Article Text

Abstract
Introduction Personal protective equipment is essential to protect health workers and patients and to ensure confidence when dealing with aerosolised disease transmission. We describe the process for ensuring adequate filtering facepiece respirator (FFR) qualitative fit testing at a local level during the COVID-19 pandemic.
Methods Cascaded training is described, which allowed rapid spreading of the testing process, with supervision allowing quality assurance throughout. Testing consisted of subjective ‘fit checking’, checking for leaks, followed by qualitative hood testing.
Results The original respirators (3M 1870) had a hood test pass rate of 87.5%. Following identification of this as a non-renewable and unsustainable option, a domestically manufactured and sustainable Help-It P2 duckbill-type respirator was adopted as the primary FFR. The hood test pass rate for this respirator was only 54%. A third respirator was made available (3M 1860), with a high pass rate of 80% but also a limited and non-renewable resource. Algorithms were constructed highlighting different proportional use of the respirators depending on the most limited resource.
Conclusion The testing format used is simple, reproducible and can be used by any hospital organisation when occupational health and safety departments are unable to provide the service during overwhelming demand. Qualitative fit testing is a scalable and effective method for ensuring appropriately sized and shaped FFRs, minimising resource consumption in the process. The use of a product with appropriate filtration capacity but a lower fit test pass rate (domestic duckbill respirator) as a replaceable resource facilitated adequate respirator availability for staff that would otherwise not have been possible. The provision of an FFR fit registry allows an organisation to make appropriate respirators available to staff from different sources as supply and demand changes.
- COVID-19
- equipment safety
- equipment and supplies
- healthcare quality improvement
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The SARS-COVID-19 pandemic has challenged the appropriate use and availability1 of personal protective equipment (PPE). PPE is the final stage of risk management, deployed as part of the hierarchy of controls for occupational exposure of hazardous substances in the workplace.2 An integral part of this, where appropriate, is the use of fitted filtering facepiece respirator (FFR), designated FFP2, N95 or P2 for protection against airborne and aerosolised disease transmission.3 4 Sourcing appropriate FFRs during times of crisis, such as the current COVID-19 pandemic, can be problematic.
Ensuring healthcare provider safety is of paramount importance during these challenging times as supplies of PPE equipment change, necessitating testing and retesting of safety equipment during the outbreak. Any response should be guided by common sense principles and a logical framework such that the availability of PPE should be constant, predictable, scalable and evidence based where possible. Healthcare worker confidence in safety equipment and the management team is important for healthcare provider safety, as highlighted in a recent Cochrane rapid review.5 Workplace culture, training, access to and trust in the PPE and support from managers are factors that positively impact healthcare workers and increase their willingness to follow infection prevention and control guidelines.5
Providing adequate PPE for staff in an environment of ongoing risk from potential SARS-CoV-2 exposure requires an approach that responds to the changing risk of disease transmission, exposure of potential and actual cases with COVID-19 and logistical issues with national and international supply chains for PPE. Changing demands due to variation in disease prevalence, hospital admissions, internal policies and guidelines test the demand side of this balance while limitations in equipment storage, accessibility and renewal of depleted stores test the supply side.
Evidence from the SARS-CoV epidemic6 suggests significant risk of virus transmission in the operating room (OR) environment. This was attributed to many procedures routinely undertaken by anaesthetists, for example, bag mask ventilation and intubation, as well as other surgical aerosol-generating procedures (AGPs). Providing appropriately fitted FFRs is an important and universal component of appropriate PPE in these situations.
FFRs must be appropriately fitted for them to be effective, such that air cannot be entrained around the respirator and must pass through the filter. This may appear obvious but inadequate fitting and testing leaves the individual potentially exposed to the very hazard that the masks are designed to mitigate. ‘Fit Checking’ describes the process that the individual (subject) uses to ensure a good facial seal, whereas ‘Fit Testing’ describes a process involving a qualitative or quantitative process. Up to 25% of people who feel they have an adequate seal of the respirator on fit checking will go on to fail qualitative testing.7 As such, fit testing is recommended with the current COVID-19 outbreak.8
The initial assessment of the tight-fitting respirator is known as the ‘secure fit check’. This begins with instructor-guided best practice application and subsequent adjustments aiming to achieve the most effective interface between the respirator edges and facial skin. Subjective assessment of the magnitude of air leak around the limits of the respirator is performed and advice/assistance is then offered in an attempt to optimise the positioning and to encourage effective moulding of the nose piece.
