Article Text

Abstract
Supporting social emotional development, beginning at birth, can improve lifelong health. The American Academy of Paediatrics recommends 12 well-child visits between birth and age 3 years. Each well-child visit provides a unique opportunity to interact with and support families to promote social emotional development of children. Eighteen US paediatric practices joined a learning community to use improvement science to test and implement evidence-informed strategies that nurture parent–child relationships and promote the social emotional development of young children.
Quality improvement methods were used to integrate 11 strategies into well-child visits between birth and age 3 years and measure the improvements with a set of outcome, process and balancing measures. Participation among the 18 paediatric practices was high with 72% of teams attending monthly webinars and 97% of teams attending the three learning sessions. Over 12 months, the percentage of children receiving age-appropriate social emotional development screens at participating practices’ well-child visits increased from a baseline median of 83% to 93%.
Current paediatric practice in the USA focuses primarily on cognitive and physical development, and paediatric providers are less familiar with established practices to screen for social emotional development and promote the caregiver–child relationship. This project suggests that improvement methods show promise in increasing the number of children who receive age-appropriate social emotional development screens or assessments at well-child visits.
- paediatrics
- healthcare quality improvement
- control charts/run charts
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Emerging evidence around the Life Course Health Development Framework emphasises that supporting children’s social emotional (SE) development may promote positive mental and physical health outcomes later in life.1 2 Optimal SE development is defined as a child’s ability to have and maintain positive relationships and manage their emotions in a healthy and appropriate manner.3 SE development is demonstrated by the ability to understand both one’s own emotions and the emotional states of others, constructively manage strong emotions, regulate one’s own behaviour, display empathy and maintain relationships.4–6 Positive caregiver–child relationships support children feeling safe and secure, especially when they receive consistent, reliable responses from primary adult caregivers.7 These early childhood relationships assist with the full development of neural synapses, brain architecture, empathy, resilience and other cognitive capabilities.8
The paediatric well-child visit presents a unique opportunity to promote SE development and provide parents with important resources and support. The 12 recommended well-child visits between birth and age 3 years provide a unique and frequent opportunity to interact with and support families.8 However, paediatric practices primarily focus on cognitive development and the prevention and treatment of physical illness. While there are a variety of promising programmes already functioning that support SE development in paediatric primary care, such as HealthySteps9 and Reach Out and Read,10 these are not universal. Additionally, paediatricians and their staff lack familiarity and confidence with many established SE screens and thus miss opportunities to promote both SE development and the primary caregiver–child relationship. In addition, limitations in the current well-child visit such as visit length, number and length of other screening, and family education all challenge the adoption of universal promotion of SE health.11
In 2017, a group of early childhood private funders collaborated to launch the Pediatrics Supporting Parents initiative to optimise the SE development of children from birth to age 3 years by redesigning processes that improve support to parents during well-child visits. A year-long learning community of 18 paediatric practices from across the USA was launched in March 2019. The aim from March 2019 to March 2020 was to support 18 practices in creating more reliable systems for screening and providing SE development support to children and parents during well-child visits. The ultimate goal was for parents to leave the well-child visits in a better position to provide SE support to their children. Teams were provided a change package of evidence-informed strategies (see table 1—Core practices) and used improvement science to test and learn how to best incorporate them into their workflow. The 11 core practices used were identified and informed by a programme analysis conducted from 2017 to 2019 by the Center for the Study of Social Policy.
Core practices
Paediatric practices were recruited through an online marketing campaign that used the networks of the National Institute for Children’s Health Quality (NICHQ) and early childhood community partners across the USA. Twenty-two practices completed applications and 18 were selected representing 12 states and a total patient population of 78 000 children/year (see table 2). Selection criteria included demonstrated alignment with the learning community’s guiding principles, existing community partnerships to enhance care coordination for families, existing infrastructure for collecting and analysing improvement data, and previous experience with a major improvement or transformative change activity. NICHQ sought diversity of geography, patient demographics and paediatric practice size to inform learning.
