Article Text

Abstract
Background and objectives Despite the American College of Emergency Physicians and American Academy of Pediatrics recommendations for standardised handoffs in the emergency department (ED), few EDs have an established tool. Our aim was to improve the quality of handoffs in the ED by establishing compliance with the I-PASS handoff tool.
Methods This is a quality improvement (QI) initiative to standardise handoffs in a large academic paediatric ED. Following review of the literature and focus groups with key stakeholders, I-PASS was selected and modified to fit departmental needs. Implementation throughPlan–Do–Study–Act cycles included the development of educational materials, reminders and real-time feedback. Required use of I-PASS during designated team sign-out began in June 2016. Compliance with the handoff tool and handoff deficiencies was measured through observations by faculty trained in I-PASS. As a balancing measure, time to complete handoff was monitored and compared with preintervention data.
Results Compliance with I-PASS reached 80% within 6 months, 100% within 7 months and sustained at 100% during the remainder of the study period. The average percent of omissions of crucial information per handoff declined to 8.3%, which was a 53% decrease. Average percentage of tangential information and miscommunications per handoff did not show a decline. The average handoff took 20 min, which did not differ from the preintervention time. Survey results demonstrated a perceived improvement in patient safety through closed-loop communication, clear action lists and contingency planning and proper patient acuity identification.
Conclusions I-PASS is applicable in the ED and can be successfully implemented through QI methodology contributing to an overall culture of safety.
- quality improvement
- hand-off
- emergency department
- communication
- patient safety
Data availability statement
All data relevant to the study are included int he article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Miscommunications and omissions during handoffs are a leading cause of medical errors.1–7 In 2006, The Joint Commission established a requirement to implement a standardised handoff approach.8 9 Since that time, the Quality Improvement and Patient Safety Section of the American College of Emergency Physicians as well as the American Academy of Pediatrics has identified the standardisation of handoffs as a target for improving patient safety in all settings including the emergency department (ED).10–12 Through a multicentre collaboration, the I-PASS handoff tool was developed based on materials adapted from TeamSTEPPS, the evidence-based medicine curriculum developed by the Agency for Healthcare Research and Quality and the Department of Defence Patient Safety Programme.13–16 This tool, focusing on resident handoffs, has demonstrated improved patient safety in the inpatient setting.17
While the standardisation of handoffs has been a focus for inpatient settings, few studies have looked at this in the ED setting where shift changes often lead to multiple handoffs between providers with varying levels of training.13 14 In a survey of 147 emergency medicine (EM) residency programme directors and academic EM faculty in 2011, over half indicated that their ED does not use a standardised handoff protocol. Among the programmes that did have a protocol, most of the residents did not use them regularly.18 The few studies that have evaluated the use of standardised checklists in the ED setting have shown reduced omission of key information and improved ED situational awareness without increasing time of check out.19 20 Literature reviewing crucial elements for successful ED handoffs has been in line with key components of the I-PASS handoff tool.12 21 However, the few studies evaluating the use of I-PASS specifically in the ED setting were performed qualitatively and focused on the feasibility of implementation.21–23 While these studies showed that I-PASS may be feasible in the ED, there are no current reports of successful implementation.
Prior to our intervention, there was no standardised approach to patient handoffs in our paediatric ED, and there was great variability among providers. Our aim was to improve the quality of handoffs during team sign-outs in the ED by establishing proper utilisation and compliance with a modified I-PASS handoff tool for 0%–80% in a 6-month period. Secondary aims were to decrease omissions of critical patient information and handoff miscommunications by 50%.
Methods
This quality improvement (QI) initiative was implemented at a quaternary paediatric ED with a level I trauma centre, with an average ED yearly patient census of 80 000. The main ED, where the project was implemented, consists of 25 beds including two resuscitation beds. All patients are seen by a paediatric emergency medicine (PEM) attending but also may be seen by medical students, paediatric residents, EM residents and PEM fellows. Both group and individual handoffs occur between physicians. Phase one of this initiative focused on large group handoffs during resident shift change (occurring at 06:00, 16:00 and 02:00) where a structured process including a prehandoff checklist already existed.20 Each group handoff typically consisted of eight to ≥15 providers that included: 0–4 medical students, 4–8 paediatric residents, 0–3 EM residents, 0–3 PEM fellows, 0–2 general paediatricians who work in the ED, 0–1 advanced practice providers (nurse practitioners and physician assistants), 2–3 PEM attendings and 1–2 charge nurses.
Intervention
In June 2015, a team of healthcare providers began meeting monthly to determine best practice for successful implementation of a standardised handoff process in the ED. The team consisted of a paediatric hospitalist trained in QI methodology and I-PASS, a QI expert and PEM physician and five PEM physician leaders. These meetings identified four key drivers for successful ED handoff standardisation including (1) selection and modification of the I-PASS handoff tool, (2) ED provider education, (3) buy-in from key stakeholders and (4) accountability of participants. Implementation of the modified I-PASS tool for the ED occurred through Plan–Do–Study–Act (PDSA) cycles with focus on key drivers (figure 1).

Key driver diagram. MOC, Maintenance of Certification; QI, quality improvement.
To determine the best handoff tool for the ED, the literature was reviewed, and focus groups were conducted with key stakeholders including ED nurses, PEM faculty, PEM fellows, EM residents and paediatric residents to determine key components of handoffs within the ED. Based on consensus agreement, the I-PASS handoff tool was selected.22 24 Slight modifications were made to emphasise components of the patient summary, prioritise disposition and further define illness severity in the context of the ED (figure 2).