Fit testing of an FFR can be either quantitative or qualitative. Quantitative testing assesses particle filtration by comparing the ratio of airborne substances inside and outside the respirator. It requires staff with specific training, relatively expensive equipment and renders the mask unusable due to the required insertion of a sampling tube. Although this may be considered the ‘gold standard’ it is impractical to upgrade such a system to provide comprehensive protection during a pandemic.9 Qualitative testing uses an aerosolised buffered bitter and/or sweet testing agent administered into a defined volume hood. A respirator fit will fail if the subject tastes either the sweet or bitter solution employed. Qualitative testing is relatively easy to deploy at a more local or departmental level, requires less staff training and uses relatively inexpensive and simpler equipment than quantitative testing. It provides reassurance to staff and the respirator used for testing is safe for subsequent use.9
In usual circumstances, responsibility for workplace safety resides predominantly with occupational health and safety departments within an organisation. In accordance with the New Zealand Health and Safety at Work Act 2015, appropriate respiratory protective equipment must be provided to staff likely to be exposed to an occupational airborne hazard. This provision must also include appropriate training in donning the respirator and qualitative or quantitative fit testing. The state of emergency caused by COVID-19 and the ensuing demand for respirator fit testing overwhelmed the usual organisational capacity.
We describe the issues encountered while providing a systematic solution for ensuring adequate provision and fit testing of suitable FFRs in this changing and challenging environment and suggest how this might be used in the future. The objective was to have all those individuals working in the ORs adequately fit tested.
Methods
Changes in the operational status at our hospital, a large tertiary centre, resulted in the temporary cessation of elective procedures and preparation for an expected influx of infected patients requiring intensive ventilator management. At the beginning of this process, it was realised that intensive staff training in PPE would be required as very few staff had ever been exposed to this safety equipment before. Unfortunately, our occupational health department, who would normally oversee such training, were overwhelmed and unable to assist. Available OR staff, anaesthetic trainees, nurses and anaesthesia technicians were taught and trained to provide N95 fit checking and qualitative hood testing to the standard previously determined by our occupational health department using the process outlined below. This is in accordance with the Occupational Safety and Health Administration (Occupational Safety and Health Standards) accepted fit test procedures.10
Interventions
Cascaded training
Training was delivered by a consultant anaesthetist, who received basic instruction on the secure fit test for the 3M 1870 respirator and 3M educational video material, to an original cohort of two registrars, one fellow and one senior theatre nurse based in our OR suite comprising seven theatres. This involved video aids on respirator placement, fit checking and hood testing specific to the 3M 1870 facemask, based on 3M training guides. Critical appraisal of each other in a workshop environment followed.
On return to theatres further trainer training was delivered by the original cohort to 12 additional staff using the same resources: 2 anaesthetic technicians, 4 further anaesthetic registrars, 2 recovery staff and 4 scrub nurses. All staff members interspersed testing with normal clinical work.
Staff testing: organisation
Equipment
Two testing hoods were originally sourced; both official 3M products with bitter (Bitrex=denatonium benzoate) and sweet solution (containing sodium saccharin) nebuliser testing kits. The hood numbers intermittently increased to 3–4, with a limited supply nationally. These hoods were subsequently shared with other areas within the organisation. The supply of the branded 3M testing solutions was exhausted within a short period of time and locally produced alternatives were sourced. A collaborative arrangement with a neighbouring district health board allowed access to the bitter solution base components. Pharmaceutical quality threshold and testing concentration solutions were subsequently available for the duration of the intensive testing phase.
In recognising the limitation imposed on testing capacity by the small number of available hoods the possibility of local production was explored but was unsuccessful.
Hygiene
Testers undertook hand hygiene precautions and donned non-sterile nitrile gloves for each individual episode. All hoods were cleaned between candidates with Clinell universal sanitising wipes (non-sporicidal 2% chlorhexidine and 70% ethanol-based alcohol) applied to all internal and external surfaces. All nebuliser devices had tops washed with hot soapy water between candidates with secondary Clinell surface cleaning immediately before use.
Environment
Empty ORs, vacated as part of COVID-19 response, were used to take advantage of frequent air exchanges, thereby reducing the risk of contamination and pollution. In order to practise social distancing, workspaces were appropriately separated with a minimum distance of 2 m between stations. One tester acted as coordinator to ensure a constant flow of staff; limiting crowding and maximising throughput.
