Article Text

Abstract
Background Surgical site infections (SSIs) are morbid and costly complications after elective colorectal surgery. SSI prevention bundles have been shown to reduce SSI in colorectal surgery, but their impact on organ space infections (OSI) is variable. Adoption of an evidence-based practice without an implementation strategy is often unsuccessful. Our aim was to successfully implement an OSI prevention bundle and to achieve a cost-effective reduction in OSI following elective left-sided colorectal operations.
Methods The Translating Research into Practice model was used to implement an OSI prevention bundle in all patients undergoing elective left-sided colorectal resections by a single unit from November 2018 to September 2019. The new components included oral antibiotics with mechanical bowel preparation, when required, and use of impermeable surgical gowns. Other standardised components included alcoholic chlorhexidine skin preparation, glove change after bowel handling prior to wound closure with clean instruments. The primary outcome was OSI. Secondary outcomes included bundle compliance, unintended consequences and total patient costs. Outcomes were compared with all patients undergoing elective left-sided colorectal resections at the same institution in 2017.
Results Elective colorectal resections were performed in 173 patients across two cohorts. The compliance rate with bundle items was 63% for all items and 93% for one omitted item. There was a reduction in OSI from 12.9% (11 of 85) to 3.4% (3 of 88, p<0.05) after implementation of the OSI prevention bundle. The average cost of an OSI was $A36 900. The estimated savings for preventing eight OSIs by using the OSI bundle in the second cohort was $A295 198.
Conclusion Successful implementation of an OSI prevention bundle was associated with a reduced rate of OSI after elective colorectal surgery. The OSI bundle and its implementation were cost-effective. Further study is required to investigate the sustainability of the OSI prevention bundle.
- surgery
- quality improvement
- infection control
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The prevention of surgical site infection (SSI) is an ongoing healthcare priority. SSIs are a costly burden to healthcare providers and patients, associated with increased morbidity, length of hospital admission and use of additional healthcare resources. Colorectal surgery has one of the highest rates of postoperative SSI, with published rates ranging from 15% to 30%.1 2 Left-sided colonic resections and rectal resections in particular have a higher incidence of postoperative SSI compared with right-sided colonic resections, potentially due to longer operating times, higher rates of exposure to preoperative radiotherapy and increased likelihood of ostomy creation.3 4 It is imperative to investigate if any intervention can decrease the rate of SSI in this group of patients.
SSI may be reported as an overall rate or stratified into superficial, deep and organ space infection (OSI) rates. SSI prevention bundles have been shown to reduce superficial SSIs in colorectal surgery, but their impact on deep and OSI is variable.5–8 Significant heterogeneity exists between studies investigating the utility of SSI prevention bundles. Study design, patient population, bundle components and compliance rates vary widely. A meta-analysis and systematic review showed that bundles with sterile closure trays, oral antibiotics with mechanical bowel preparation and preclosure glove changes had significantly greater overall SSI risk reduction; however, it did not further stratify SSI risk into superficial, deep or OSI.1
Care bundles to reduce the rate of SSIs have been implemented on a national level in the USA through the Surgical Care Improvement Program and in England as part of the Department of Health High Impact Intervention programme.9 10 To our knowledge, there has only been a single study on the use of an SSI prevention bundle in colorectal surgery in the Australian setting. Although they observed a decrease in SSI rate, the focus was on feasibility of implementation rather that outcomes of SSI.11
We identified a high rate of OSI following colorectal surgery in our colorectal unit as well as a gap between our practice and an evidence-based approach to reducing SSI after colorectal surgery. The aim of this study was to determine if successful implementation of an OSI prevention bundle, introduced in an Australian institution, reduced the rate of OSI following elective left-sided colorectal operations and to evaluate the cost-effectiveness of the bundle.
Methods
We formulated an implementation strategy to develop and adopt an evidence-based sepsis bundle to reduce OSI after colorectal surgery in our institution. The Standards for Quality Improvement Reporting Excellence 2.0 guidelines were used in study development and reporting.12
Context
The colorectal unit has seven surgeons, all members of the Colorectal Surgical Society of Australia and New Zealand, providing tertiary public hospital services for a culturally and linguistically diverse population.
Reporting of SSI is based on coding data and is voluntarily reported by public hospital infection control committees. Infections presenting after discharge are not captured. The data are not reported to the colorectal unit. Unlike in the USA, the rate of any healthcare-associated infections is not part of the hospital funding formula. In Australia, the state governments provide capped funding to public hospitals based on discharge coding.
