Article Text

Abstract
Background An academic safety-net hospital leveraged the federally funded state Delivery System Reform Incentive Payment programme to implement a hospital-wide initiative to reduce healthcare-associated infections (HAIs) and improve sepsis care.
Methods The study period was from 2013 to 2017. The setting is a 770-bed urban hospital with six intensive care units and a large emergency department. Key interventions implemented were (1) awareness campaign and clinician engagement, (2) implementation of HAI and sepsis bundles, (3) education of clinical personnel using standardised curriculum on bundles, (4) training of key managers, leaders and personnel in quality improvement methods, and (5) electronic medical record-based clinical decision support. Throughout the 5-year period, staff received frequent, clear, visible and consistent messages from leadership regarding the importance of their participation in this initiative, performing hand hygiene and preventing potential regulatory failures. Several process measures including bundle compliance, hand hygiene and culture of safety were monitored. The primary outcomes were rates of central line-associated bloodstream infection (CLABSI), catheter-associated urinary tract infection (CAUTI), surgical site infection (SSI) and sepsis mortality.
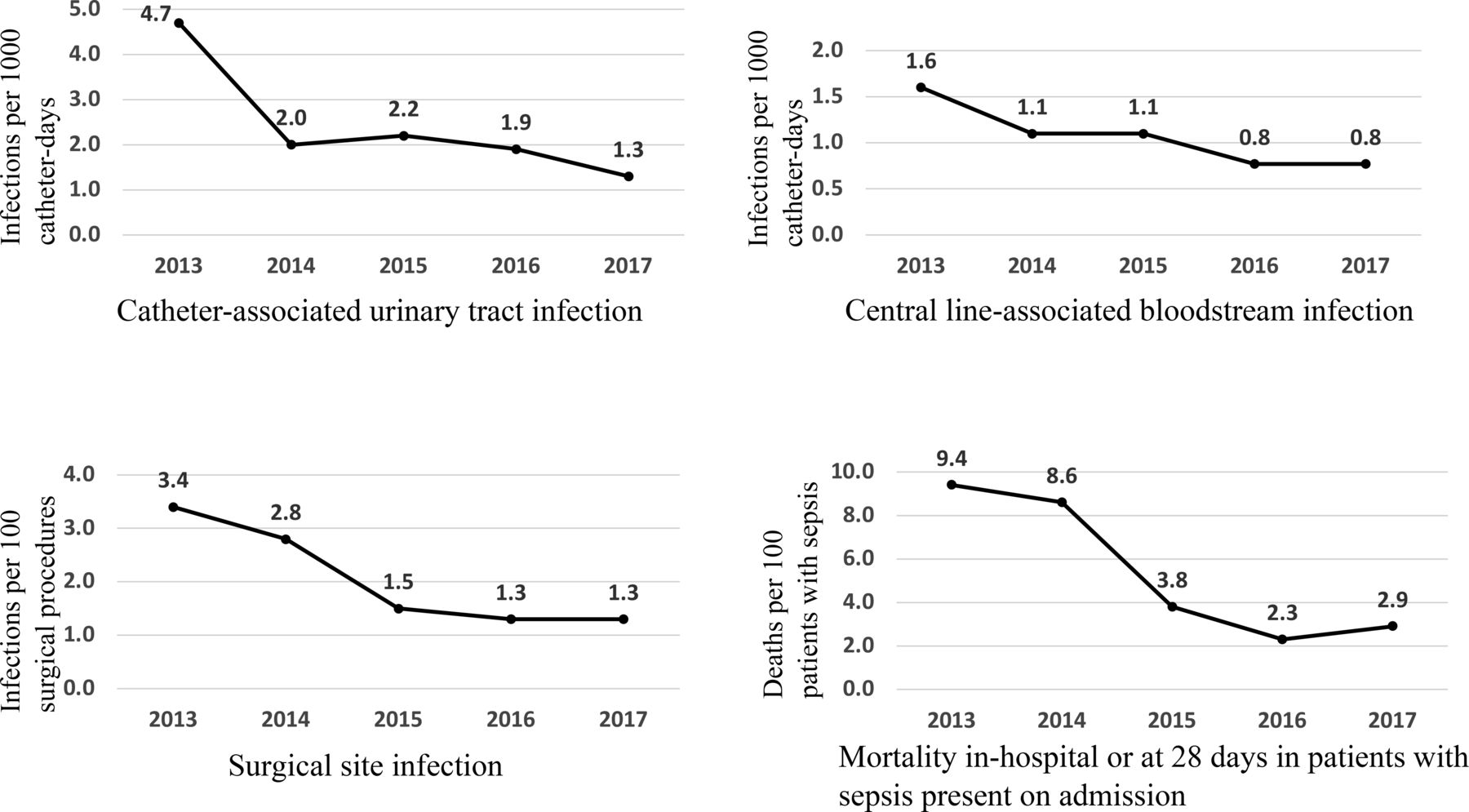
Results From 2013 to 2017, the hospital-wide rates of HAI reduced: CLABSI from 1.6 to 0.8 per 1000 catheter-days (Poisson regression estimate: −0.19; 95% CI −0.29 to −0.09; p=0.0002), CAUTI from 4.7 to 1.3 per 1000 catheter-days (−0.34; −0.43 to −0.26; p<0.0001) and SSI after 18 types of procedures from 3.4% to 1.3% (−0.29; −0.34 to −0.24; p<0.0001). Mortality of patients presenting to emergency department with sepsis reduced from 9.4% to 2.9% (−0.42; −0.49 to −0.36; p<0.0001). Adherence to bundles of care and hand hygiene and the hospital culture of patient safety improved. Results were sustained through 2019.
Conclusion A hospital-wide initiative incentivised by the Delivery System Reform Incentive Payment programme succeeded in reducing HAI and sepsis mortality over 5 years in a sustainable manner.
- patient safety
- healthcare quality improvement
- nosocomial infections
- health policy
- infection control
