Article Text

Abstract
Rehabilitation programmes can be delivered to patients receiving acute care (‘in-reach rehabilitation’) and/or those who have completed acute care but experience ongoing functional impairments (‘subacute rehabilitation’). Access to these programmes depends on a rehabilitation assessment, but there are concerns that referrals for this assessment are often triggered too late in the acute care journey. We describe a Proactive Rehabilitation Screening (PReS) process designed to systematically screen patients during an acute hospital admission, and identify early those who are likely to require specialist rehabilitation assessment and intervention. The process is based on review of patient medical records on day 5 after acute hospital admission, or day 3 after transfer from intensive care to an acute hospital ward. Screening involves brief review of documented care needs, pre-existing and new functional disabilities, the need for allied health interventions and non-medical factors delaying discharge. From May 2017 to February 2019, the novel screening process was implemented as part of a service redesign of the rehabilitation consultation service. Four thousand consecutive screens were performed at the study site. Of those ‘ruled in’ by screening as needing a rehabilitation assessment, 86.0% went on to receive inpatient rehabilitation interventions. Of those ‘ruled out’ by screening, 92.1% did not go on to receive a rehabilitation intervention, while 7.9% did receive some form of rehabilitation intervention. Of all patients accepted into a rehabilitation programme (n=516), PReS was able to identify 53.6% (n=282) of them before the acute care teams made a referral (based on traditional criteria). In conclusion, we have designed and implemented a systematic, PReS service in one metropolitan Australian hospital. The process described was found to be time efficient and feasible to implement in an acute hospital setting. Further, it appeared to identify the majority of patients who went on to receive formal inpatient rehabilitation interventions.
- rehabilitation
- quality improvement
- process mapping
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Rehabilitation programmes have been developed to be provided while a patient is still receiving acute care (‘in-reach rehabilitation’) and/or after a patient has completed acute care but cannot be discharged from hospital due to ongoing functional impairments (‘inpatient (subacute) rehabilitation’).1 The former is still an emerging model of care but the latter is well established in Australia, with around 125 000 episodes of care provided via this model in 2019.2
The authors work in the Department of Rehabilitation Medicine in a tertiary, public teaching hospital in Sydney, Australia, with a capacity of 400 beds. The rehabilitation consult service provides assessment and triaging of patients to either in-reach rehabilitation and/or inpatient (subacute) rehabilitation. This assessment is done at the request of the acute treating medical or surgical team. There is growing consensus that rehabilitation assessments should be performed as soon as practical during a hospital admission.3 4 But in reality, the referrals for these assessments are often triggered too late in the acute care journey.5 6 Anecdotally, the clinicians in this rehabilitation consult service observed that some patients who would have been appropriate for rehabilitation were not considered for referral by their acute treating teams (especially for in-reach rehabilitation programmes). Further, referrals were often received at a late stage in a patient’s acute hospital admission, prompting the authors to consider designing a more systematic method of identifying likely rehabilitation candidates early during a hospital admission.
Late referrals for rehabilitation assessment may negatively impact on patient flow and, in turn, on patient outcomes. It has been estimated that patients spend 12.0% of days admitted to an acute hospital ward waiting for a rehabilitation bed in Australia.7 Waiting for inpatient rehabilitation services has also been identified as a major problem in other countries, which may lead to delays in accessing appropriate care and so increase the costs of hospitalisation.8–10 Delayed transfer to rehabilitation has also been associated with poorer functional outcomes.11 12
The ‘gold standard’ process would be to conduct formal rehabilitation assessments on all hospital admissions to identify those patients likely to require and benefit from rehabilitation programmes. However, such a process would be expensive, labour-intensive and impractical to implement on a wide scale. This gave the impetus for exploring whether such a process could be achieved through screening in a busy hospital setting like ours.
Background
To our knowledge, there are only two screening tools that have been developed in Australia with the aim of predicting subacute inpatient rehabilitation as a likely discharge disposition after completion of an acute care hospital admission. Both were developed for specific patient populations, namely, one for elective joint replacement (the Risk Assessment and Predictive Tool or RAPT)13–15 and the other for lower limb orthopaedic fractures.16 The RAPT was reported to have a predictive accuracy of 73.4% for identifying rehabilitation needs preoperatively but is only applicable to patients undergoing elective joint replacements. It has not been tested postoperatively in the acute hospital setting. The latter tool, while developed for a broader orthopaedic trauma population, requires complex formula calculations to derive a patient’s probability of requiring rehabilitation, making it less practical for routine and rapid clinical use, and it is yet to be prospectively tested in busy acute hospital settings.
