Article Text

Statistics from Altmetric.com
- healthcare quality improvement
- diagnostic services
- emergency department
- evidence-based medicine
- unnecessary procedures
Introduction
First-episode psychosis (FEP) is a frequent presentation to hospital.1 Neuroimaging is often ordered during the initial assessment to facilitate diagnostic buy-in, mitigate medico-legal concerns, and maximise assessment in a patient population that is typically marginalised.2 3 These benefits, however, are outweighed by the unnecessary radiation, cost, and strong evidence that neuroimaging rarely yields actionable findings.2 3 This stance is evidenced in international guidelines2 3 and Choosing Wisely Canada (CWC) recommendations.4
Our site’s radiology department queried inconsistent (per guidelines) CT imaging in FEP, given requisition patterns. We undertook a quality improvement initiative to determine the prevalence of inconsistent imaging and study the effectiveness of an intervention aimed at improving recommendation adherence.
Methods
Data collection
All CT head studies with FEP-related indications performed at two local hospitals were identified through keyword searches of radiology reports containing any of the following terms: bizarre, delusion(s), delusional, hallucination(s), psychosis and psychotic. Extracted data included ordering physician specialty, provided indication, and imaging findings. Studies were classified as consistent or inconsistent with CWC guidelines.4 ‘Later-age of onset’, a CWC criterion for neuroimaging, is not defined by CWC and was chosen a priori to be age 40 years or more, based on local expert consensus and literature suggestions ranging from 35 to 50.2 3 5–8 Chart review was used to clarify history and imaging indications when ambiguous requisition information was provided. All ambiguous cases were settled through consensus (RS and RDH).
Pre-intervention data collection was performed retrospectively from January to June 2018 (6 months). Although a 6-month post-audit period would have been sufficient based off a predetermined sample size calculation, we expanded the post-intervention period to 12 months to assess the durability of findings.
Intervention
Following collection of baseline pre-audit data, multidisciplinary stakeholders were consulted to develop study priorities, design, and interventions. Engaged stakeholders included local experts in quality improvement and psychosis, and administrators and support staff of psychiatry and radiology departments. Identified priorities were to minimise workflow disruption and study-specific administrative burden. Stakeholder and literature evidence suggested the combination of audit and feedback with education, and separately visual prompts, could be successful in effecting change.9 From these considerations, we created a one-page infographic incorporating pre-intervention audit results and CWC guidelines (see online supplemental file 1), which was then emailed by department heads to high yield physician groups (emergency and psychiatry physicians) and physically posted throughout physician workspaces (walls and doors).
Supplemental material
Data analysis
Basic descriptive and inferential statistics are reported. A Cochran-Mantel-Haenszel test was applied to a series of 2×2 contingency tables stratified by specialty, which compared consistent and inconsistent orders in the pre-audit and post-audit. The odds of ordering an inconsistent scan (outcome) in the post-intervention period (exposed group), relative to the pre-intervention period (reference) were estimated. Odds ratios (ORs) are reported with 95% confidence intervals (CIs). All analysis was two-sided, and significance set at p<0.05. Analysis was conducted on SAS Enterprise Guide V.7.1 and R Studio V.12.1.
Results
Patient and ordering physician characteristics
Pre-intervention and post-intervention audits yielded 60 and 83 FEP cases, respectively. The mean age for the entire cohort was 44 (standard deviation 18.6, range 17–100). Sixty-one (43%) of patients were women. Psychiatrists and emergency physicians ordered the vast majority of CT scans during both pre-intervention (97%) and post-intervention (92%) periods.
Indications for head imaging and yield
Among pre-intervention cases (n=60), ‘later-age of onset’ was the most frequently cited valid indication (n=22, 37%) for head imaging. Other valid indications included ‘other’ (n=8, 13%), ‘headache’ (n=5, 8%), ‘atypical psychosis features’ (n=4, 7%), ‘nausea or vomiting’ (n=2, 3%), and ‘seizure-like activity’ (n=1, 2%). A greater proportion of post-intervention cases were due to ‘later-age of onset’ (n=51, 61%). Other valid indications post-intervention were ‘atypical psychosis features’ (n=17, 20%), ‘query autoimmune encephalitis’ (n=3, 4%), ‘headache’ (n=4, 5%), ‘seizure-like activity’ (n=1, 1%), ‘nausea or vomiting’ (n=1, 1%), and ‘other’ (n=11, 13%).
