents in 8-week and 4-week rotations, respectively. Both hospitals at the time of this study used paper-based ordering, charting and used the same medicine admission order form. On the decision to admit a patient, the staff physician or resident completes the medicine admission order form in the emergency department (ED) and the ED clerk processes the orders. Once the patient is on the unit clerk reviews the admission orders and will continue the laboratory test orders as indicated on the admission order form.
Initial evaluation
Prospective chart audits (N=50) to evaluate baseline laboratory test ordering on GIM units found that BUN test ordering was frequent (76%−38/50) and often continued as a daily order despite the results being normal. This frequency of BUN orders often did not align with the 13 clinical indications for which BUN blood tests were deemed appropriate based on literature review,21 22 local specialists and the provincial laboratory which prompted further investigation (see box 1).
Acceptable indications for ordering bun blood test
The list was developed after literature review and consultation with local experts to help guide thoughtful bun ordering. It is not meant to be exhaustive or to replace individual clinical judgement.
On admission of hospitalised patients with community acquired pneumonia.
Adrenal insufficiency.
Haemolytic uraemic syndrome.
Metabolic acidosis.
Sickle cell disease.
Suspected toxic shock syndrome.
Suspected or known acute or chronic renal failure.
Blood urea nitrogen clearance testing for dialysis.
Severe sepsis or shock.
Pericarditis.
Acute pancreatitis.
Gastrointestinal bleed.
Acute intoxication.
After closer review, it was determined that poor admission order form design was a contributing factor to increased inappropriate BUN blood test ordering.
Intervention
Based on these findings the medicine admission order form laboratory section was updated: unbundled all laboratory tests, removed the BUN test, added frequency options and a free text section for physicians to order any laboratory test if necessary, on hospital admission (figure 1). Updated admission order form implementation was staggered between the two hospitals, hospital A in April 2018 and hospital B in September 2018. The rationale for the staggered implementation approach was to determine the singular effect of the order form redesign at hospital B. As there were other QI interventions underway at hospital A during this study timeframe, while hospital B had no interventions apart from the redesigned admission order form. Both hospitals had the GIM division physician leaders inform their teams of the rationale for improvement along with the redesigned form implementation start date.
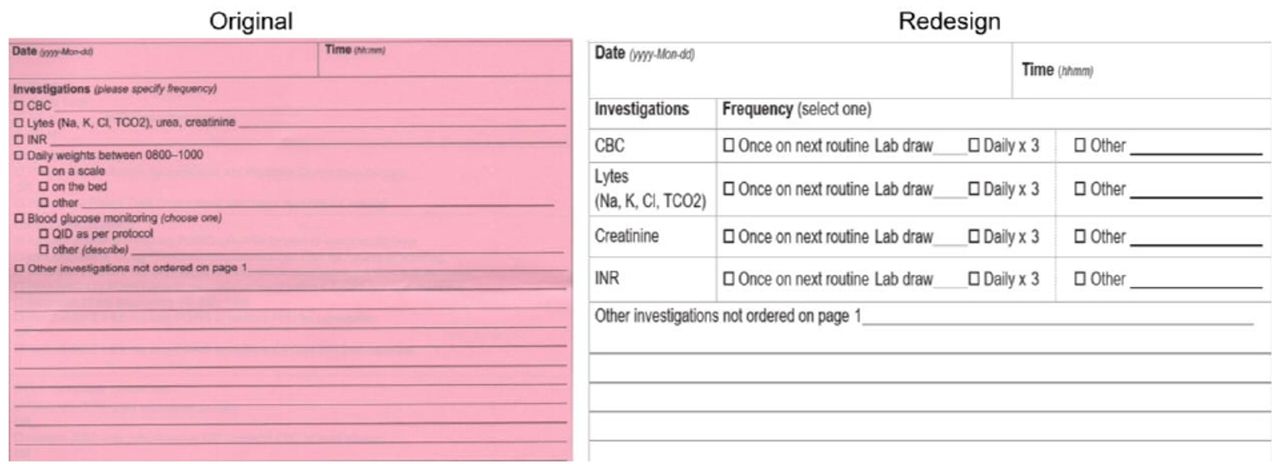
Medicine admission order form-laboratory section. The original admission order form-laboratory section compared to the redesigned admission order form laboratory section. The redesigned form, blood urea nitrogen/urea test is removed, frequency options included and a free text section maintaining physician ability to order any laboratory test required.