In the USA, a tool called the Activities Measure for Post-Acute Care 6-clicks has been developed and validated.17 It is a short measure of basic mobility and when used within 48 hours of admission by a physiotherapist, it has been shown to be able to predict whether a patient will be discharged home (area under the receiver operating characteristic curve 0.78).18 This tool has not been evaluated within the Australian healthcare system to date. Further, this tool was designed to predict discharge home to a private residence rather than predicting more specifically the likelihood of a patient requiring inpatient rehabilitation.
In the absence of a published simple and quick tool for the purpose of predicting rehabilitation needs for admitted patients with heterogeneous diagnoses, we chose to design from scratch a novel screening process to achieve this goal (ie, case finding of rehabilitation candidates early in the acute care journey).
Measurement
Usual care rehabilitation processes at the study site
At the study site, patients admitted to an acute medical or surgical ward are seen by single-discipline allied health professionals (eg, physiotherapy, occupational therapy) at the referral of their acute treating team according to individual patient need. This ward-based therapy is not considered to constitute a formal rehabilitation programme or episode of care, as it is not coordinated by rehabilitation physicians, nor multidisciplinary in nature.
Rehabilitation programmes, that is, multidisciplinary rehabilitation coordinated by a rehabilitation physician at the study site include:
In-reach (acute) rehabilitation. This is an emerging model of care in Australia,1 whereby a formal specialist rehabilitation episode is delivered to patients still receiving acute medical/surgical management on an acute hospital ward.
Inpatient (subacute) rehabilitation. This is a more traditional model of inpatient rehabilitation, whereby patients who are medically stable are transferred to a subacute rehabilitation unit.
Standard practice involves an acute medical/surgical team making a referral for rehabilitation assessment if they anticipate that their patient will benefit from a rehabilitation programme.
Implementing and measuring service redesign
In this project, the authors undertook a pragmatic redesign of the rehabilitation consultation service, with the aim of developing and implementing a standardised screening process to identify patients with heterogeneous diagnoses who may benefit from rehabilitation assessment early in the course of an acute hospital admission. Key features of the novel screening process were that it had to be time-efficient and practical for use in busy clinical settings, yet sensitive enough to identify patients likely to be accepted into rehabilitation programmes by rehabilitation physicians.
To evaluate the feasibility of implementing the novel screening process, measurement of the time taken to perform the screening was conducted, and barriers to screening were explored. To explore the clinical utility of screening, the proportion of patients screened as likely to need rehabilitation, who went on to receive an inpatient rehabilitation intervention, was calculated. The number of patients who were referred to rehabilitation via traditional referral methods was compared with the number who were identified as likely to require rehabilitation via proactive screening.
Design
Developing a Proactive Rehabilitation Screening (PReS) process
On the basis of clinical literature review,19–23 several domains were identified by the authors to be pertinent to rehabilitation needs. These included:
New functional dependency, indicated by an increased level of physical assistance required for mobility, personal care and/or the need for assistive equipment (such as a mobility aid).
Need for allied health interventions in the acute care setting (such as physiotherapy, occupational therapy, speech pathology and other disciplines).
The presence of pre-existing physical and/or cognitive disabilities.
‘Medical stability’ (no medical interventions requiring acute care in hospital for at least 24 hours prior) but non-medical factors preventing or delaying discharge (such as psychosocial barriers).
Using these domains, a method of proactive screening via file review was developed by the authors. The screener was asked to briefly review a patient’s medical record. This review included examination of documented care needs and progress over the preceding 5 days of a patient’s acute hospital admission, with particular focus on the domains listed above.
After reviewing the medical records, the screener was asked to decide on one of three possible outcomes: (1) ‘ruled-in’, as appropriate and likely to need a rehabilitation programme; (2) ‘ruled-out’, as inappropriate and/or unlikely to need a rehabilitation programme; (3) ‘rescreen in 7 days’, where there is notable ambiguity and a definitive decision needs to be made at a subsequent screening time point.