Components of the I-PASS handoff tool. **Highlighted portions represent emphasised components and modifications to fit emergency department (ED) needs. CC, chief complaint; PHM, past medical history; PSH, past surgical history.
Education of providers on I-PASS occurred in multiple ways and was modified as the project matured. Paediatric residents in the ED were familiar with I-PASS as it was the standard handoff tool used on the paediatric hospital medicine service. All paediatric residents had received I-PASS training during their intern orientation. The training was initially 3 hours in length but was modified to a 1 hour class, which made it more feasible for widespread expansion. In order to address the slight modifications made to the I-PASS tool for the ED and address education for faculty, fellows and rotating EM residents, a 30-minute online PowerPoint presentation on I-PASS was developed and placed on Moodle, an online learning management system. Online learning was chosen to allow residents easy access to the material and give them time to view the presentation on their own time prior to starting their rotation. The materials were made available to all residents (at the start of their rotation), PEM fellows and PEM faculty through email notification and consisted of a basic breakdown of the I-PASS handoff tool, what ED-specific modifications were made, specific video examples on how to use I-PASS and the expectation of providers to use I-PASS during handoffs in the ED. To ensure completion by first-time rotators at our institution, EM residents were given protected time during their ED orientation to complete the educational material. Education was also provided to PEM faculty and PEM fellows at section meetings and through email reminders. Faculty members performing observations also completed observation training through a separate interactive module that required scoring of handoffs using standardised video examples followed by expert feedback.
To establish buy-in and promote accountability among providers, ED leadership and senior quality leadership were engaged from the beginning of the process. In addition, ED I-PASS champions were identified to encourage I-PASS usage during all handoffs in the ED. Regular communication to all ED providers (faculty, fellows, nurse practitioners, physician assistants and residents) occurred through emails, educational sessions at sectional meetings stressing the success of I-PASS in the inpatient setting, I-PASS poster placement in ED work areas and distribution of badge cards. Providers were reminded to use the I-PASS handoff tool immediately prior to every group handoff as part of the sign-out checklist.20
Following the availability of education materials on 27 May 2016, required use of I-PASS during group handoffs began on 1 June 2016. Resident handoffs were observed and evaluated by faculty trained in the I-PASS handoff tool and on the use of an established observation form developed by the I-PASS Institute.25 Because this was a QI initiative, blinding was not necessary, and residents giving and receiving handoff were reminded to use I-PASS and given feedback on their handoffs during group handoffs. To encourage regular observations of group handoffs, faculty providers who performed observations were offered Maintenance of Certification (MOC) Part 4 credit.26
Study of the intervention
We observed and documented group handoffs from February 2016 to February 2017, with the first 4 months as preintervention baseline data and the last 9 months accounting for the intervention study period. To assess sustainability, we reviewed data following subsequent PDSAs that expanded the project to include hospital-wide implementation. ED compliance with I-PASS for this data was reviewed from March 2017-December 2017.
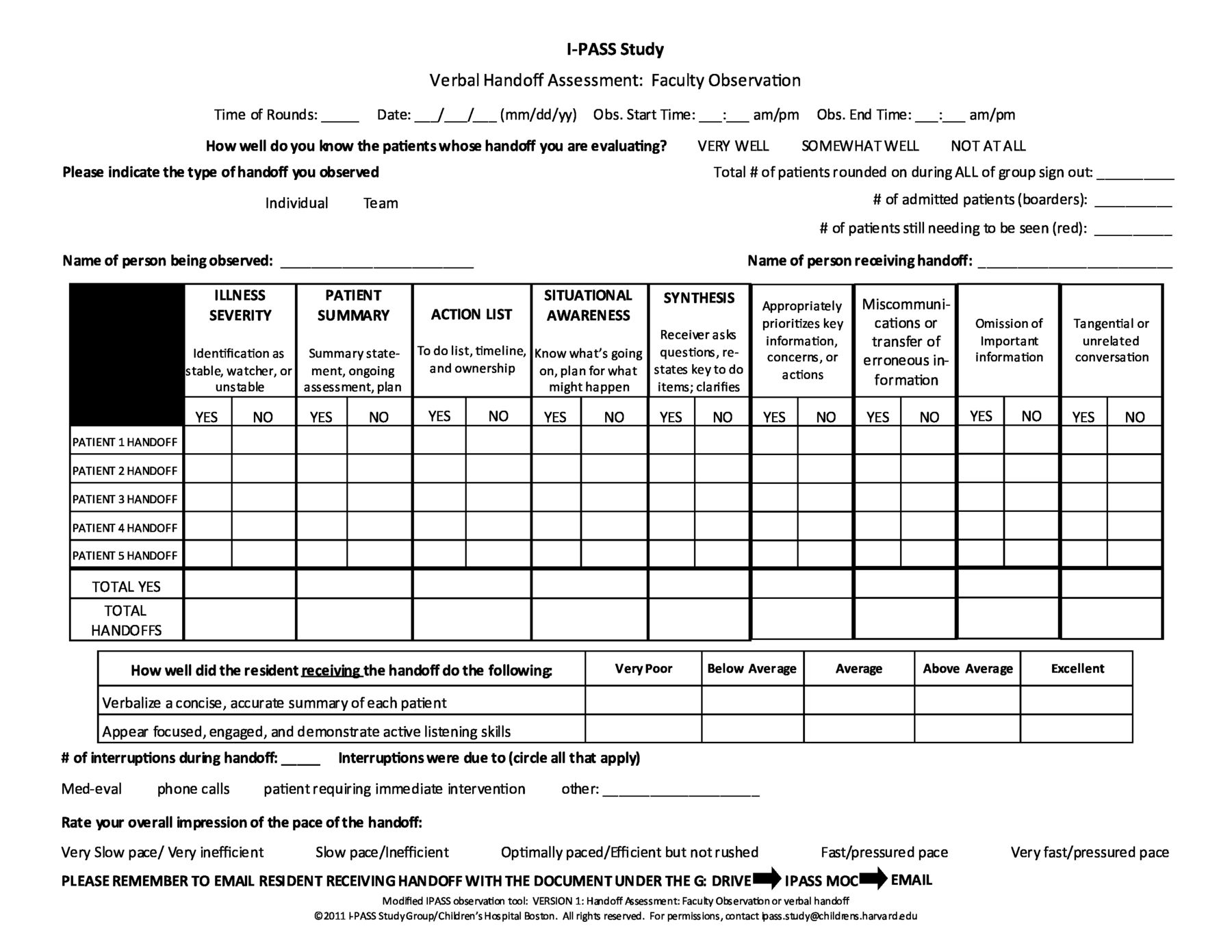
Faculty observers would select one resident handoff to observe during the group sign-out. Individual (single provider to provider) handoffs occurring outside of the designated group sign-out were excluded during this phase of the project. Observations were done by trained faculty using an I-PASS observation form developed by the I-PASS Institute (version 1 figure 3).25 This form used a Likert Scale to assess a resident’s overall handoff (multiple patient handoffs during one group sign-out).