Measures
The Donabedian conceptual evaluation framework was used to examine the effect of order form redesign wherein a desired outcome is gained through the progression of structure and process.23 The outcome measure was the monthly count of BUN blood tests ordered for the GIM units at the two hospitals. The process measure was the percentage of updated medicine admission order forms used and the balancing measures were the number of ‘add on’ BUN tests, number of stat ordered BUN tests postpatient medicine unit admission, mortality and readmission rate. These balancing measures were selected to ensure that the proposed change intervention would not adversely impact laboratory workload and patient care.
A cumulative BUN monthly test order volume for the study units were provided by the provincial laboratory and placed in an Excel spreadsheet to facilitate data analysis. The monthly BUN volume for hospital A represents the total volume for the five GIM units and for hospital B represents the total volume for the six GIM units. To determine the usage of the updated medicine admission form (completed admission form located in the patient chart), a prospective chart audit of 50 charts per hospital GIM units was completed. To determine the number of add on or stat BUN tests, data were provided by the laboratory. Further, to determine the readmission and mortality rates, data were provided by the local health organisation.
Analysis
To analyse the findings for each study hospital, a comparison of the preintervention and postintervention BUN order volume average along with developing and interrupted time series (ITS) was completed.24 An ITS will allow for a series of observations on the same outcome before and after the introduction of an intervention to determine immediate and gradual effects of the intervention introduced at a specific point in time.25 Power calculations are difficult to complete, therefore a simulation study power calculation was used.26 For that reason, a total of 30 months (data points) with a minimum of 12 months preintervention of BUN order volume-count data for each hospital adult medicine units were collected preintervention, concurrent and postintervention. We base the ITS on Linden,27 Ramsay28 and on the Cochrane Review best practices.29 Statistical analysis was performed using STATA V.15.30 The basic strategy was to demonstrate the presence of autocorrelation in the time-series, and then model that time series with potential changes in intercept, and then in intercept and slope, before and after the intervention. If the changes are statistically significant, the time series was interrupted at the point of intervention, and the structural change would be interpreted either as a drop, or a drop with a changed slope, respectively.