Characteristics of participating paediatric practices
Background
Promoting optimal SE development requires a comprehensive, system-wide approach, including ways to support children and their parents across settings. While a variety of programmes offer support in multiple venues, relatively few programmes take place in primary care settings, and SE screening within primary care for infants and toddlers is not common practice.12 13 The dearth of programmes in the primary care setting likely is due, in part, to inherent challenges in the structure of primary care. This may include increasing demands for non-clinical responsibilities such as billing, documentation and evaluation. Clinicians already have numerous competing demands for a brief visit, including physical growth and development, household safety and vaccinations. Some primary care providers also report lack of confidence and/or training to conduct such screening.14 It could be argued that providers have little time to take on additional topics such as SE health of the child and the quality of the parent–child relationship. However, providers who have participated in such interventions have reported that time constraints did not weigh heavily in terms of programme limitations.15 There is a clear opportunity for interventions, sensitive to the barriers and competing demands in the primary care space, to promote SE development in paediatric well-child care. A holistic, comprehensive approach that considers the child and family in the context of all aspects of life is necessary to optimise health and well-being.16 17 Although much attention has focused on early childhood development, the primary care setting has not been fully leveraged and is an important opportunity to further reach children and their families.
Measurement
The measurement strategy included quantitative measures and qualitative assessments to foster understanding of whether and how 11 evidence-informed strategies (core practices; see table 1) related to the parent–child relationship and affected practice change within the well-child visit for children from birth to 3 years.
Quantitative measures
Outcome measures
Parent knowledge of SE development and self-efficacy
Data source: 10 preselected items from the validated Knowledge of Infant Development Inventory (KIDI) parent questionnaire.
Strategy: monthly, collect 30 KIDI questionnaires from parents with children 0–36 months each month who have a well-child visit.
Parent–child relationship
Data source: percentage reporting top 2 boxes of 1–7 scale for each of the three questions: (a) How confident do you feel leaving this visit that you are able to support your child’s SE development?; (b) How confident do you feel leaving this visit that you know how to strengthen your relationship and your family’s relationship with your child?; (c) How confident are you that you could find resources in the community to help you strengthen your relationship with your child if you needed them?
Strategy: monthly, collect 30 responses from parents of children 0–36 months of age.
Process measures sought to understand changes at the practice level. Data were collected from patient charts on 100% of children seen at a well-child visit during the measurement month (or a sample of 20 if information not easily accessible).
Percentage of well-child visits where child leaves with at least one goal related to SE development co-created between parent and provider.
Percentage of children receiving age-appropriate SE developmental screens or assessments at well-child visits.
Percentage of those with positive screens or assessments referred.
Percentage of well-child visits where a strength-based bundle was used and included: observation, reflection, engagement and positive instructive feedback.
Percentage of child visits with screening/assessment completed for family stressors (eg, parental depression, social determinants of health).
Percentage of those screening positive for family stressors who are offered support or services aligned with their self-identified needs and priorities.
Percentage of referrals where loop is closed (per the parent, it has resolution and no longer a topic they need help with).
A quarterly ‘Joy in Work’ balancing measure was collected and reported to assess whether the new work related to SE development during well-child visits affected staff satisfaction. Quarterly anonymous surveys asked staff if they would strongly agree, agree, disagree or strongly disagree with the statement, ‘I would recommend this practice as a great place to work’.
For 12 months, between April 2019 and April 2020, teams voluntarily reported monthly de-identified quantitative data. NICHQ initially proposed weekly data collection to have more data points such that improvement patterns would emerge sooner in the project, however, none of the participating practices could support a weekly data reporting requirement. Based on this feedback and to further reduce the burden of new measurement and reporting, the measures were introduced in stages between April and July 2019 and reported through May 2020.
Qualitative assessments
Paediatric practices participated in qualitative assessments to inform learning and improvement during the 12-month learning community.