Patients with functional dependency who required high levels of allied health interventions were generally ‘ruled-in’ by screening. This included those who required high levels of physical assistance (assistance from multiple people) to mobilise or perform daily activities; those who required intensive doses of therapy; and/or those who required intervention from multiple allied health disciplines. The patients who were ‘ruled-out’ by screening were those who required no or minimal allied health intervention, who were in acute care wards receiving medical or surgical interventions, primarily and those who were largely independent.
For those who were ‘ruled-out’ but remain admitted to hospital after 28 days, they were eligible for rescreening at day 28 of admission with only two possible outcomes: ‘ruled-in’ or ‘ruled-out’. For patients who were admitted or readmitted to intensive care after screening, they were eligible for rescreening when they were discharged from intensive care and returned to an acute ward, but this was considered a new screening episode.
Screening was designed to take place on day 5 of admission to an acute hospital ward, or 3 days after discharge from intensive care to an acute ward. For intensive care survivors who are transferred to an acute ward prior to the fifth day of admission, screening was delayed until they reach a minimum length of stay (LOS) of 5 days. Where day 5 fell on a weekend, screening was performed on the next consecutive weekday (at day 6 or 7).
This screening window commencing on the fifth day of admission was chosen a priori based on the average LOS of patients admitted to Australian public hospitals (mean 5.7 days).24 On the basis of clinical experience, it was assumed that patients with short hospital admissions (<5 days) would be unlikely to need inpatient rehabilitation; therefore, they would be less likely to benefit from screening. As this group accounted for 50% of all Australian hospital admissions, excluding them from a proactive screening process served to streamline the workflow of screening and focus screening efforts on the patient population most likely to benefit/require inpatient rehabilitation.
The screening process was intended to be simple to perform and to not require specialist clinical or rehabilitation expertise. The process was designed to be able to be completed by a variety of people, namely, those with experience reviewing and interpreting clinical documentation, including medical staff, nurses, allied health professionals and clinical researchers.
Strategy
Implementing a PReS service
From May 2017 to February 2019, a PReS service was softly launched. Screening was performed on each weekday by a rehabilitation nurse (OM). All consecutive patients who were admitted to hospital for at least 5 days, and under 75 years of age, were screened. Patients over the age of 75 years were not included in this particular study cohort (as assessment for rehabilitation programmes in patients ≥75 years is managed by the geriatric medicine service at this site). Admissions under psychiatric, drug and alcohol, and palliative care services were also excluded.
Patients who were ‘ruled-in’ by PReS were assessed by a rehabilitation physician (JW) or rehabilitation registrar (specialist doctor in training). For patients who were ‘ruled-out’ by the screening process, their screening outcomes were not documented in the medical records, and as such, acute care teams were not aware of each patient’s screening status. Hence, screening did not influence usual care referral processes. Standard care continued throughout the study period, that is, all patients referred by their acute treating team were assessed by the rehabilitation physician or registrar according to usual practice, irrespective of their screening outcome.
A clinical rehabilitation assessment could result in three possible outcomes: (1) accepted for rehabilitation on the acute ward by the in-reach rehabilitation team; (2) accepted for rehabilitation and transferred to a subacute inpatient rehabilitation ward (either onsite or offsite); or (3) no inpatient intervention. The first two outcomes ((1) and/or (2)) were defined for our study purpose as an inpatient rehabilitation intervention. The latter (3) included any rehabilitation assessments for discharge planning purposes, outpatient rehabilitation and/or follow-up at outpatient rehabilitation medical clinics.
A minimum dataset was collected for each screening episode, including the following process and outcome measures: screening outcome (ruled-in, ruled-out, rescreen); the time to screening (days from admission); whether a rehabilitation referral was requested prior to screening; the type of rehabilitation intervention received (in-reach, subacute inpatient, or combination; or none); the time to subacute inpatient rehabilitation transfer (if applicable); and hospital discharge destination.
The time taken (in minutes) to conduct screening was collected over a subset of 10 consecutive screening days. This included the time taken for screening preparation, locating paper-based medical records, review of medical records and recording the screening decision.
The PReS service was launched as a quality initiative (clinical service redesign) and as such did not require individual patient consent to screen data routinely collected in hospital medical records. Rehabilitation assessments and treatments by rehabilitation clinicians are routinely used as part of standard clinical care at the study site and as such do not require written consent. Individual participant consent to review these records was not required as this was considered low risk and the minimal dataset extracted was comprised solely of routinely collected data fields.