Leadership and support
Support and involvement from senior clinical members of the management team maintained efficiency and morale among testers by facilitating release of testers from clinical responsibilities and limiting testing periods to 4-hour stints with protected breaks. This prevented fatigue and burnout of the involved testing personnel.
Staff testing: process
Respirator availability and type
Initial secure fit checking and hood testing were carried out on 3M 1870 respirators as these were the preferred type and no alternative was physically available at that time. Within a week after completing the testing, it became apparent that the supply chain would be inadequate if the anticipated increased requirement for these eventuated. This was due to difficulties in replenishing stock originally sourced through China.
A New Zealand-manufactured Help-It P2 duckbill-type respirator was soon accessed as a readily available locally manufactured alternative, limiting the impact of isolation from reduced import of masks and materials. While meeting the performance characteristics dictated by the Australian/New Zealand Standard 1716:2012 for P2 facemasks (table 1) there were minimal data regarding appropriateness of fit. The Australian and New Zealand standard is similar to US National Institute for Occupational Safety and Health N95 and European FFP2 respirators, in that it specifies physical properties and performance characteristics. Comparison of the three standards is summarised in table 1.11
Comparison of different international FFR standards
A supply of 3M 1860/1860S N95 respirators was also maintained but as with the 3M 1870 variant they were unlikely to be a renewable resource in the projected time period (see figure 1). Due to availability of 3M 1860 and 1860S masks, these were not differentiated in testing and are referred to simply as 1860. Those with smaller faces were fitted with the 1860S but specific details were not recorded in our database.

Filtering facepiece respirators used—clockwise from left to right: 3M Aura 1870+ (N95), 3M 1860 (N95), Help-It (P2). N95 (US NIOSH 42CFR84). P2 (Australia/New Zealand AS/NZS 1716:2012). AS/NZS, Standards Australia and Standards New Zealand; NIOSH, National Institute for Occupational Safety and Health.
In accepting that the Help-It P2 respirator had the potential to rapidly become the only type of respiratory protective equipment available, an aggressive retesting strategy for all staff was initiated.
Evolving methodology
Initially, staff likely to be involved in AGPs were prioritised and fit tested. Testing with the original 3M 1870 respirator was managed without the need for a formal appointment system. The high rate of success for individuals with the secure fit checking and hood tests limited retesting with other respirators and ensured a predictable and rapid process. A small number of failures underwent subsequent fitting with 3M 1860 respirator (see the Results section). Higher failure rates with the Help-It P2 respirator and need for further 3M 1860 mask testing engendered a much slower undertaking which rendered a ‘drop in’ approach untenable. An appointment system was subsequently employed allocating half-hour slots to maintain social distancing and avoid overcrowding. There was less ‘spontaneous’ uptake of appointments due to ‘hood fatigue’ (all theatre staff by this point had already been tested for the 3M 1870 respirator within 1–2 weeks of the repeat testing) and less perceived urgency due to decreasing reported COVID-19 cases in hospital and the community.
Quality assurance
Individuals from the original ‘test group’ supervised further testers and provided troubleshooting support. There was also a workshop with previously trained senior OR staff and practice educators to discuss and troubleshoot the testing and hygiene processes. Moving from the 3M 1870 to the Help-It P2 and 3M 1860, testing used the same material for the initial hood testing. This material was a 3M SecureFit test, which was adapted to ensure the fit of all three masks. Minimal resources or information were available to optimise the application and fit of the Help-It P2 respirator, so the training team used the experience gained with the initial round of fit testing to guide their approach.
Measures
Disclosure and documentation
All staff were informed of the non-compulsory nature of testing. Testing was recommended to provide confidence in equipment and ensure adequate protection for all staff. Tests were recorded using a standard organisational occupational health form, which included consent and medical history. All data were kept in line with Caldicott principles.12 A database was constructed with restricted access but live update capability. From this, another database was provided to the senior theatre management team detailing respirator fits for individual staff to allow appropriate mask and staff allocations in the event of a COVID-19 case.