Self-assessment of progress on core practice strategies (two surveys)
Practice teams were asked to respond to two surveys, one administered during project midpoint and one at project end, to assess teams’ progress on the testing and implementation of the core practice strategies. Core practices were defined as high leverage changes that could promote SE health, the parent–child bond and parental mental health within the paediatric well-child visit (see table 1). Participants were asked to rate their perceived progress on the 11 core practices using a 6-point scale (0=no work on practice, 1=plans but no action on practice, 2=testing one idea related to practice, 3=testing multiple ideas related to practice, 4=testing multiple ideas related to practice with plans to implement, and 5=implemented ideas related to practice and working on sustaining improvement). Descriptive statistics, including frequencies and means, were examined among participants’ responses at both time points. In addition, t-tests were conducted to determine whether participants’ perceived progress on each of the core practices differed significantly over the course of the project.
Experiences of participating paediatric practices (interviews)
Interviews were conducted with 10 of the paediatric practices that responded to an open invitation at the midpoint of the learning community. Notes from the semistructured interviews were reviewed using thematic analysis with NVivo V.12.0. Interviews were initially reviewed in their entirety and then iteratively coded until primary, secondary and tertiary themes were identified. Results of the thematic analysis provided important insights into the barriers and facilitators of incorporating the core practices into the paediatric well-child visit.
Design
Our theory of change was portrayed in a Driver Diagram18 and companion change package that reflected 11 evidence-informed strategies, named core practices. The core practices are high leverage changes that could promote SE health, the parent–child bond and parental mental health within the paediatric well-child visit (see table 1). Throughout the learning community, paediatric practices tested multiple change ideas and implemented core practices 1, 2, 3, 6, 8, 9, 10, 11. Paediatric practices made plans for but did not move to testing for core practices 4, 5, 7.
Paediatric practices tested and implemented changes within well-child visits for children aged 0–3 years. The learning community provided peer support, learning and reflection grounded in transparent sharing between participants of tests of change, data and results. Expert faculty coached teams on core content related to SE development, the Model for Improvement, and how to adapt changes to local well-child visit settings. Paediatric practice teams represented by a team leader, medical provider champion, family partner(s) and data lead attended one in-person and two virtual learning sessions combined with monthly coaching and technical assistance webinars over the 12-month initiative. Monthly webinars balanced presentations by faculty with expertise in SE development, family engagement and quality improvement with sharing by the participating practice teams. Topics included process mapping for improved workflow, family engagement strategies, co-created goal setting, and conducting strength-based observation and feedback. There was high team engagement: 72% attended monthly webinars and 97% attended the three learning sessions.
Qualitative assessments were used to inform and customise the curriculum for the second half of the learning community. They provided additional context on the experiences of testing and implementing the core practices and of collecting, reporting and analysing data. For instance, following interviews with 10 paediatric practices, additional reports from participating teams were included in the monthly calls as this was noted as one of the greatest benefits of participating in the learning community.
Participants reported monthly progress on NICHQ’s Collaboratory, an online platform, for discussion, resource sharing, data submission and data visualisation. Faculty experts and learning community leadership reviewed and provided coaching on Plan–Do–Study–Act (PDSA) submissions and quantitative data. Each paediatric practice team received $10 000 to support learning activities.
Strategy
Paediatric practices attended an in-person learning session in January 2019 and received coaching on quality improvement methods and content related to the core practices. Objectives for paediatric practices following this first learning session included the following:
Understand the aim and goals of the Pediatrics Supporting Parents learning community.
Explain their practice’s aim and goals as they relate to the learning community’s aim and goals.
Learn how to identify gaps in the SE development of children in their community and key strategies to help close those gaps.
Gain a better understanding of what can be done to support parents and children with their SE development within the scope of the well-child visit.
Understand the Model for Improvement and its value in executing improvement work.
Understand the value of PDSA cycles to learn and improve.