Observation Tool: Version 1 (V1)
Initial feedback during baseline observations revealed that the observation form was difficult to use and too subjective despite the video training. Therefore, in July 2016, the project team made modifications to the observation form to improve objectivity and usability. Consensus agreement led to the revised form (version 2 (V2) figure 4), and the video training was updated to reflect the changes. The V2 form was made available for observations 23 August 2016.
Observation Tool: Version 2 (V2)
Observations occurred via convenience sampling when faculty observers were available during both clinical and non-clinical time. Observation forms were made available in the group handoff work area. Following the observation, faculty observers were required to input their results in a shared Microsoft Access programme for future data analysis.
To assess attitudes towards the intervention, a one-time preintervention and postintervention survey was sent out via email to faculty, fellows and residents after implementation. This survey consisted of a Likert Scale (strongly disagree, disagree, neutral, agree and strongly agree), and percentages were calculated as a sum of agree and strongly agree for each question.
Measures
The primary measure was to reach 80% compliance with the I-PASS handoff tool during group sign-out within a 6-month period. Compliance was defined as correctly using the components of I-PASS in each sign-out session. Data were analysed monthly and discussed among project participants to identify barriers and areas for improvement.
To further assess handoff standardisation’s impact on patient safety, percentage of handoffs with omission of key information, miscommunications and tangential information was evaluated as outcome measures. Omissions were defined as any information necessary to adequately provide patient care that had to be added by a supervisor during handoff. Miscommunications were defined by any need for clarity or correction by a supervisor during handoff, and tangential information was considered if topics unrelated to the patient were discussed.
As a balance measure, time to complete group sign-out was monitored and compared with prior data (table 1).
Project QI Measures
Analysis
We measured the success of our intervention through traditional QI methods and descriptive statistics. Prior to the development of the V2 observation form, the modified Likert Scale developed by the I-PASS Institute was used, and percentages were calculated.
In August 2016, the revised observation form (V2) was finalised and used for all subsequent data collection. The observation form was iteratively changed from percentage ranking to categorical for ease of use and accuracy. Compliance was calculated by taking the mean of total yeses over the total number of handoffs for each specific component of I-PASS. Any handoff that had a mean of 90% or more was considered compliant.
To follow changes over time, percentage of compliant handoffs was compared monthly during the study period and plotted on a run chart with our aim documented in a horizontal line and times of interventions plotted for reference. Sustainability data were plotted in the same manner.
Deficiencies in handoffs including omissions, tangential conversations and miscommunications were tracked, and totals were calculated on a month-to-month basis during the study period as well. Time to complete handoffs was also documented as nominal values and plotted over time as individual data points on a run chart. Descriptive statistics were used to analyse attitudes.
Ethical considerations
The Institutional Review Board for the Protection of Human Subjects determined the project to be exempt from review as QI.
Results
Fourteen faculty providers participated in observations of handoffs. From February 2016 to February 2017, there were a total of 202 observations, of which 198 were used for data collection and four were excluded due to missing data. Of the 198 observations, 18 (9%) served as baseline or preintervention data and 180 (91%) as the postintervention study period. The average number of patients handed off per resident handoff was three (range 1–5, with 4–8 residents per sign-out). Variability with regard to total number of observations per month occurred with a substantial drop off in December, likely attributed to convenience sampling with decreased observer availability and increased census.