Bowel preparation before colorectal surgery is selective and antibiotic use with bowel preparation is rare. Although neomycin is manufactured in Australia for export, it isnot readily available. A standardised bowel preparation and an enhanced recovery programme within the unit had been discussed but not audited—at baseline, surgeons acted autonomously.
Study development
Our Translating Research into Practice (TRIP) implementation model comprised a stakeholder analysis and was followed by the four E’s strategy (educate, engage, execute and evaluate) to develop and use a colorectal sepsis bundle.13 This process involved a multidisciplinary, interprofessional group including surgeons, operating room nurses, managers, anaesthetists, infection control nurses and physicians, preadmission clinic staff, ward nurse unit managers and nurses, pharmacists and hospital medical officers.
The baseline data and evidence from the literature were presented in meetings for the surgical unit, morbidity and mortality meetings, infection control committee, safe care committee as well as individual meetings with key stakeholders. An iterative process between staff was used to reach an agreement on the components of the colorectal sepsis bundle and the evaluation process. This process took 12 months but facilitated education, engagement and agreement of key stakeholders.
Neomycin was approved on an individual patient basis via the Special Access Scheme of the Pharmaceutical Benefits Scheme administered by the Therapeutic Goods Authority (TGA). No additional resources were provided to the surgical unit. An education package, checklist for the operating room and a dedicated data collector (NT) were developed prior to commencement.
Data were monitored monthly and feedback to the unit was given for opportunity to adapt the protocol. Adaptions included regular education sessions for each new rotation of hospital medical officers, a template for neomycin approvals and further education to nursing staff regarding the different grades of surgical gowns.
Study design
This was a single institution cohort study undertaken by the colorectal unit. The high rate of OSI in our unit had been identified in consecutive patients by using International Classification of Diseases coding, audit data and chart review from March 2017 to October 2017; this group formed the baseline (prebundle) cohort. The OSI prevention bundle was implemented and used from November 2018 to September 2019. These patients formed the (post) bundle cohort. Data were prospectively collected for retrospective analysis.
Factors that could influence the rate of SSI were collected. These included patient demographic data such as age, gender, body mass index, American Society of Anesthesiologists physical status grade, diabetes status, smoking status and preoperative radiotherapy. Indication for procedure, type of resection and operative method (laparoscopic vs open) was also collected. Patient outcomes of OSI rate and anastomotic leak were collected based on CT scan with rectal contrast. CT scans were performed only for clinical suspicion of complications based on routine assessment and blood tests. Follow-up was complete on all patients at 90 days. To measure the effectiveness of the implementation of the intervention, process measures were reported as compliance with bundle elements on an individual and aggregated basis.
The primary outcome of the intervention was OSI as defined by the Centers for Disease Control and Prevention criteria.14 Secondary outcomes were anastomotic leaks, length of stay (LOS) and other complications (Clavien-Dindo grade 3 and above), as well as total cost per patient. Unintended consequences were recorded, including reactions to oral antibiotics and Clostridium difficile infections.
Inclusion and exclusion criteria
All patients who underwent an elective left-sided colorectal operation under the colorectal unit during the study periods were included. Operations included laparoscopic and open approaches for left-sided colectomy and/or proctectomy with or without anastomosis. Patients who had pre-existing OSI were excluded.
SSI prevention bundle
The bundle was implemented in November 2018 and comprised 12 elements (box 1). These elements were based on a combination of strong evidence-based interventions and common-sense interventions with the aim of reducing postoperative OSI. Interventions such as the use of prophylactic intravenous antibiotics, use of skin clippers for hair removal and use of alcoholic chlorhexidine for skin preparation have strong evidence for reduction of SSI.1 8
Surgical site infection (SSI) prevention bundle components
Administration of oral antibiotics (3000 mg neomycin and 1200 mg metronidazole) with mechanical bowel preparation, if mechanical bowel preparation deemed to be required by the treating surgeon.*
Discussion of bundle during surgical team time out.*
Hair removal with clippers.
Skin preparation using 2% chlorhexidine in 70% alcohol.
Preoperative dosing of intravenous prophylactic antibiotics 2 g cefazolin and 500 mg metronidazole.
Repeat dosing of intravenous antibiotics if the operation was over 4 hours.
Use of Association for the Advancement of Medical Instrumentation (AAMI) level III surgical gowns by surgical team.*
Use of wound protector.
If a stapled side-to-side anastomosis was performed, two separate linear staplers were used to prevent contamination from luminal content.*
Quarantine of contaminated instruments on a separate trolley.*
Change of gloves by surgical team after bowel handling, prior to fascial closure.