Results
The flow of 4000 consecutive screening episodes is illustrated in figure 1. For those patients who were screened after transfer from intensive care (n=1051), screening occurred a median of 9.0 days (IQR 7.0–15.0) after hospital admission. For those admitted to the acute wards (n=2949), screening was achieved within the target timeframe of days 5–7 in 86.9% of cases (n=1604). As screening required access to a paper-based medical record, there were some occasions where the record was not available at the time of the daily screening round (eg, if being used by other clinical teams, or if the patient had been transferred off the ward for clinical investigations). Where this occurred, another attempt at screening would be made the next working day.

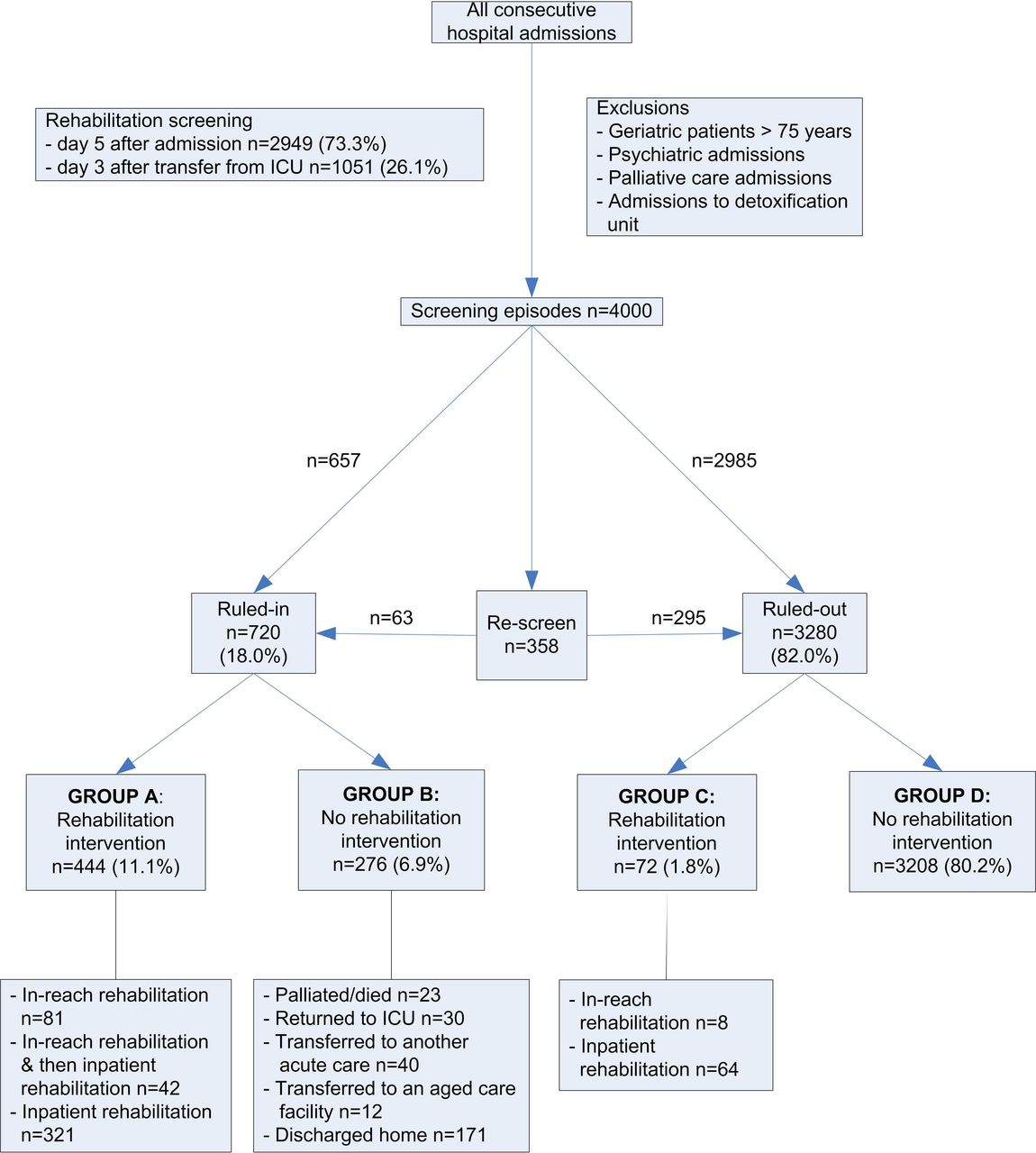{kind=link}
Patient flow. ICU, intensive care unit.