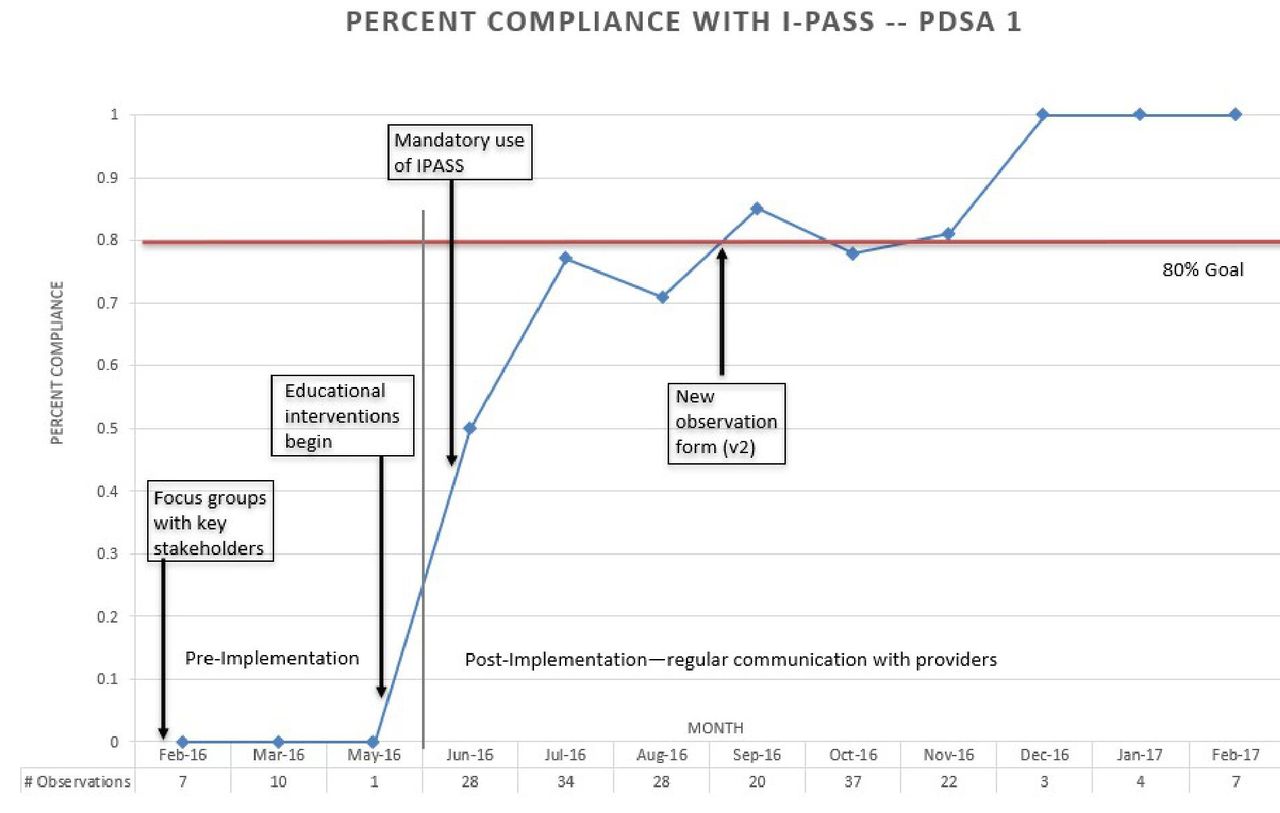
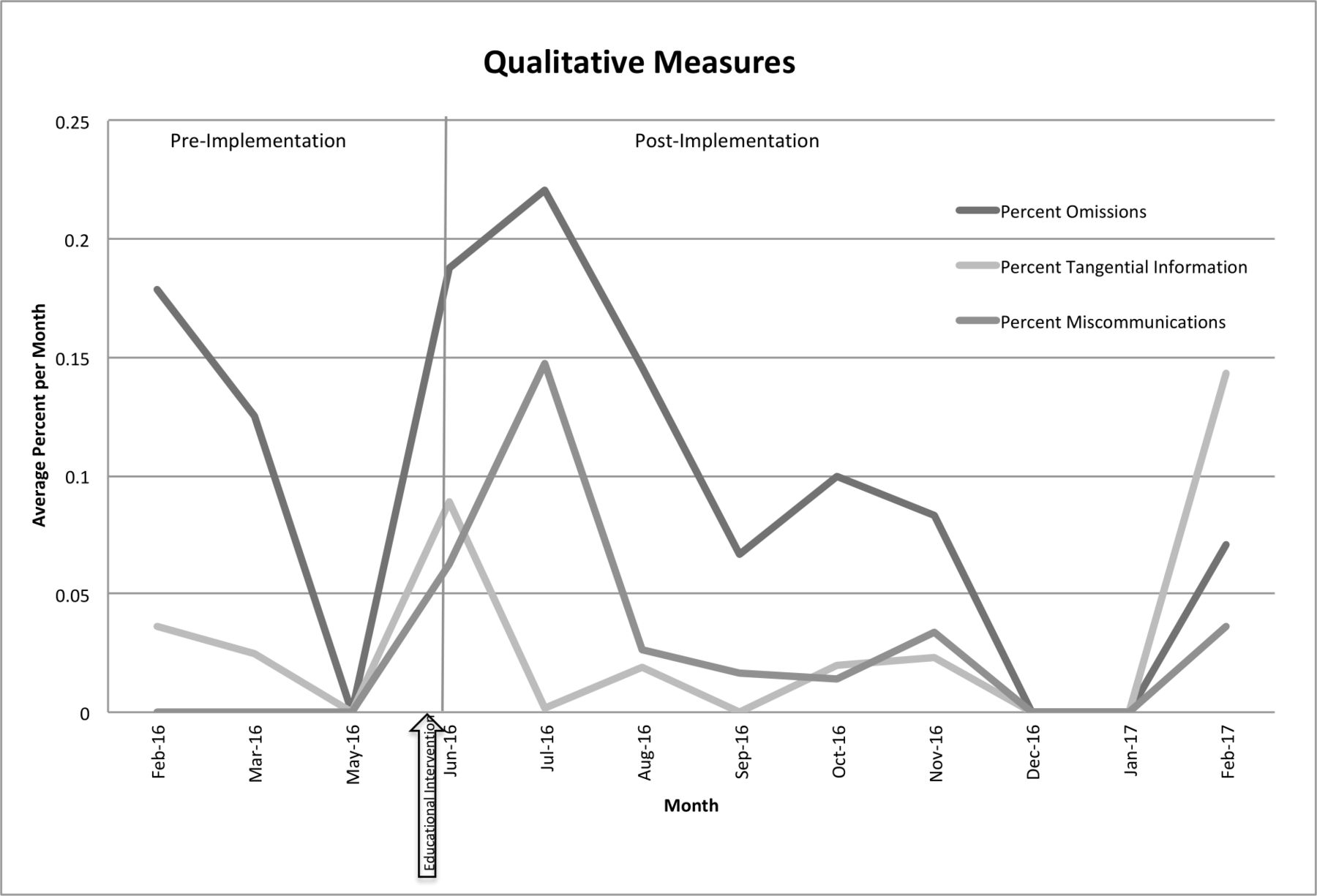
Preintervention data (from February 2016 to May 2016) showed that 0% of handoffs were compliant with the I-PASS handoff tool. The percent omissions of crucial information per handoff ranged from 12% to 18%, tangential information ranged from 2.5% to 3.6% and miscommunications were not identified in this sample. Following stepwise implementation, including education (27 May 2016), poster placement, email reminders and the initiation of observations (1 June 2016), compliance with the I-PASS handoff tool steadily improved on a monthly basis, reaching 80% compliance within 6 months, 100% within 7 months and sustaining at 100% compliance during the remainder of the study period (figure 5). The average percent of omissions of crucial information per handoff had a steady decline as well from 18% to 8.3% during the final month of the study period, which was a decrease of 53%. Average percentage of tangential information as well as percent of miscommunications per handoff did not show a steady decline and averaged 3% and 3.8%, respectively, over the study period (figure 6). With regard to our balance measure, the average length of handoffs was 20 min, which did not differ from the preintervention time to complete handoffs noted in a previous study.20
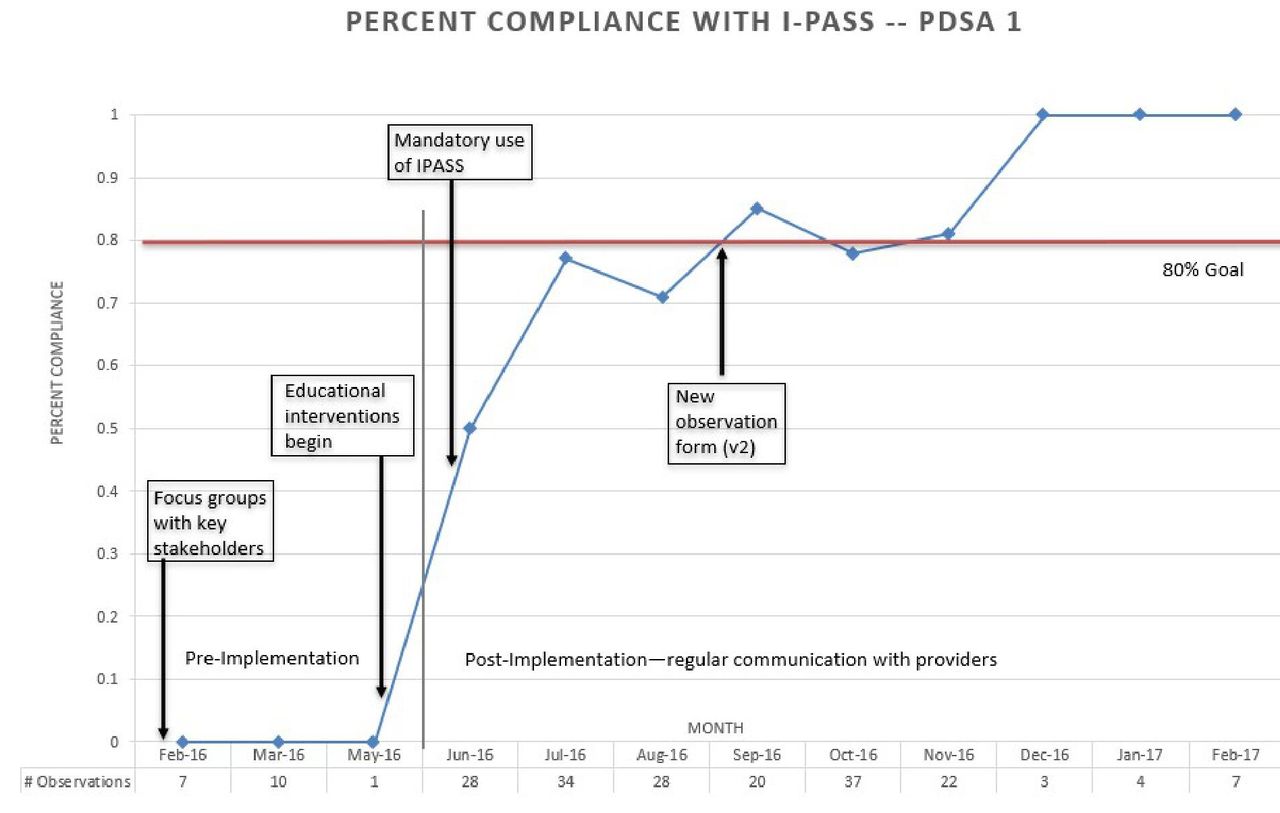
Run chart: Compliance with I-PASS use during group sign-out from February 2016 to February 2017. PDSA, Plan–Do–Study–Act; v2, version 2.