Clean closing instruments used for fascial and skin closure.*
*Bundle elements that were new to our institution.
Bundle elements without strong evidence but based on principles that would decrease contamination of the abdominal cavity and wound were also included, such as the use of wound edge protectors and glove change after bowel handling. Our staff preferred quarantining contaminated instruments and use of separate clean closing instruments to a separate closing tray. The use of higher grade surgical gowns was implemented after surgeons at our institution noticed strikethrough of patient blood and bodily fluid through the gown sleeves during longer and more technically difficult rectal dissections. Upgrading the surgical gowns from level II to level III gowns was consistent with the Food and Drug Administration standard15 and eliminated strikethrough.
Bundle data were collected using a checklist and entered into a spreadsheet. Compliance rates were continuously measured and reviewed monthly, enabling ongoing feedback to medical and nursing staff about bundle implementation. Costing data were retrieved from institutional clinical costing service for each patient episode, after finalisation of data for each financial year. Costing data were only obtained for the prebundle cohort to avoid the need for adjustment for inflation when comparing between years. Readmissions specifically related to OSI were included. Readmissions to restore intestinal continuity were excluded.
Analysis
OSI rates in the prebundle and postbundle groups were compared using the χ2 test for categorical variables. Demographic characteristics between the two groups were compared using the χ2 test for categorical variables and the Student’s t-test for continuous variables. Continuous variables were described using the mean and SD. Costing data were compared using the Mann-Whitney U test. A p value <0.05 was considered significant.
Results
Patient characteristics
A total of 173 patients were included in the study, with 85 in the prebundle group and 88 in the bundle group (table 1). Patient groups before and after implementation of the bundle were similar, including rates of diabetes, smoking status, use of radiotherapy and minimally invasive surgery. The majority of patients underwent minimally invasive restorative surgery for colorectal cancer.
Patient characteristics
Compliance with SSI prevention bundle
Compliance
The overall compliance rate with the bundle was 62.5%, while the compliance rate with at least 11 out of 12 elements was 93.2% (table 2). The compliance rate with the use of oral antibiotics and mechanical bowel preparation where applicable was 84.9%. Compliance rates of 100% were achieved for hair removal with clippers, use of alcoholic chlorhexidine for skin preparation, administration of preoperative prophylactic intravenous antibiotics, redosing of prophylactic intravenous antibiotics if the procedure lasted over 4 hours, use of two linear staplers in a side-to-side anastomosis and quarantine of closing instruments.
Patient outcomes
Implementation of the OSI prevention bundle was associated with a significant decrease in OSI (12.9% vs 3.4%, p<0.05) (table 3). There was no significant difference found in the number of anastomotic leaks, which is a subgroup of OSI. There were also no statistically significant differences observed in the LOS, complications graded Clavien-Dindo grade 3 and above and rate of return to operating theatre. No unintended consequences of bundle implementation were observed, including any clinically detected C. difficile infections or allergic reactions attributable to the addition of oral antibiotics to mechanical bowel preparation.
Patient outcomes
Costing
Prior to implementation of the bundle, the median estimated costs for admissions and related readmissions were significantly higher in the patients who suffered OSI (figure 1). One readmission for OSI occurred at another hospital from which costs were unattainable. The median cost for the 11 patients with OSI was $A58 739 compared with $A21 834 for each of the 74 patients without OSI (p<0.01). Therefore, the average additional cost for a patient with OSI was $A36 905. The cost of adding new items in the bundle (grade 3 gown ×2 and oral antibiotics) was $5.29 per patient. Using costing data from 2017, eight instances of OSI would have been avoided through use of the OSI prevention bundle, saving an estimated $A36 899 in each instance, or $A295 198 total. Considering the entire cohort of patients, the median LOS for the 159 patients without OSI was 6 days (IQR 4–9), compared with 16 days (IQR 11–23) for the 14 patients with OSI (p<0.01).