The time required for daily screening rounds, collected over a period of 10 consecutive weekdays, is summarised in table 1. On average, 3.6 min was required for each screening episode. It was the authors’ impression that no more than 15 min of preparation time was required each day to identify the patients who required screening.
Time taken for screening over 10 consecutive weekdays
Of the patients who were ‘ruled in’ by screening, 86.0% went on to receive an inpatient rehabilitation intervention. Of those ‘ruled out’ by screening, 92.1% did not go on to receive a rehabilitation intervention, while 7.9% did receive some form of inpatient rehabilitation. Possible reasons to explain ‘false negative’ screening outcomes (Group C, n=72) were reviewed by a rehabilitation physician. The two most common reasons documented were that (1) the patient was functionally independent for discharge home but not confident or too anxious to leave hospital (n=13); and (2) the patient was due for rescreening in 7 days, but was referred to rehabilitation by their acute care team according to standard care processes before rescreening could be conducted (n=22). The remainder (n=37) were due to errors in screening (ie, a full rehabilitation assessment would have come to a decision of ruling that person in), poor documentation of care needs in the medical record (limiting the accuracy of screening) and difficulty screening with respect to more specialised rehabilitation needs (such as cognitive rehabilitation and rehabilitation for functional neurological disorders).
The premise of screening is that it allows patients to be identified earlier so that rehabilitation interventions can be delivered earlier. Of all the patients who were accepted into a rehabilitation programme (Groups A and C, n=516), PReS was able to identify 53.6% (n=282) before the acute care teams made a referral (based on traditional criteria). Among the 282 patients in Group A who were identified by screening and not referred via traditional methods, 68 (24.1%) of them were ready for transfer to a subacute inpatient rehabilitation unit within the day of screening.
We prospectively collected the waiting time duration for all patients who went to inpatient rehabilitation. In our cohort (n=412), 43.7% of patients were transferred on the same day they were considered ‘ready for rehabilitation’, and 76% were transferred to rehabilitation within 2 days; only 24% of patients had to wait more than 2 days for their transfer to rehabilitation. While local pre-implementation data on waiting times were not available in the present study, these figures were compared with published waiting times for patients admitted to two inpatient rehabilitation units in Melbourne (Australia) in 2008, where routine referral processes were being used (n=360).7 This study reported that 27.8% of patients were transferred on the same day they were considered ‘ready’ for rehabilitation by the rehabilitation consult service, and 29.4% had to wait more than 2 days for their transfer. Thus, waiting times observed in our study appeared to be favourable by comparison. Our data included patients referred to both internal and external rehabilitation facilities (including specialist offsite brain and spinal injuries units), while the published Melbourne cohort reported on internal rehabilitation admissions only. Given that waiting times to access external rehabilitation units can often by prolonged and are not under the control of the rehabilitation service, it is possible that the benefits of screening on waiting times may be even more pronounced when considering internal rehabilitation admissions only.
The present study focused on the predictive outcome defined as either rehabilitation delivered by an in-reach team in acute care or inpatient rehabilitation in a subacute rehabilitation unit. However, we also conducted separate analyses were the outcome was defined as subacute inpatient rehabilitation only (not in-reach rehabilitation) because many Australian hospitals only provide the traditional subacute inpatient model of rehabilitation. For these analyses, those patients who received in-reach rehabilitation only (and did not need inpatient rehabilitation) in Group A (n=81) were reclassified as false positive (Group B). When predictive outcome was defined as subacute inpatient rehabilitation only, 85.0% of all patients ‘ruled in’ by screening went on to receive a rehabilitation intervention, while 98.0% of those patients ‘ruled out’ by screening did not receive rehabilitation. This is likely a conservative measure of screening accuracy as arguably, many of the patients who received in-reach only may have required inpatient rehabilitation if they did not receive such a service.