Plan for at least two tests of change, using PDSA cycles, to take place in their practice the week following learning session 1.
Paediatric practices self-selected which core practice(s) they would work on. Fourteen paediatric practices (80% of the teams) reported a test of change (ie, a PDSA cycle) within the first week of learning session 1, an important early marker for engagement. As a learning community of 18 paediatric practices, multiple PDSA cycles were conducted to effectively test how to incorporate the 11 core practices into the well-child visit setting. For illustrative purposes, an iterative cycle for core practice 1: designate roles among the care team and standardise workflow to provide developmental, behavioural, and social determinants of health screening, developmental health promotion, support, and resources, is included.
Cycle 1 hypothesis: SE screening rates will increase by incorporating the ASQ:SE-2 at the 9-month visit rather than the 30-month visit.
Plan: five patients will be screened with the ASQ:SE-2 at the 9-month well-child visit; staff will ask parents if they find it challenging to complete the ASQ3 and ASQ:SE-2 at the 9-month visit.
Do: five patients were screened with the ASQ:SE-2 in addition to the standard ASQ-3 during the month of August 2019.
Study: screening rates for the ASQ:SE-2 increased and parents reported it was not a burden to complete two questionnaires. Staff found it challenging to score two questionnaires prior to the provider seeing the patient and to find enough time to discuss the results in the visit.
Act: adapt and test using the ASQ:SE-2 at the 15-month well-child visit when there are no other questionnaires.
Cycle 2 hypothesis: parents and staff will find it easier to incorporate the ASQ:SE-2 screening at the 15-month visit rather than the 9-month visit.
Plan: five patients will be screened with the ASQ:SE-2 at the 15-month well-child visit; staff and parents will be asked if they found it challenging to complete the questionnaire at this visit.
Do: the cycle was conducted as planned.
Study: screening was conducted with five patients; parents reported that it was not difficult to complete the questionnaire and staff reported that they had adequate time to score it because there were not any other questionnaires. The provider also reported that there was adequate time to review the questionnaire with the parent and work on co-created goals. This test revealed that additional training was necessary for front registration staff. We observed that staff gave the incorrect ASQ to patients and had to rearrange questionnaire boxes and label them differently to make it easier for staff to identify the appropriate ASQ:SE-2 to give each patient based on their age.
Act: adopt and continue conducting the ASQ:SE-2 at the 15-month visit.
By March 2020, 7 of the 18 teams implemented at least 1 of the 11 core practices, and their data signalled early improvement in one or more process measures.
Results
Quantitative measures
Teams used run charts to understand if implementation of the core practices signalled improvement.19 Three run chart rules were used to analyse data for non-random signals of improvement: 6 consecutive points above or below the baseline median (shift), astronomical point, and a trend of 5 or more data points steadily ascending or descending.20
The two outcome measures, which were parent reported, were obtained in 8 of 18 practices. The analytical run chart rules did not show any signals of improvement in the outcome measures: parent knowledge of SE development (O1) and self-efficacy and parent/child relationship (O2). Process measures as reported by the practices reflected initial excellent performance levels. The measures: parent knowledge of social and emotional development and self-efficacy; parent–child relationship; parent-developed goals; the use of a strength-based bundle and screening for family stressors confirmed that these practices were high performing at the onset of the learning community, with sustained performance over the 12 months. This is likely related to the selection criteria of the practice teams which included prior improvement experience and commitment to early childhood development. Closing the loop on referrals was the hardest process measure for practices to collect and report; and there was variability in how practices defined the act of closing the loop.