Analysis
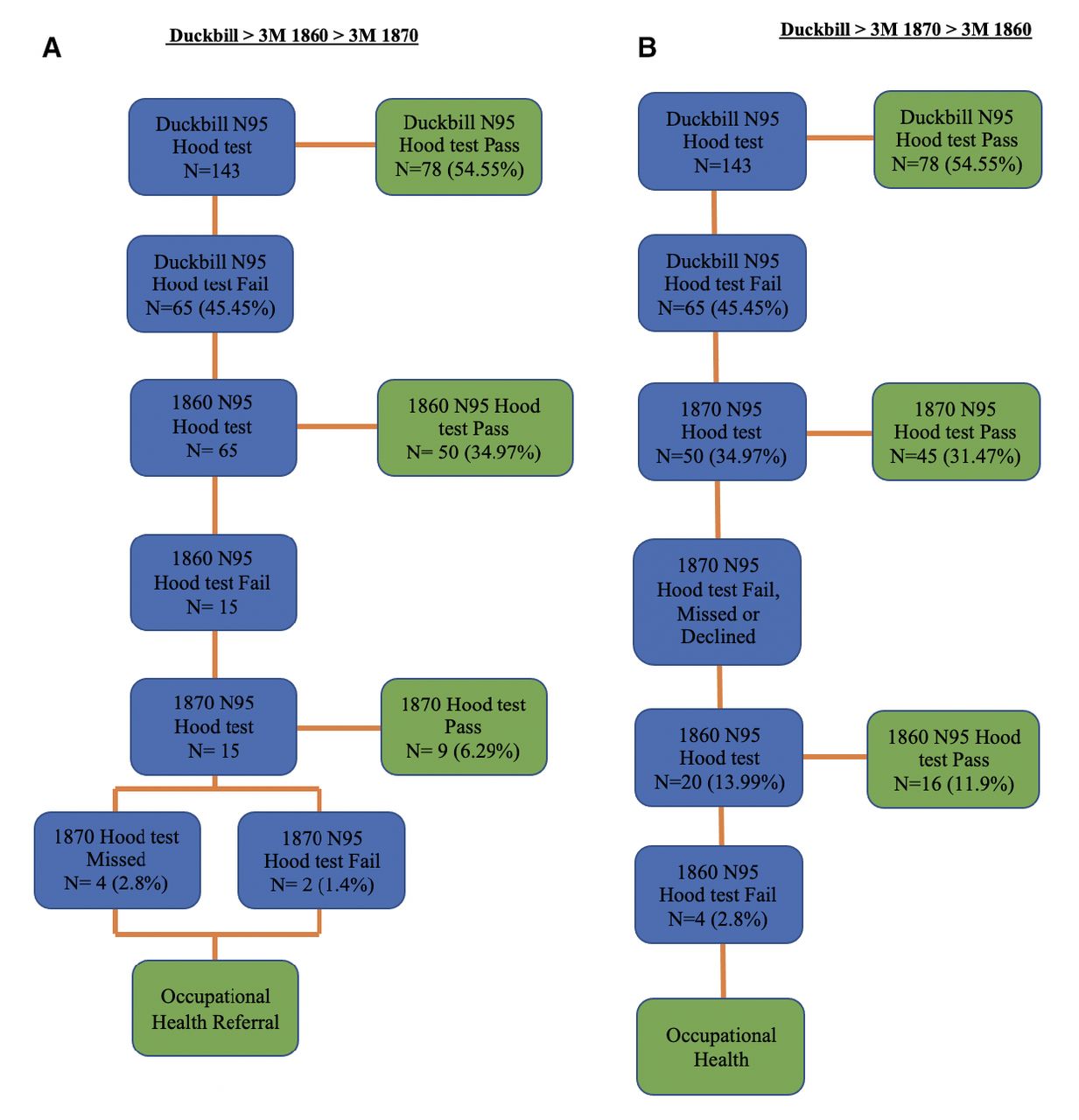
A table of success and failure rates of different respirator types was constructed from the raw data broken down by sex, for subsequent analysis. 2×2 contingency tables were constructed to allow analysis of potential sex-related respirator fit failures. Fisher’s exact test was applied for each mask type and the relative risk (RR) of failure for male versus female was calculated. Decision trees regarding the most appropriate respirator fitting regimens were constructed for two scenarios: (A) where the 3M 1870 respirator was the most constrained resource, and (B) should the 3M 1860 respirator become the most constrained resource.