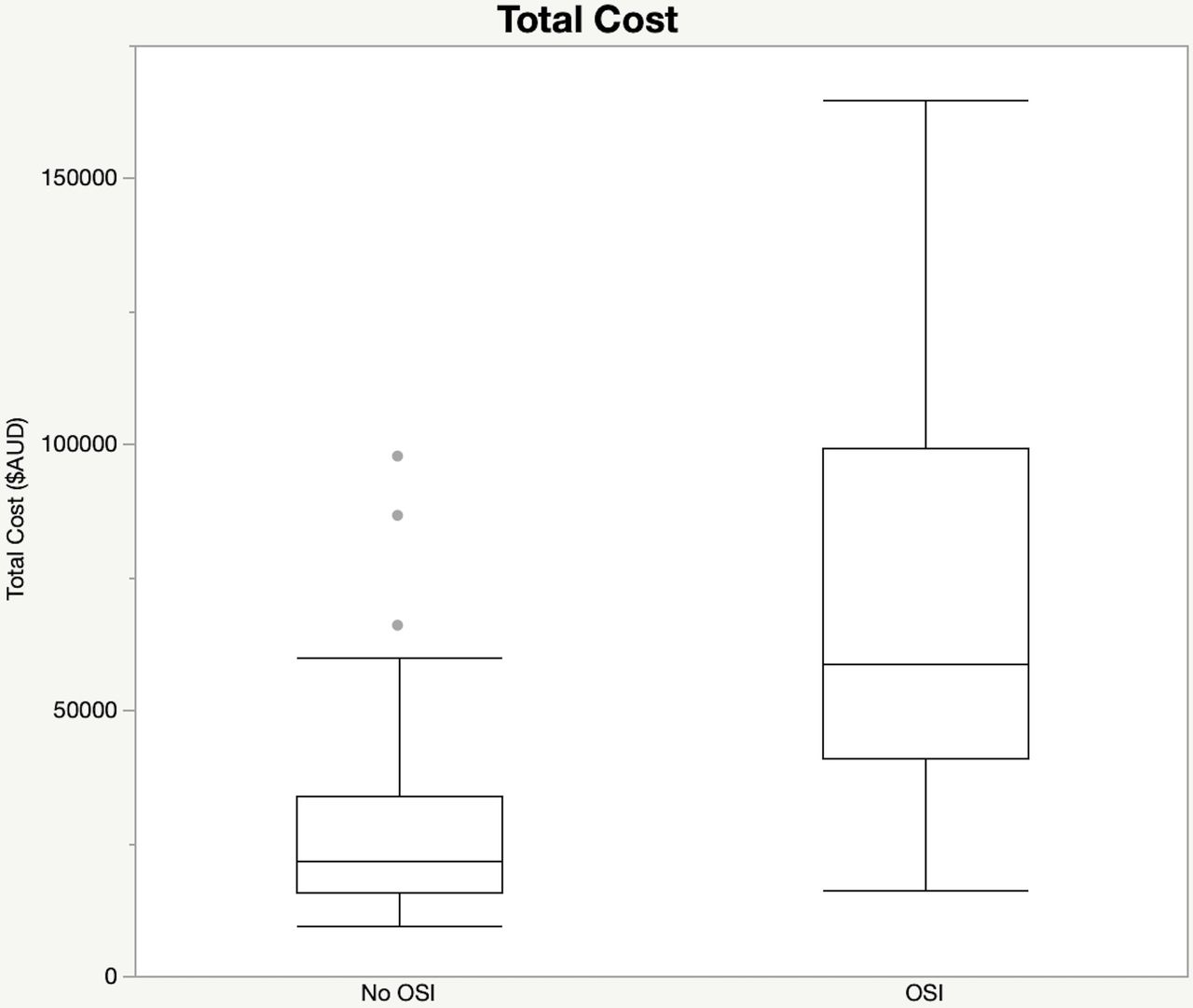
{kind=link}
Total costs for patient admissions in 2017 prior to implementation of the bundle. OSI, organ space infection.
Discussion
Healthcare interventions often fail due to a lack of engagement and feedback from front-line providers.16 17 We used the TRIP model to engage a multidisciplinary team in collaborative design and use of the sepsis bundle.13 One of the strengths of this study was the successful implementation of the OSI bundle.
Our study shows that a bottom-up initiative with a multidisciplinary team approach to bundle design and implementation can institute a positive cultural change towards OSI prevention. With regard to bundle implementation, an inverse relationship between compliance rates and SSI rates has been previously demonstrated.18 Our overall compliance rate with the OSI prevention bundle was 62.5%. Compliance rates with individual elements of the bundle ranged from 84.9% to 100%. The TGA restriction on the prescription of oral neomycin remains a challenge. We found with staff turnover that it was essential to have an appointed surgical team leader overseeing the use of the bundle and providing education and feedback to all staff involved in its use. The Institute for Healthcare Improvement describes executive sponsorship as a contextual element associated with successful teams; our study did not have an executive sponsor.19 Ongoing surveillance is required to measure the sustainability of results with the OSI prevention bundle.