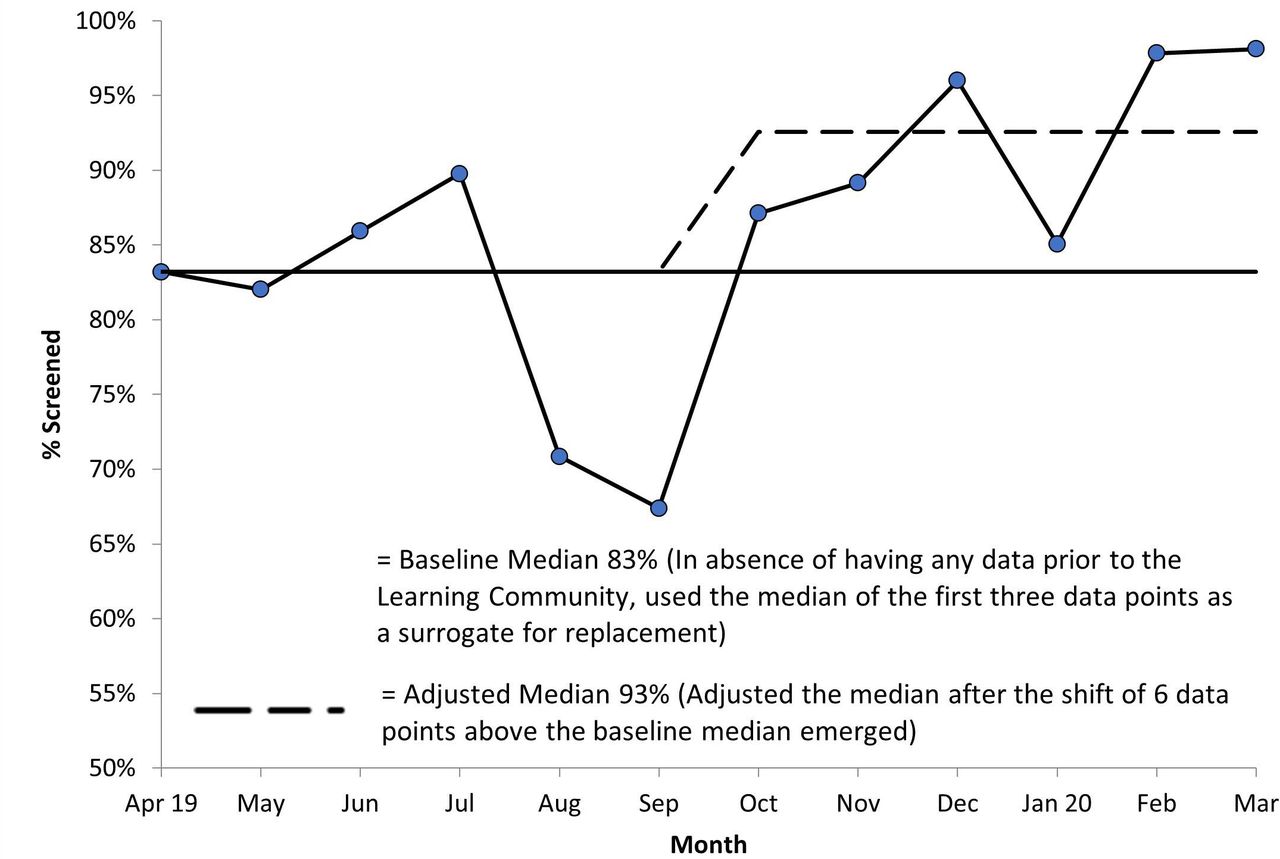
The per cent of children receiving age-appropriate SE developmental screens or assessments at well-child visits showed improvement during the learning community. Fifteen of the 18 teams reported this measure. The first 3 data points in the run chart were used as a surrogate baseline. It was extended into the future to help visualise a shift in performance. A shift in the data occurred in the last 6 months of the learning community.21 The baseline median was 83% and the adjusted median after the favourable shift occurred was 93% (see figure 1).

Percentage of children receiving age-appropriate social and emotional development screens at well-child visit run chart.