Lessons and limitations
This project has demonstrated that it is feasible to implement a PReS process in the acute hospital setting. The PReS process was simple, quick to perform and able to be implemented with limited additional staff time or resources. In this preliminary implementation at one hospital, screening appeared to be able to identify early during admission those patients who would go on to receive an inpatient rehabilitation intervention during their hospital admission. The screening process we describe is applicable to a broad patient demographic and suitable for use with a variety of clinical diagnoses.
We have demonstrated that proactive screening conducted on day 5 of an acute hospital admission can identify 53.6% of all patients who would be accepted into rehabilitation programmes earlier than traditional referral processes. This is congruent with data from one Australian study, which reported that a median of 7 days (IQR 4–13) typically elapses between acute hospital admission and referral for rehabilitation, under routine processes.7 Data from one Australian study suggested that the time period between traditional method of rehabilitation referral to transfer to inpatient rehabilitation is typically a median of 4 days (mean 5.7±5.2 days).6 Thus, some patients may experience notable delays to accessing rehabilitation services, even after being referred and/or deemed suitable to receive them. Early identification of this group of patients may allow transfers from acute to subacute care in a timely manner and may reduce delays to rehabilitation commencement. A screening process similar to the one we described may assist patient flow within a hospital, leading to potential logistical and economic benefits for the health service as a whole.25 Although not specifically explored in this project, such a screening process may also minimise variations in access to rehabilitation services which currently rely on ad hoc referral processes.26–29
In the group of patients identified by screening alone (ie, those not referred via traditional methods), 24.1% were deemed ready by a rehabilitation physician for transfer to a subacute inpatient rehabilitation facility on the same day or within 1 day of screening. This finding is consistent with New et al,7 who found that 62.7% of the patients referred and assessed by a rehabilitation consult service was deemed to be ready for transfer to inpatient rehabilitation on the same day of assessment. In that particular study, 22.2% of all patients referred to inpatient rehabilitation were assessed by the consult service and deemed ready to transfer to rehabilitation on the day of referral. These findings, along with ours, suggest that the majority of people referred to rehabilitation do not require ongoing acute care at the time of referral, indicating that they could have been referred sooner for rehabilitation.5 This suggests that there may be hospital discharge processes that could be targeted for research into acute health service efficiencies.
In the present study, the flow of patients from acute care to inpatient rehabilitation appeared to be more timely than for a similar published cohort in Melbourne, Australia7; with more patients being transferred to rehabilitation on the day that they were ready (43.7% here vs 27.8% previously). In that study, the authors found that patients spent 12.0% (804/6682 days) of their overall acute hospital LOS waiting for a rehabilitation bed. Our screening process highlights potential opportunities to improve patient flow for acute hospital patients with rehabilitation needs.
The inpatient rehabilitation unit at the study site had traditionally operated at 95%–100% capacity prior to the implementation of screening. When introducing the new screening service, the in-reach and inpatient rehabilitation teams initially had concerns about how their service workflow may be impacted. Surprisingly, there were no negative impacts observed on either service, and both services were able to accommodate the flow of rehabilitation patients identified via screening. Throughout the project period, neither the in-reach rehabilitation team nor the subacute rehabilitation unit changed in staffing or bed numbers.
The efficiency of patient flow from acute to rehabilitation warrants further exploration. The authors hypothesise that early identification of patients through screening may have allowed the in-reach rehabilitation team to work with more patients in the acute setting, which may have prevented the need for a later inpatient rehabilitation episodes of care for some patients. This, in turn, may have freed up inpatient rehabilitation beds to allow the rehabilitation unit to manage receiving earlier patient transfers to rehabilitation than via the traditional rehabilitation referral route. We also hypothesise that patients who received in-reach rehabilitation earlier than the traditional referral method may have been functionally less dependent by the time they were admitted to inpatient rehabilitation and may have therefore required a shorter LOS.
Whether a patient receives various rehabilitation interventions is dependent not only on the rehabilitation physician’s assessment of clinical benefit but also on logistical considerations including service availability, patient stability, insurance status, patient preference and consent.30 Despite these potential confounding factors, here a method of proactive screening focused primarily on clinical need was able to identify a high proportion of patients (86%) who went on to receive rehabilitation interventions.