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Healthcare-associated infections (HAIs) and sepsis mortality are major public health problems which are preventable.1–3 In the USA, federal programmes such as value-based payment programmes and public reporting have been implemented to increase accountability of hospitals to improve quality and safety outcomes such as HAI.4 However, these programmes are more likely to penalise major teaching hospitals and safety-net hospitals that treat a disproportionately large share of patients of low socioeconomic status.5 In the year 2012, a Medicaid 1115 transformation waiver that incentivised delivery system reform, called Delivery System Reform Incentive Payment (DSRIP), converted a significant portion of its Medicaid hospital payments to performance-based payments,6 which allowed hospitals to commit to transform quality of care by applying process improvement methodologies and reduce potentially preventable complications. We leveraged this opportunity to implement a 5-year hospital-wide initiative with the goal of reducing HAI and sepsis mortality.
The initiative focused on reducing the following primary outcomes: central line-associated bloodstream infection (CLABSI) in all wards and intensive care units (ICUs), catheter-associated urinary tract infection (CAUTI) in all adult wards and ICUs, surgical site infection (SSI) after 18 different types of surgical procedures, and mortality in patients who presented to the emergency department (ED) with sepsis on admission. The scale of this initiative was above and beyond federal and state requirements for infection prevention in the year 2013. The initiative was needed because prior efforts to reduce HAI were confined to CLABSI in ICUs and publicly reportable SSIs, and the interventions largely addressed select infections and pathogens, without a system-wide strategy or structures in place. Per the DSRIP programme requirements, the hospital system committed to implement a predefined set of broadly applicable, horizontal interventions (eg, awareness campaign) and infection-specific interventions (eg, bundles of care) and achieve at least 10% reduction in the primary outcomes during 2013–2017. The DSRIP fund at risk if the initiative was not implemented and the goals not met was $25 138 697.00, or 2.34% of the total supplemental payments for providing uncompensated care at the study institution during this time period. This article discusses the intervention strategy, results, lessons learnt and implications for public policy.