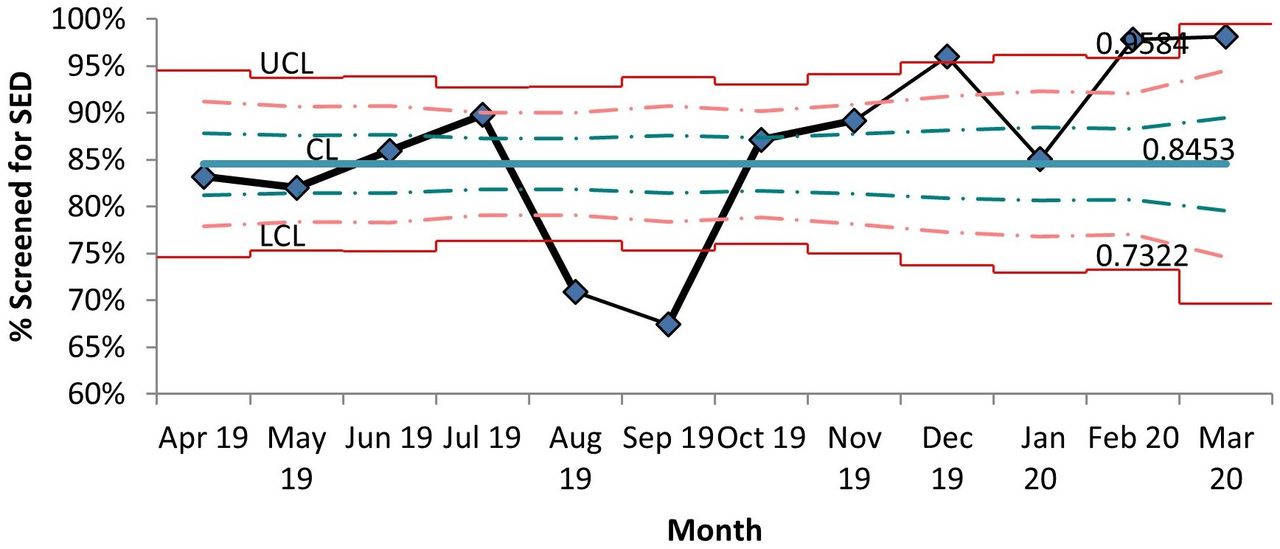
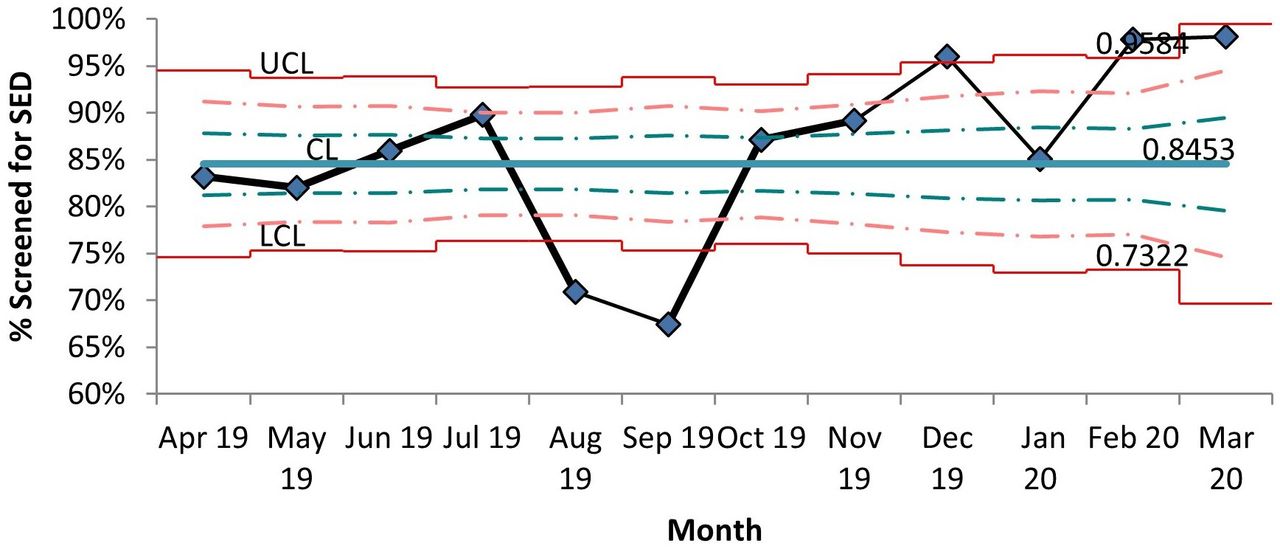
To further understand the run chart signal, we used a Shewhart p chart to detect special cause variation (ie, variation that was caused by a change in the system and not by chance). A p chart with trial limits was selected due to having less than 20 data subgroups. It did detect favourable special cause variation in 3 of the 4 final months of the learning community (see figure 2). We hypothesise that, with a second year of additional data collection, improvement would be detected because this was an area where the teams focused their improvement in the learning community.