Screening did result in a modest additional workload for the rehabilitation consult service. Approximately an additional hour of work was required to prepare for and perform the screening on each weekday in our moderately sized, 400 bed hospital. There is also additional manpower required to perform a larger volume of rehabilitation assessments, including those for patients where inpatient rehabilitation did not eventuate or was not needed (Group B). While these could be perceived as ‘wasted’, arguably, many of the rehabilitation assessments for Group B were still valuable and of benefit to the acute care team in guiding discharge planning. Examples include assessments that advised on arranging palliative care referrals for those with limited life expectancy, sourcing aged care facilities for the older disabled patient or sourcing supported independent living for the younger disabled patient. In addition, these assessments may have been useful for arranging outpatient rehabilitation services for patients able to discharged back into the community from acute care. More research is required to see if the relatively low investment of upfront resources to perform screening may produce a significant overall reduction in the cost of hospital care for selected patients with high rehabilitation needs. This is important as busy clinicians will only implement screening if improved patient outcomes and/or cost savings for the healthcare system can be demonstrated (a concept called ‘impactability’31 in the predictive modelling literature).
It is important to note that the described screening process is not intended to replace traditional rehabilitation referral systems. Rather, we propose it could be used to augment and enhance usual processes. Acute care teams should continue to use clinical judgement to decide when to request a rehabilitation assessment if they identify a need. In the present study, we cannot exclude that the introduction of screening may have introduced inadvertent bias in routine referral behaviour, as some acute teams may have been aware that screening was occurring, and subsequently may have delayed or omitted making a referral. To minimise this potential problem, screening outcomes were deliberately not documented in the medical records, although we acknowledge this as a limitation.
The screening process should also not replace expert rehabilitation assessment by a physician to determine whether someone will benefit from a rehabilitation programme, but rather could be used to trigger rehabilitation assessments earlier than the traditional methods, and in a systematic way.
We have demonstrated that a quick medical record review can predict who needs rehabilitation interventions and that it is feasible to implement in one busy hospital. The authors plan to validate the screening process in a subsequent study in four hospitals using research staff (both rehabilitation trained and not rehabilitation trained) to perform screening independent of usual care practices. This will allow the proposed screening method to be validated while minimising some of the pragmatic biases inherent in this quality evaluation. It will also allow us to standardise the screening method and to evaluate the psychometric properties of the screening method such as inter-rater reliability.
Conclusion
In conclusion, we have successfully designed and implemented a systematic PReS service in one metropolitan Australian hospital. The novel screening process described was found to be time efficient and feasible to implement in a busy acute hospital setting. The screening process was able to be integrated into the existing rehabilitation consultation service, with no additional dedicated resources or staffing. This screening process was able to correctly identify the majority of patients who were likely to require a rehabilitation assessment early during their acute admission, and who subsequently received inpatient rehabilitation. Thus, screening may have the potential to positively impact on patient flow, rehabilitation accessibility and patient outcomes, and warrants further investigation.
Our experience with the described screening process is that it has provided our rehabilitation service with the opportunity to become involved in a patients’ hospital journey at an earlier stage. This has markedly enhanced care coordination and facilitated delivery of allied health interventions in a more coordinated fashion; earlier and more effective discharge planning for patients with complex needs (who typically have long admissions in acute care); and more timely referrals to external rehabilitation units and home-based care packages and/or rehabilitation. These preliminary findings support a role for PReS as a mechanism of improving patient flow through the hospital, care coordination and ultimately patient outcomes. Thus, we propose that systematic methods of rehabilitation screening should be further researched as clinical redesign strategies that may contribute to improved efficiencies in acute care and reduce overall healthcare costs.
Acknowledgments
The authors gratefully acknowledge Angela Vratsistas-Curto for comments on the manuscript.
References
Footnotes
Contributors JW conceived the study concept and developed the initial project plan. In consultation with OM, CS and SF, JW led the development of the novel screening process and implementation of the new process within the clinical rehabilitation consultation service at the study site. JW liaised with clinical stakeholders at the site regarding the new process. OM, CS and JW performed the rehabilitation screening and contributed to data collection. JW and CS reviewed data collection and performed the data analyses. JW drafted the initial manuscript. All authors critically reviewed and contributed to the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval Individual participant consent to participate was not required as this was a retrospective analysis of routinely collected data. This study was approved by the Human Research Ethics Committee of St Vincent’s Hospital, Sydney (LNR/17/SVH/388).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.