No structural cause for psychosis was identified in any CT study within this project.
Intervention effectiveness
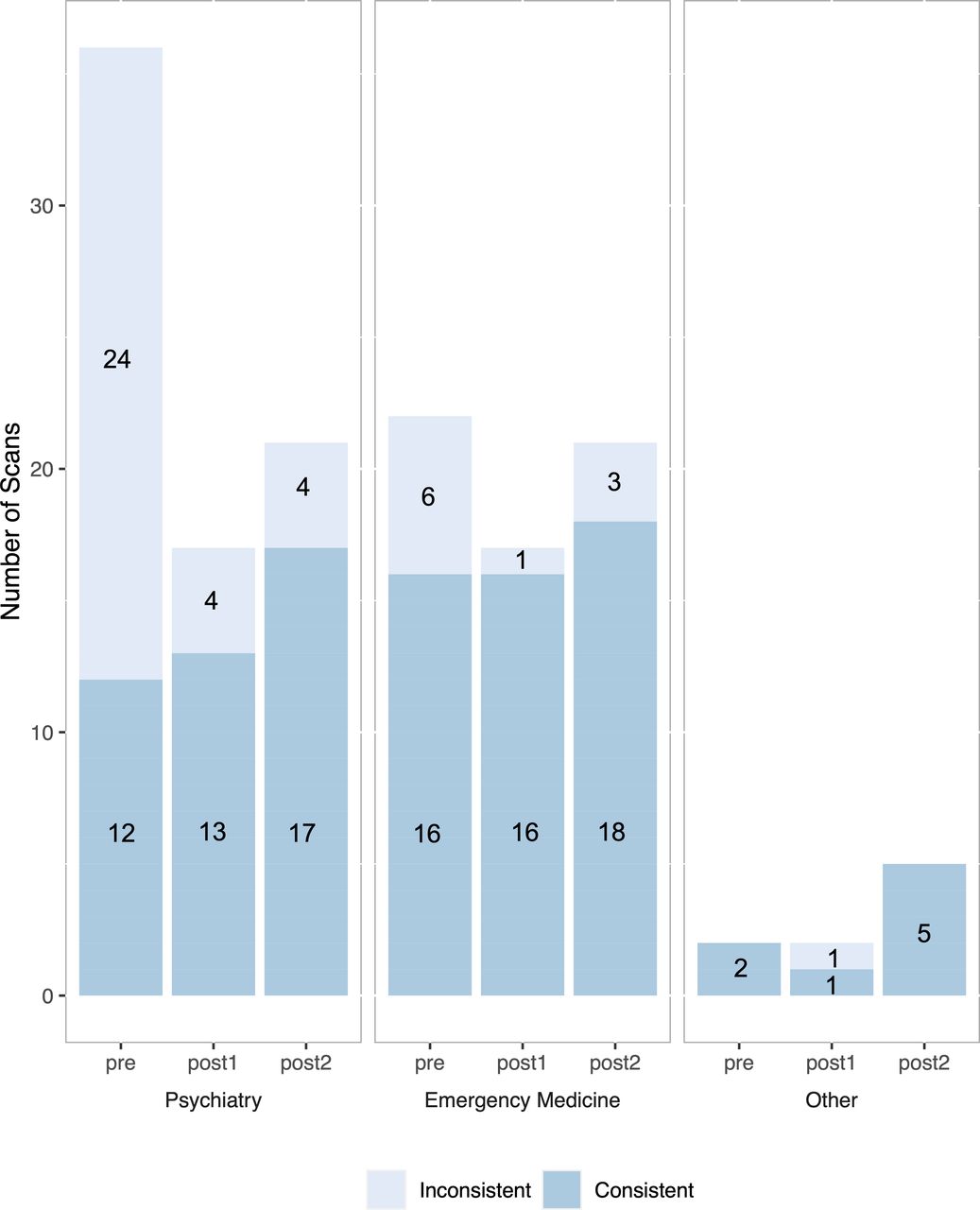
There was a significant decrease in the proportion of inconsistent CT studies from 50% to 16% post-intervention (OR 0.2; 95% CI 0.09 to 0.44, p<0.01). When the 12-month post-intervention period is divided into two 6-month blocks (‘post1’ and ‘post2’), similar reductions are observed (17% and 15%, respectively). Figure 1 demonstrates the number of consistent and inconsistent scans in the pre-audit and post-audits, stratified by physician specialty.