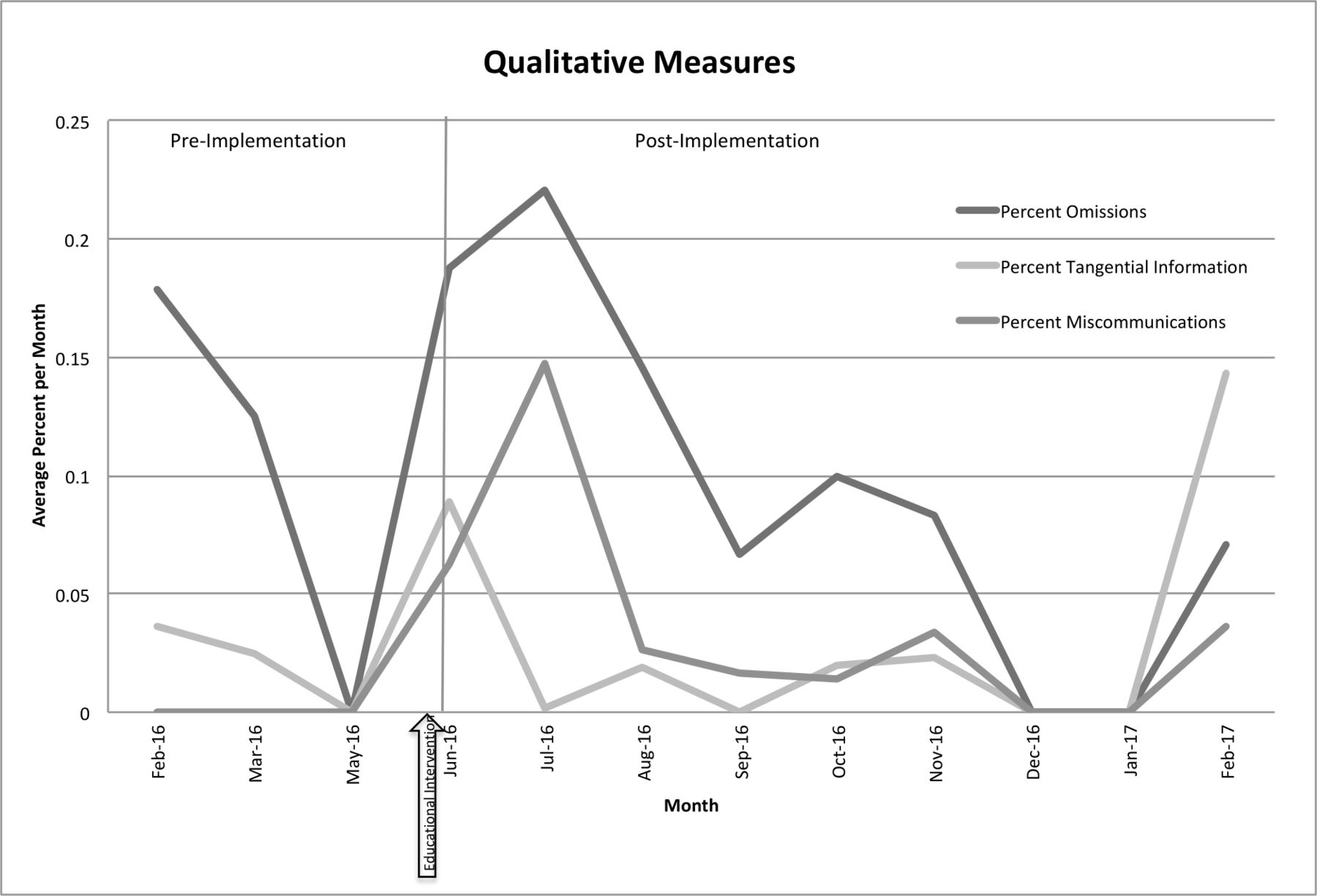
Run chart: handoff deficiencies during group sign-out from February 2016 to February 2017.
To assess sustainability, compliance in the ED following hospital-wide implementation of I-PASS was reviewed from March 2018 to December 2018. Data from this period showed an initial decline in compliance to 40% in March as well as a decline during the month of July to 30%, likely due to the start of new residents and fellows. With further required interactive educational workshops for hospital-wide faculty and fellows and a resurge of observations, there was a steady increase in compliance to our initial aim of 80% by November 2017 (figure 7).