{kind=link}
{kind=link}
Percentage of children receiving age-appropriate social and emotional development (SED) screens at well-child visits p chart with trial limits. UCL, Upper Control Limit; CL, Center Line; LCL, Lower Control Limit
Additionally, the project included a balancing measure—staff satisfaction/joy in work to ensure that, while working on improving the core practices, staff did not experience increased burden or decreased joy in their work. Eighty-eight per cent of staff reported they strongly agreed that they would recommend the practice as a great place to work with a median of 91% and mode of 100%.
Qualitative assessments
Self-assessment of progress on core practices
Thirteen practices responded to the progress on core practices survey. Significant differences in the self-assessment of implementation of core practices were found for the following: core practice 6, co-created goal setting, t(11)=2.54, p=0.03; core practice 8, use environments and structures to promote relationships and patient experiences, t(11)=2.69, p=0.02; core practice 11, create support for clinic teams to address burnout, stress/fatigue and retention issues, t(11)=2.25, p=0.05. In addition, a non-significant trend was found for core practice 9, develop community partnerships with clear processes and protocols, t(11)=1.84, p=0.09. While the outcome and process measures did not demonstrate improvement during the learning community with the exception of screening, differences in the two progress on core practices surveys suggest perceived progress in implementation of core practice strategies.
Experiences of participating paediatric practices
Qualitative analysis of project midpoint interviews with 10 practices revealed barriers and facilitators to the implementation of the core practices. Of the 11 core practices, paediatric practices made plans for but did not move to testing for core practices 4, 5, 7. In summary, primary barriers to this work included time and staffing (discussed in all 10 interviews). Specific barriers included family capacity, limited staff capacity (ie, time) to test core practices and limited practice capacity (eg, funding, infrastructure) related to addressing SE development during a well-child visit. Facilitators of the work included pre-existing infrastructure related to this work (eg, HealthySteps, Reach Out and Read), practice motivation, learning community participation, prior quality improvement experience and staffing appropriate to the work.
Lessons and limitations
Paediatric practice teams developed effective changes to improve SE screening and assessment processes for children aged 0–3 years and conducted these within the current structure and constraints of well-child visits. Teams tested and implemented changes based on their organisation’s specific needs and cultures and learnt to provide parental guidance, support parents around SE developmental activities and help parents set age-appropriate goals for their children. The interest in the work was evident as measured by the high number of practice teams that joined the learning sessions and monthly coaching and technical assistance webinars. Teams shared ideas and resources freely and one practice used their stipend to develop a training video that would benefit all.
One notable limitation of the study was also one of its hallmarks. The learning community’s participant practices were high performing in the process measures as reflected in baseline data. The gap between current practice and best practice was small and it sometimes proved difficult to motivate teams to test new ideas and collect and report data when they already performed so well in many of the strategies. However, teams still identified performance gaps and worked to improve and hold their gains in the core practices. The paediatric practices also cited challenges collecting and reporting data throughout the learning community, especially with the onset of COVID-19 in the learning community’s final months. Some practices lacked human resources or time during the well-child visit to be able to collect the ‘parent knowledge of SE development and self-efficacy’ and ‘parent–child relationship’ outcome measures. The short length of the learning community (12 months) created challenges in detecting significant improvement.