Results
One hundred and ninety-four staff were initially subjectively fit tested with a 3M 1870 respirator offered as the ‘preferred’ respiratory protection by our organisation of whom five failed resulting in a failure rate of 2.6%
Table 2 illustrates the number of staff tested with the three respirators, their overall failure rates and failure rates by sex. One hundred and fifty-one (55 male, 96 female) staff proceeded to qualitative hood testing, initially using the 3M 1870 respirator. Nineteen staff (3 male, 16 female) failed the fit test for a failure rate of 12.5%. A total of 10 staff declined the test and 33 staff were designated to other duties without risk of clinical COVID-19 contact.
Fit and hood testing 3M 1870, Help-It and 3M 1860
When the testing was recommenced for the Help-It P2 respirator, 143 staff completed the testing and 11 declined (not involved with patients with COVID-19). With this respirator, 65 staff (30 male, 35 female) failed the fit test and 78 passed (18 male, 60 female) resulting in a failure rate of 45.5%. Subjective assessment of the reason for failure showed that in 32 (50%) (11 male, 21 female), there was an obvious leak around the nose, and for the other 33 (50%) (19 male, 14 female) there were a variety of causes: head/neck movement 8, leak under chin 4, deep breathing 3, unable to keep mask on face 3, unknown 15.
Of the 65 staff who failed the Help-It P2 respirator, 50 passed the hood test with the 3M 1860 respirator and 46 had previously passed the hood test with the 3M 1870 respirator. In total, 78 staff were hood tested with the 3M 1860 respirator with 15 failures, resulting in a failure rate of 19.2%. There was no specific feature identifiable leading to these failures.
Only two staff failed the hood test with all three respirators and for both individuals, the occupational health department was able to source an appropriately fitting mask. One member of staff was unable to taste either sweet or bitter and was able to get quantitative testing, fitting the Help-It P2 respirator. These individuals are not counted in our ‘hood testing’ data as they did not ‘fail’ the hood testing, they were screened out in the baseline testing.
The failure rates by respirator type and sex are summarised in table 3. For the 3M 1870 respirator failure rate, no gender bias was identified, despite an RR=0.33. The high failure rate of the Help-It P2 respirator demonstrated an increased failure rate in males (63%) compared with females (37%) with RR=1.7 (p=0.005). For the 3M 1860 respirator no gender bias was identified.
Respirator-type failure by sex: contingency table and analysis
From the hood testing data, a decision tree regarding respirator allocation was constructed with the Help-It P2 respirator as the first choice whenever possible, the 3M 1860 as the second choice and the 3M 1870 as the third choice based on availability information at the time of completion of this exercise (decision tree—figure 2A). This demonstrated that 55% of staff should use the Help-It P2 respirator, 35% 3M 1860 respirator and only 6% would need to use the 3M 1870 respirator. Of the remainder, 5 (3%) were retasked to non-clinical duties and did not complete the testing and 2 (1%) fitted none of the masks so were referred to occupational health for further assessment and fitting. This also applied for the remaining 4 (2.8%) in decision tree B. Should the 3M 1860 respirator availability become more restricted than the 3M 1870 mask then an alternative decision tree could be used (decision tree—figure 2B), indicating 12% employees would require this respirator.
{kind=link}
{kind=link}
Decision tree depending on respirator availability. (Path A or B as detailed in the text).
Of note, there were no outbreaks of cough/cold COVID-19 positive or otherwise in the testers or candidates during this time, supporting adequate hygiene policies.
Discussion
The cascaded training and deployment of a limited number of OR staff to provide qualitative fit testing for high filtration respirators during the current COVID-19 pandemic resulted in all team members being appropriately fitted at a time when the organisation’s occupational health department was unable to provide the service. The process proved to be rapidly adaptable in the face of disrupted supply lines, changing suppliers and varying requirements. It coped with testing and retesting staff up to three times from a seven-theatre operating suite plus radiology locations in order to provide properly fit tested respirators.
The testing process described highlights a number of issues with ensuring staff safety through adequate and appropriate testing. First, with the initial testing of a widely used commercial product (3M 1870 respirators), fit checking suggested a 2.6% failure rate but qualitative testing demonstrated a failure rate of 12.6%, an almost fivefold increase. Second, the subsequent respirator (Help-It P2) that we were required to test (due to concerns about the adequate supply of the initial mask) was clearly inferior to the previously tested mask: 45% vs 12.6% failure rate. Because it was a renewable resource (locally produced) and not subject to the same supply constraints of the 3M respirator, it needed to be part of the solution in providing FFR respiratory protection for our staff. Half of the failures were due to fitting difficulties around the bridge of the nose suggesting the design could be improved, which was fed back to the manufacturer. This was the only respirator not to have foam under the metal nose strip. Third, shifting information regarding potential availability of alternate masks resulted in testing of another 3M N95 respirator (1860) to ensure that something was available for all staff.