{kind=link}
Summary of CT scans performed for first-episode psychosis during the pre-intervention (pre), first 6 months of post-intervention (post1), and second 6 months of post-intervention (post2) periods, stratified by ordering physician specialty. Chart bars are divided according to consistency with Choosing Wisely Canada recommendations into either consistent (dark blue) or inconsistent (light blue) scans.
Discussion
An audit of CT usage in FEP was conducted at two local institutions before and after implementing an intervention of feedback, education, and visual prompting, which aimed to align ordering practices with guideline recommendations. Psychiatrists and emergency physicians were responsible for the majority of requests and were most directly targeted.
Our study suggests that infographics can be used to decrease CT scans inconsistent with CWC recommendations, in patients with FEP. Post intervention, the 6-month rate of inconsistent CT head requests decreased from 50% to 17% and 15% (at 6 months and 12 months, respectively). This outcome is highly relevant in healthcare, where a limited capacity to modify workflows is a near ubiquitous constraint. Although passive educational methods receive criticism for their ineffectiveness,10 a growing body of literature supports this and our other interventions. A recent study found that among reviewed initiatives with sustained results, each of our three strategies—audit and feedback, education, and reminders—were present.11 A 2017 systematic review found that provider education, performance feedback, and multicomponent interventions all have strong evidence for reducing low-value health services.12 Most recently, a similar education and feedback intervention was shown to durably reduce cardiac echocardiograms.13 Critical to our success was our team, multicomponent approach, and visual prompts. Engaging multidisciplinary stakeholders, including our target clinician groups, led to practical insights for optimising the intervention approach. Our intervention also likely benefited from synergistic effects associated with using several evidence-based approaches together, and clear and consistent reminders achieved with the physical placement of cues in the work environment.
The results of our initiative also lend further support to evidence-based guidelines3 14 15 indicating CT imaging for FEP provides minimal utility; no explanatory intracranial abnormality was identified during the pre-intervention or post-intervention audits.
Several limitations merit discussion. By prioritising minimal workflow disturbance over obtaining process measures, we cannot firmly establish a link between our intervention and results, nor could we run successive Plan Do Study Act (PDSA) cycles to optimise interventions. Calendar-year timing differences between audits may also impact results. Finally, while our preference would have been to display the data in a run chart format,16 our dichotomous outcome and insufficient number of observations precluded its usage.
Conclusions
Reducing guideline-inconsistent testing may be achieved through infographics employing minimally-invasive feedback mechanisms (audit and feedback, education, and reminders) with visual prompts in physical spaces.
CT neuroimaging has a limited role in FEP and we recommend following CWC recommendations. Future studies should aim to identify a specific age with which to define the ‘later-age of onset’ criterion.
Ethics statements
Ethics approval
The radiology department pursued this initiative for organisational quality improvement. Guidance from the University of British Columbia’s Behavioral Research Ethics Board (IRB equivalent in Canada) deemed this type of initiative as falling under QI ethics exemption under Article 2.5 of the 2018 Tri-Council Policy Statement. Results are presented anonymously and in aggregate to minimise re-identification risk.
Acknowledgments
Dr Michael A Irvine from the Clinical Research Support Unit, BC Children’s Hospital Research Institute for his assistance with statistical analysis approaches for the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
RS and RDH contributed equally.
Contributors RS, RDH, JS and TL designed and conducted the quality improvement project and performed the intervention. RS and RDH conducted data acquisition. RS, RDH and CN performed data analysis, data interpretation and manuscript preparation, with important intellectual input from TL and JS. All authors approve of the final version of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement statement Patients and members of the public were not involved in the performance of this quality initiative.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.