Conclusion
Pediatrics Supporting Parents aimed to implement evidence-informed strategies (ie, core practices) that support nurturing parent–child relationships and promote children’s SE development in a learning community setting that employed improvement science and peer support. Results of quantitative measures and qualitative assessments demonstrated that paediatric practices engaged in the learning community process found that the structure facilitated their ability to screen for and implement processes that support the parent–child relationship and promote SE development. Pre-existing infrastructures for screening, training and community support were practice facilitators to promote SE development within the well-child visit. Paediatric practices with pre-existing programmes that support SE development already embedded in their practice, such as HealthySteps and Reach Out and Read, had an easier time incorporating the core practice strategies. These programmes, however, are not universally available to paediatric practices and require significant funding. For paediatric practices that did not have these programmes, this structured learning community was a positive contributor to advancing screening and support for SE development. While our quantitative data were limited to 12 months, an improvement in SE screening was observed among reporting practices, suggesting SE screening is ready for wider diffusion. Practices did note burden on families to complete the screening and on staff to score a lot of screening during the time allotted for a well-child visit. Paediatric practices found data collection and reporting difficult for closing the loop on referrals. They shared improvement barriers of limited visit time, staff buy-in and capacity, and funding to sustain a redesigned workflow.
Addressing and promoting children’s SE development are critical to incorporate into well-child visits in the first few years of life, particularly in light of the potential long-term impact of the COVID-19 pandemic. We have shown that a quality improvement approach increased the number of children who received age-appropriate SE developmental screens or assessments at well-child visits. We recommend future SE development approaches and initiatives build on this work and engage in spread by using quality improvement approaches. Paediatric practices should leverage pre-existing infrastructure including practice motivation, staffing and prior experience with quality improvement initiatives to expand this vital work.
Data availability statement
Data are available upon request.
Ethics statements
Ethics approval
Ethical approval was not required for this project as it was a quality improvement project and not intended as research.
Acknowledgments
We acknowledge the contributions of expert advisors and faculty including: Beth Dworetzky, Dennis Kuo, Dayna Long, Dipesh Navsaria, Ryan Padrez and Jane Taylor. We acknowledge partner organisations in this initiative: the Center for the Study of Social Policy, Child Trends and Family Voices. We recognise the NICHQ current and former staff who contributed to the launch of the learning community including: Colleen Murphy, Kelley Devlin and Emily O’Donnell. Finally, we thank the Silicon Valley Community Foundation and the Pediatrics Supporting Parents funders (The Einhorn Collaborative; J B and M K Pritzker Family Foundation; The David and Lucile Packard Foundation; W K Kellogg Foundation; Overdeck Family Foundation; and an anonymous individual contributor) for their vision and commitment to improving the social emotional health of young children.
Footnotes
Contributors MLJ designed and oversaw the learning community, drafted the initial manuscript, revised the manuscript and approved the manuscript as submitted. SB-D led all improvement activities for the learning community, oversaw the acquisition and interpretation of improvement data, contributed to the initial draft of the manuscript, critically reviewed and revised the manuscript and approved the final manuscript as submitted. MM led the evaluation of the learning community, contributed to the initial draft of the manuscript, critically reviewed the manuscript and approved the final manuscript as submitted. KE contributed to the initial draft of the manuscript, critically reviewed the manuscript and approved the final manuscript as submitted. SDB contributed to the design of the learning community, critically reviewed and revised the manuscript and approved the final manuscript as submitted.
Funding This study was funded by Silicon Valley Community Foundation Grant ID: 2018-192032(5685)
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.