Postoperative OSI is a morbid and costly complication after colorectal surgery, with higher rates experienced in left-sided colonic resection and rectal resections.3 4 One study at the Cleveland Clinic demonstrated a significant reduction in OSI rate with the use of an SSI prevention bundle; however, their patient population had a high proportion of inflammatory bowel disease with associated steroid use, undergoing complex pouch surgery.5 This differs greatly from the patient population treated by the colorectal surgical unit at our institution. Most studies investigating the use of a care bundle for the prevention of SSIs in colorectal surgery fail to conclusively demonstrate an effect on OSI.6 8 18 20 21 In this study, we have demonstrated that the implementation of an OSI prevention bundle can significantly reduce the rate of OSI in elective left-sided colorectal operations.
The new items for our unit in the bundle group were the introduction of oral antibiotics with use of mechanical bowel preparation (only if mechanical bowel preparation was indicated), the use of AAMI grade 3 surgical gowns and putting aside dedicated clean instruments for use at the end of the case to close the wound.
The addition of oral antibiotics to mechanical bowel preparation has been associated with reduced anastomotic leaks, SSI rates and ileus in elective colorectal surgery.22 23 Access to oral neomycin for use as bowel preparation prior to colorectal surgery is limited in Australia, requiring individual application for TGA approval for use in each patient. This study supports the use of oral antibiotics in addition to mechanical bowel preparation as part of a bundle to reduce OSI in elective colorectal surgery, and makes an argument for easier access to and prescribing of neomycin in Australia.5 Limited evidence is available about the efficacy of oral antibiotics in the absence of mechanical bowel preparation, and further investigation is required to measure an effect on SSI outcomes.
Longer operation times are an independent risk factor for SSI in rectal surgery; however, it would be difficult to determine if the grade of surgical gowns used was a contributing factor leading to higher rates of OSI.3 4 24 Nonetheless, this finding is a pertinent reminder that surgeons have to be at the front line of quality improvement measures to better patient care and outcomes.
While reducing complications has intrinsic merit for patients and practitioners, most hospitals require a business case for new initiatives. Most OSI bundle items required consistency of behaviour rather than new consumables. The cost of the new items in the OSI was small: $A5.29 per patient. The projected savings was based on the cost estimate of $A36 905 per OSI. This is a slight underestimate as one readmission at another hospital was not included as the cost was not available. For our second cohort, the OSI bundle reduced the expected number of OSI by 8, saving $295 198. Bed-days saved have also been a proposed method of costing hospital-acquired infections.25 In our study, the median LOS for patients without an OSI was 6 days compared with 15.5 days for patients with an OSI (p<0.01). Both outcomes support the use of the OSI bundle as a cost-effective strategy.
Several limitations exist with this study. First, being a single-centre cohort study, we are unable to correct for all confounders contributing to OSI rates. Second, due to the nature of a bundled set of interventions, we are unable to determine which elements of the bundle have more of an effect on OSI than others. Third, the rate of superficial SSI was not collected in this study, as these data were not able to be accurately captured. This would have required follow-up over 30 days postoperatively, mostly in the community. The impact of SSI prevention bundles on superficial SSI has also been extensively studied previously. Lastly, the diagnosis of OSI was based on CT scans with rectal contrast. CT scans were requested based on clinical concerns and were not routinely performed on every patient. However, all patients were followed at 90 days to minimise the chance of a missed OSI, which we believe was a pragmatic approach.
This study may assist other institutions to reduce OSI by using an implementation framework to introduce evidence-based practice.17 We have established the cost of an OSI to assist units that develop a business case for change. Limited access to oral neomycin remains a barrier to implementation of this bundle. More studies are needed to demonstrate sustained improvement in OSI rates.
Conclusion
We successfully implemented an OSI prevention bundle, which was associated with a significant reduction in OSI rate in elective left-sided colorectal surgery in an Australian institution. This process was cost-effective. Further investigation is required to demonstrate if this is transferable across multiple centres.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Ethics approval
Ethics approval for this study was obtained from the institutional ethics board of Western Health (QA 2018.87).
References
Footnotes
Contributors Concept and design: IF, SG, MH. Acquisition, analysis or interpretation of data: IF, NT, MH, JY. Statistical analysis: IF, NT, MH. Drafting of the manuscript: IF, NT, MH. Critical revision of the manuscript for important intellectual content and approval of final version: IF, NT, MH, SG, JY. Supervision: IF, JY. IF is the corresponding author and had full access to all of the data in the study, and takes responsibility for the integrity of the data and the accuracy of the data analysis and is guarantor for this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.