Results
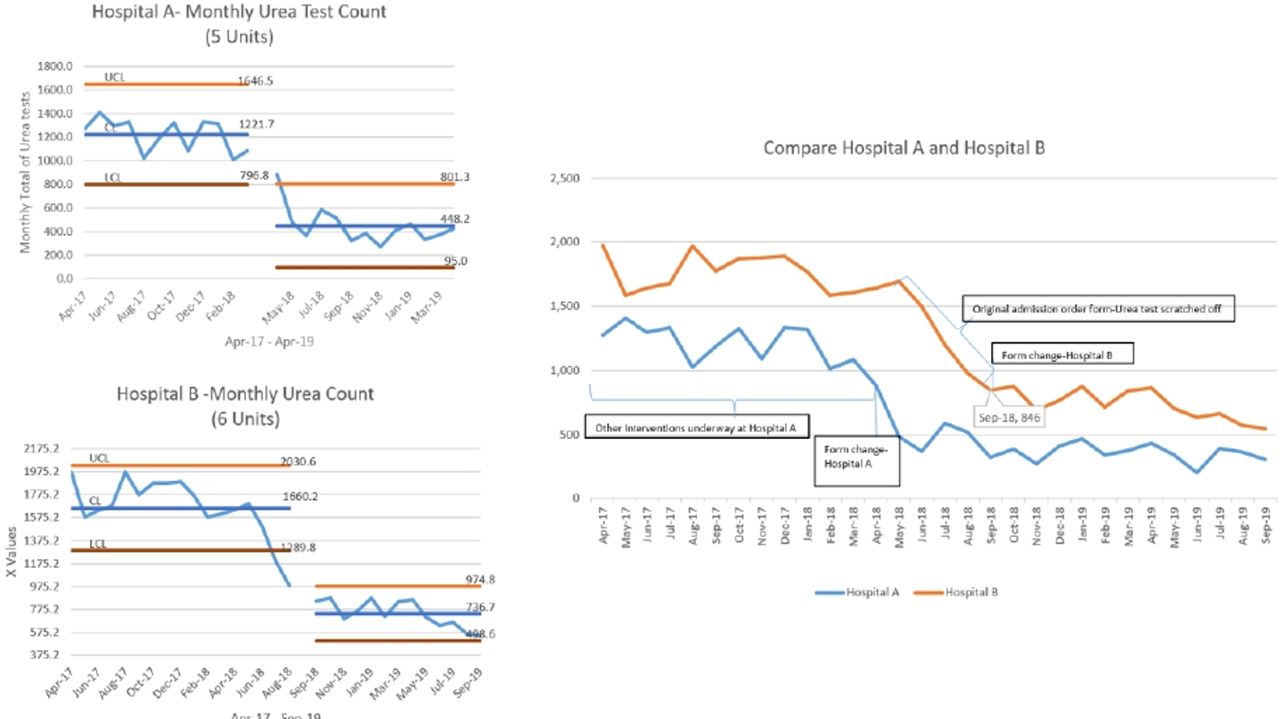
The average total monthly BUN test order decreased for hospital A, from 1221 to 448 and similarly for hospital B from 1660 to 736 over 17 months (figure 2). The annual BUN test collection and processing estimate cost for hospital A decreased from $73 260.00 to $26 880.00 a cost avoidance of $46 380.00. Similarly, for hospital B the estimate cost was reduced from $99 600.00 to $44 160.00 a cost avoidance of $55 440.00. The cost estimates were based on a referenced median cost of $5.00 per BUN test.20
{kind=link}
{kind=link}
Interrupted time series (ITS) graphs for hospital A and B and comparison graph. Hospital A and B ITS graphs illustrate the average total blood urea nitrogen (BUN) monthly order volume preorder and postorder form redesign implementation. For hospital A the total average order volume declined from 1221 to 448 BUN tests and for hospital B the total average order volume declined from 1660 to 736 BUN tests. The comparison graph illustrates similar downward trends for both hospitals during this time frame and that when hospital A implemented the form design the intervention effect was also noted at hospital B where the original form design was still in use. Allocation concealment was not possible as residents and attending physicians rotate between hospital A and B.
There is evidence of autocorrelation for both hospital A and B based on the Breusch-Godfrey statistical test. For both hospital A and B, using Newey-West standard errors for coefficients estimated by Ordinary least squares (OLS) regression the drop in intercept is statistically significant (hospital A, p value <0.001 and hospital B, p value=0.005), but the change in slope was not statistically significant for either hospital (p value=0.696 and p value=0.456). The data provide significant support for the hypothesis that the change in admission order form design coincided with a one-time drop in BUN monthly test orders, followed by a continuation of the longer-term trend. Statistical analysis provided in online supplemental file.
Supplemental material
The utilisation rate of the redesigned admission order form was found to be 100% following a random chart audit for both hospitals’ GIM units, enabling the continuation of physician laboratory test order practice change in these paper-based facilities. There was no add on or stat BUN test requests during the intervention time frame reported by the laboratory and there was no change in mortality and readmission rates.