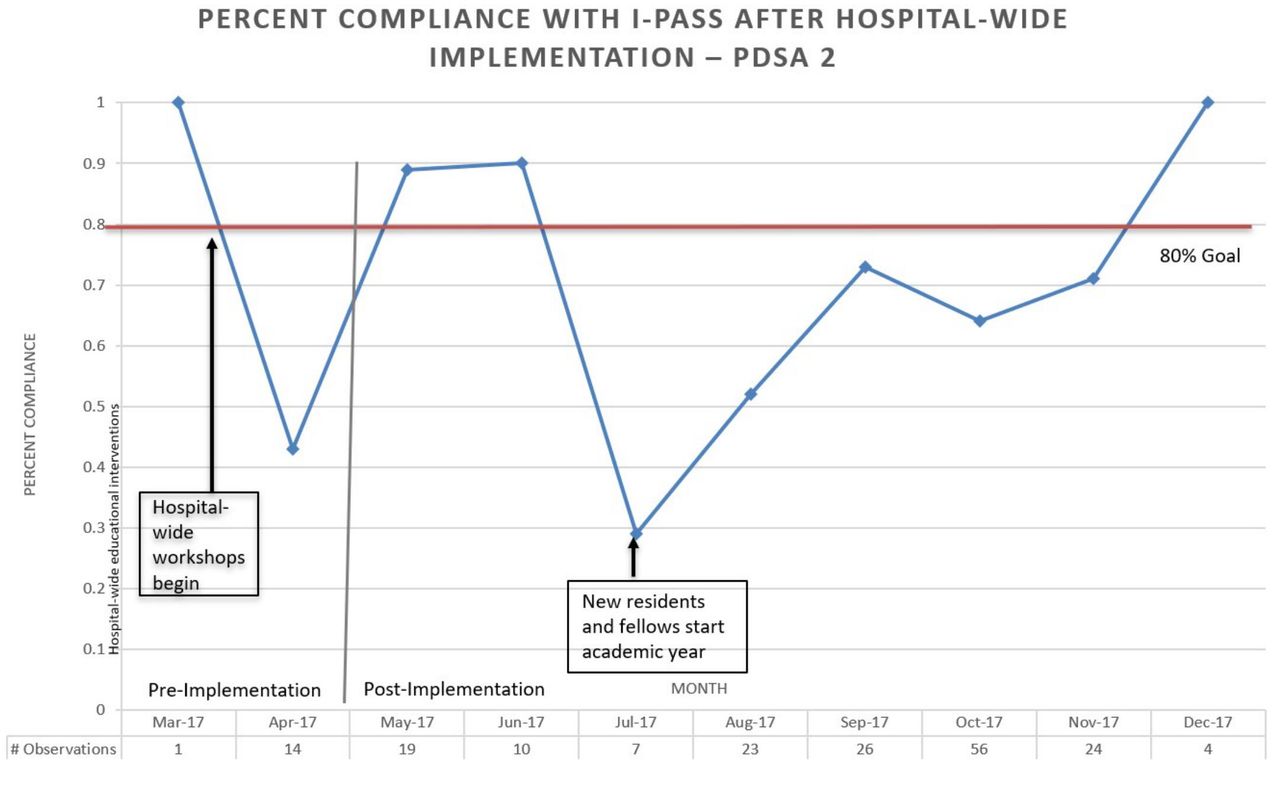
Run chart: postimplementation I-PASS compliance following hospital-wide implementation (results specific to paediatric emergency department). PDSA, Plan–Do–Study–Act.
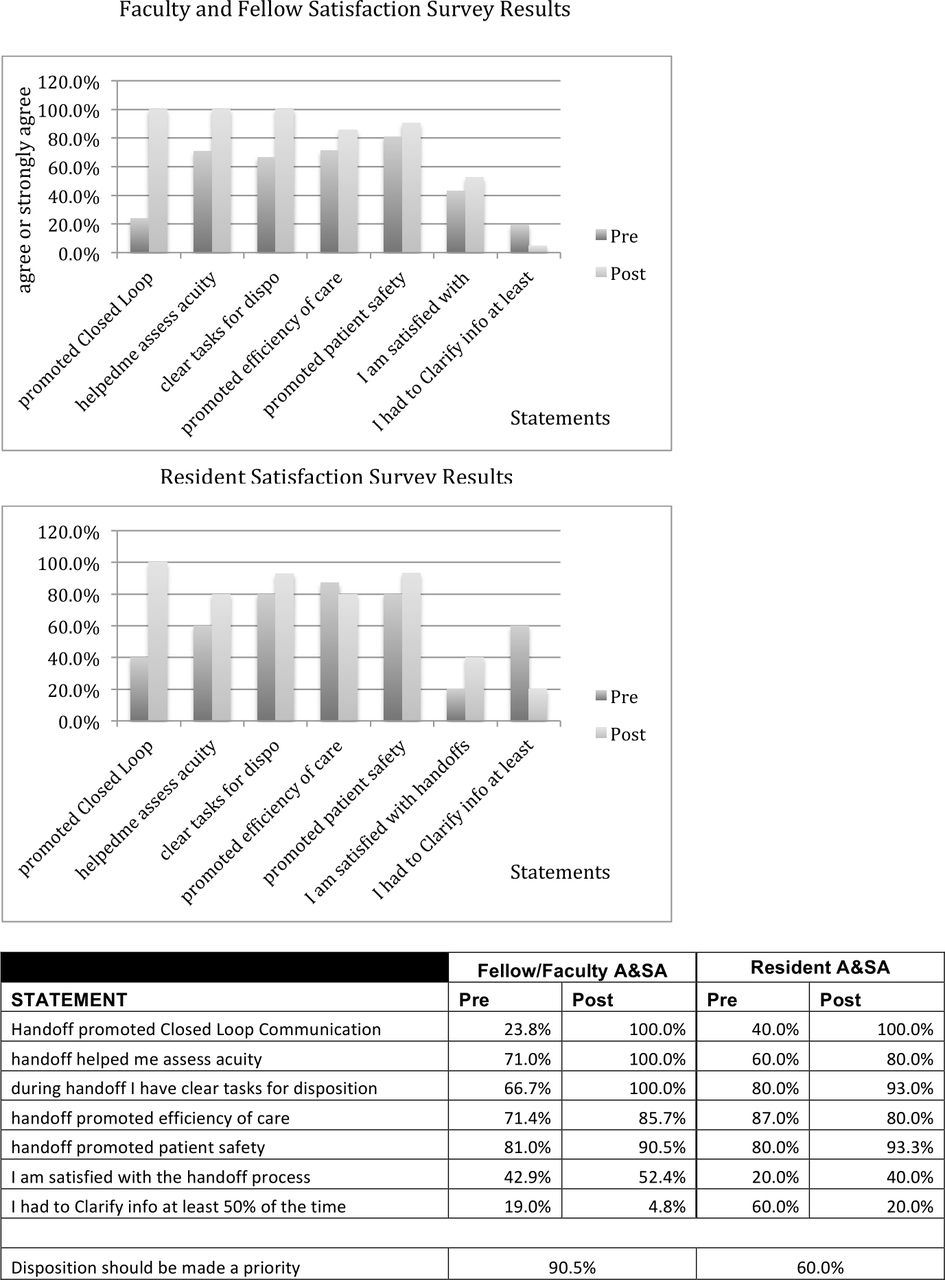
The preintervention and postintervention survey, sent out in January 2017, had 36 responses with an overall response rate of 23% made up of 15% residents (15 responses) and 36% faculty and fellows (21 responses). Results showed that providers felt I-PASS handoff promoted closed-loop communication, allowed for proper assessment of patient acuity, provided clear action lists to disposition patients and promoted patient safety (figure 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Provider preintervention and postintervention perception survey results for residents and faculty/fellows.