Each mask has a different shape and design, so it is not surprising that different respirators fit different face types. All the masks have a nose strip that needs to be moulded to the nose. Both 3M masks have nose foam, but the Help-It P2 respirator does not. The 3M 1870 respirator has a three-panel design, the 3M 1860 is a more rigid dome-shaped design and the Help-It respirator is a duckbill shape (figure 1). The duckbill respirator appeared more suitable to female face shapes, with a lower failure rate, RR=1.7: only 38% of male faces fitted this mask. Data regarding race or facial shapes were not collected.
Differing failure rates between the sexes for the 3M 1870 and Help-It P2 respirators reflect the difficulty in matching different respirators with differing facial size and morphology. This highlights the need for qualitative or quantitative testing and the unreliability of subjective secure fit checking alone. This is in keeping with previous work. Gender and age may both impact the likelihood of successful fitting. Younger females are more likely to fail qualitative fit testing with 3M 1870 N95 masks.13 People with larger facial dimensions have a greater chance of an adequate respirator fit test with some respirators. Overall, the facial fit of filtering facepieces increases with increasing facial dimensions. Respirators with a three-panel flat fold structured in the facepiece provide a greater fit, particularly when users move their heads with gender-specific difference consistently observed with different anthropometric measurements.14 Qualitative testing failure rates reported for the 3M 1870 respirators have been as high as 64%, and as high as 54% and 84% for the 3M 1860 and 3M 1860S, respectively.15 Duckbill respirators are associated with a higher failure rate than dome-shaped masks.16 Collectively, these articles highlight the heterogeneity of different populations and the need for a variety of respirators to be available for staff.
At the end of this process, the most limited resource was the 3M 1870 respirator. Based on this information, the initial decision tree (figure 2A) was constructed. Using this approach, the 3M 1870 respirator use could potentially be reduced to 6.3% of the total demand, with the renewable Help-It P2 respirator accounting for 55% and the 3M 1860 respirators for 35% of the total requirement. This allowed for appropriate distribution and allocation of FFRs and should facilitate improved inventory control and distribution. Should the most limited respirator resource change to the 3M 1860 variant, the decision tree can be adapted as in figure 2B, which shows that the limited resource would be required for 12% of staff with the duckbill providing 55% and the 3M 1870 respirator 31% of total requirements.
Previous studies have shown that the elimination of qualitative or quantitative fit testing and relying on a user seal check alone increases the exposure risk for staff, even when experienced users are involved.4 In the current pandemic, almost all users are inexperienced and most are naïve in regard to mask fitting which emphasises the importance of an adequate safety checking regimen with appropriate and visible quality assurance in keeping with crisis resource management and teamwork training principles.5 17 From the H1N1 influenza pandemic in Australia in 2009, ensuring adequate PPE and infection control, maintaining staff morale, addressing new required roles for staff and managing the fear of contracting and transmitting the disease were the most important themes that impacted the lived experience of staff during the pandemic.18 There is also evidence that poor PPE practice and inadequately fitting facemasks contributed to healthcare worker infection during the SARS epidemic.19
Limitations
Due to the low number of COVID-19 cases nationally we were unable to determine the clinical impact of our intervention on healthcare staff. However, the performed tests are validated and provided security for staff and patients.
Conclusion
Subjective fit checking and qualitative fit testing of FFRs using local staff rather than the usual staff from occupational health is readily achievable when a simple process of cascaded training as described is followed. We have shown that in a time of crisis, as occurred during the current COVID-19 pandemic, staff can be rapidly trained and deployed to provide a robust and effective method of ensuring appropriate selection and fitting of FFRs necessary to maintain staff safety. The visibility of the process being delivered by colleagues provided additional reassurance that their safety was of high organisational concern.
The process described in this article could be replicated in any part of a healthcare organisation by releasing a limited number of staff from their usual duties for a limited period of time during a time of crisis.
Data availability statement
Data are available upon request.
Ethics statements
Acknowledgments
The authors would like to thank the Starship Theatre team for their efforts and support in the mask fitting.
Footnotes
Contributors CA, JS, OB: data collection. PX: data collection and analysis. NW: data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.