Despite the staggered intervention start times, both hospitals exhibited similar downward trends suggesting unintended intervention spread. On closer examination of the audited charts for hospital B, postintervention start at hospital A, the BUN test was manually scratched off the original admission order form and the laboratory test order frequency had become time bound (ie, once or daily ×3) versus the preintervention frequency of daily. This may suggest that rotating residents and attending physicians’ individual laboratory test order behaviour change continued from one hospital to the next, despite not having the updated form. Further implying that hospital A previous interventions had some degree of effect on reducing BUN and laboratory test ordering frequency. Also, this could suggest the transfer of knowledge from residents and attending physicians further influencing other physicians at hospital B to change their laboratory test order behaviour.
Discussion
A QI intervention consisting of a medicine admission order form redesign was implemented with the goal of reducing BUN blood tests ordered in GIM wards in two Canadian teaching hospitals. This intervention had the advantage of being easy to implement and applicable to all the physicians on the GIM wards. The updated admission order form also required minimal education to have an influence on the physician’s ordering practice. We found that the updated admission form enables a sustainable reduction in laboratory tests seen in previous studies translated to BUN blood tests at these Canadian teaching hospitals.11–17 Additionally, because of the simplicity of the intervention implementation where the physician leaders communicated the rationale for the form update, the common pitfalls of completing a physician led QI project, that requires several hours of dedicated time for physicians to review the shortcomings of the current processes while simultaneously focusing on their clinical duties was avoided.31
The greater reductions experienced at hospital A compared with hospital B indicate that the additional interventions such as the targeted resident education, unit process changes alerting physicians of lab test order frequency and posted BUN clinical indication job aides that were in place at hospital A had a compounding effect. This coincides with previous knowledge that physician behaviour is best influenced by a multimodal approach.10 Therefore, hospital B will be incorporating the same additional intervention components in the near future to aid the sustained reduction of BUN test ordering and laboratory test order frequency. The main takeaway from this study is that admission order form design plays a critical role in habitual over ordering of the BUN test on hospital medicine admission sustaining local physician practice norms.
Limitations
With the rotation of residents and medical students between hospitals it was not possible for allocation concealment of the updated admission order form, thus, contamination was inevitable. Furthermore, the study occurred within the same city giving it a single local context and should be replicated elsewhere to determine transferability. Not only was this carried out in a single city but both locations were carried out at a teaching hospital wherein residents are known to unnecessarily order more frequently than hospitalists.7 Therefore the results may be different, or the methods require alterations, if carried out under different contexts.
Conclusions
Based on our findings, admission order form design can be extremely influential on physician laboratory test ordering behaviour change. Therefore, careful consideration should be given to the design of an admission order form to prevent unnecessary over ordering. Because our healthcare system is continually operated at its financial limits, order form changes could become a quick and effective way to maintain cost-effective care. Additionally, although the design of the order forms have an effect, this can be escalated with the addition of job aides that outline the clinical indications for specific laboratory tests, education or other context specific interventions that heighten physician awareness of laboratory test order frequency posthospital unit admission.
Implications
The notion that order form design can have an effect on physician ordering behaviour prompts an actionable response for sustainable healthcare. This most effectively occurs with collaboration between physicians, hospitals administrators, health organisations and laboratory leaders. Both paper order forms as well as computerised order systems can contribute to resource overuse and stewardship thus design of either should be carefully considered. With low value blood testing, design concepts in place, attaining financial accountability and resource stewardship may very well be possible.
Ethics statements
Ethics approval
Full ethical board approval was not required as our project was not conducted for research purposes but for organisational quality improvement.
Acknowledgments
The authors wish to acknowledge Alberta Precision Laboratory (APL) and the APL Data Analyst, Brent Knorr whose data support enabled the team to complete the study. Along with Alberta Health Services, University of Alberta Hospital and the Royal Alexandra Hospital Medicine Programmes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PM was responsible for conception and design of study, led-acquisition of data, analysis and drafting the manuscript. CB co-led drafting the manuscript. RH conducted the statistical data analysis and interpretation. YS and NK responsible for revising the manuscript critically for important intellectual content. All authors provided approval of the version of the manuscript to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.