Discussion
Although the I-PASS handoff tool was developed for the inpatient setting, we were able to demonstrate its applicability to the ED setting and met our aim of 80% proper use of the I-PASS handoff tool during group handoffs with sustainable results. Observations demonstrated a decrease in the percent of omissions per handoff by 50%, but we did not see any significant change in the percent of handoffs with tangential information or miscommunications. Despite provider perceived changes in timeliness using I-PASS during group handoffs (survey 1), the time to complete sign-out did not change and remained as an average time of 20 min. Additionally, faculty feedback revealed that providers noticed residents no longer repeating handoffs again after group handoff, thus improving overall efficiency. Although not conclusive due to low response rates, survey results did reveal a perceived improvement in communication, patient prioritisation and task management. A perception of improved patient safety likely played a crucial role in our ability to change culture within the ED, a necessary key driver in any QI initiative.
Successful implementation and maintenance of I-PASS in the ED were highly attributed to the buy-in by key ED and QI stakeholders, as well as the accountability that inevitably comes into play when one is being observed. Faculty members and PEM fellows held residents accountable for using I-PASS and were able to use the sign-out sessions as an opportunity for education and real-time feedback.27 Additionally, the offering of MOC Part 4 was an important factor to further incentivise faculty participation in observations. This also allowed for regular group feedback sessions to identify barriers, determine areas for interventions and provide internal support of our efforts.
Using I-PASS in the ED is impactful in multiple ways. Given that The Joint Commission identified standardisations of sign-out procedures as a 2008 National Patient Safety Goal as well as the ED’s vulnerability to medical errors during transfer of care, a standardised approach to handoffs in the ED was overdue.9 12 28 The I-PASS collaborative’s successful implementation in multiple settings, proven improvement of patient safety and structure made it ideal for the ED.9 14 17 Through our initiative, we demonstrate that I-PASS can be a useful tool in the ED, contributing to a culture of safety and improving communication.
Limitations
We encountered limitations while implementing this study in our ED. Enforcing faculty and fellow education on I-PASS with an online module was difficult, a recognised limitation of online education.29 Additionally, despite our desire to survey residents on specific safety events related to handoffs, these events were rarely reported, likely out of fear of adverse consequences or a lack of ease with the reporting process.30–32 Initial efforts also hoped to follow time to disposition as a potential outcome measure, but this was confounded when other factors, including the hours expansion of an onsite urgent care centre in August 2016 that made it difficult to isolate handoffs as a causal source for time to disposition. While modification of the observation tool greatly improved ease of use for observers, the change made statistical evaluations of predata and postdata difficult.
Future directions
Since the implementation in the ED, with the help of institutional QI leadership, grant funding and the I-PASS Institute, hospital-wide implementation of I-PASS has occurred throughout our paediatric, surgical, anaesthesia and obstetrics/gynaecology departments. Lessons learnt from this QI initiative have driven the success of hospital-wide implementation and include the continued offering of MOC Part 4, multiple education modalities, gaining early support from local QI leadership and using observation sessions as an opportunity for teaching, reinforcement and accountability. Future directions for I-PASS use within the ED hope to focus on individual handoffs at the bedside to encourage patient and public participation, as well as ED to inpatient transfers.
Conclusions
I-PASS is an applicable tool for handoffs in the ED and contributes to a perceived culture of safety through QI methodology. Successful implementation is highly dependent on diversifying educational modalities, key stakeholder support, personal accountability and incentivising participants.
Data availability statement
All data relevant to the study are included int he article or uploaded as supplemental information.
Ethics statements
Acknowledgments
Thank you to Monica Floquet for her help with database development and data analysis. Thank you to Meghan McClure, MD, for her assistance with education, data collection and future steps for the project.
Publication costs were generously supported by the Texas Children's Hospital Young Investigators Endowed Fund.
References
Footnotes
Contributors MSC conceptualised and designed the project, developed educational materials, carried out analyses, drafted the initial manuscript and reviewed and revised the manuscript. CD, KA and MR contributed to conceptualisation and design of the project, collected data and reviewed and revised the manuscript. BP contributed to conceptualisation and design of the project, provided quality improvement expertise and feedback, developed the data collection tool and reviewed and revised the manuscript. JS contributed to project design, reviewed data and revised the manuscript for important intellectual content. KL-W conceptualised and designed the project, developed educational materials, collected data, carried our analyses and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement statement Given that this was a quality improvement project to improve patient handoffs among physicians, patients and the public were not involved in the design, conduct, reporting or dissemination of our research.
Provenance and peer review Not commissioned; externally peer reviewed.