Methods
This prospective observational quality improvement study was conducted from 2013 to 2017 in a publicly funded 770-bed public academic hospital in the USA, Parkland Health and Hospital System, that provides a wide variety of medical and surgical services including oncology, dialysis, renal transplant, stroke, complex level I trauma care, acute burn care for the region, level III neonatal intensive care and high-risk maternal fetal care. The hospital has two medical ICUs, a surgical trauma ICU, a burn ICU and a neonatal ICU. In August 2015, the hospital moved to a new facility with a hundred additional beds and a neurocritical care unit. Patients receiving care are socioeconomically challenged, with over 73% being uninsured or underinsured. Patient volumes include more than 35 000 adult inpatient discharges, over 1000 discharges from the neonatal ICU and about 250 000 ED visits annually. The health and hospital system has over 11 000 employees, in addition to 2000 residents and fellows, and 250 medical and other students rotating per year. Physician services are largely provided by over 1600 faculty physicians employed by the medical school, with which the hospital is affiliated through a medical services contract. During the 5-year initiative from 2013 to 2017, in addition to the 2 years prior to the start of the initiative, the hospital was under regulatory oversight to improve quality of care, and several executive leadership changes occurred. There were four categories of patients included in the quality improvement initiative: hospital inpatients with central venous catheters (~45 000 central line days per year); adult hospital inpatients with urinary catheters (~27 000 urinary catheter-days per year); patients undergoing any of the following 18 types of surgery (~9000 per year): abdominal aortic aneurysm surgery, abdominal hysterectomy, breast surgery, carotid endarterectomy, caesarean section, cholecystectomy, colon surgery, craniotomy, elbow prosthesis, hernia repair, laminectomy, open reduction internal fixation, peripheral vascular bypass graft, shoulder prosthesis, spinal fusion or refusion, total hip replacement, total knee replacement and vaginal hysterectomy; and patients with sepsis present on admission who were admitted through the ED (~2500 per year).
Intervention
The intervention team consisted of over a dozen multidisciplinary, interprofessional teams including nursing, medical and operational, informatics and other leaders, with facilitation and oversight provided by the system-wide infection prevention committee. The change was implemented in multiple small steps throughout the institution and several steps occurred in parallel. The overall change strategy was innovation and system redesign using a combination of horizontal approaches, that is, processes that are foundational to improving all outcomes of interest in this initiative, and vertical approaches, that is, processes that are specific to a single outcome of interest. Using such a combination of approaches using technical (a solution that is concrete and visible; eg, implementing a dressing change kit) and adaptive (a solution intended to enable critical thinking and problem-solving; eg, conducting interviews using open-ended questions) solutions to improve care is well supported in published literature.7–9 The theoretical framework of improvement was engaging stakeholders, standardising curriculum, training and workflows to reduce variation in care and ‘raise the floor’ per the Agency for Healthcare Quality and Research, and continuous quality improvement using plan-do-study-act methodology and quality improvement tools such as process maps, run charts and defect analysis tools.10 Individual services were allowed latitude to implement evidence-based interventions specific to the patient population they served (eg, vascular surgery service implemented chlorhexidine-based preoperative skin preparation; colorectal service implemented a reduction bundle that included hair removal in the preoperative area, use of antimicrobial incision drape for all cases, and use of a separate closing set with change of gloves, gown and separate drape if visibly contaminated).
An overview of specific activities and timeline is shown in table 1, with details in subsequent paragraphs.
Key component activities of the hospital-wide initiative to reduce HAI and sepsis mortality
In year 1, for gap analysis and designing interventions in granular detail, performance improvement analysts developed process maps from staff interviews, patient tracers and input from infection prevention experts to assess gaps in clinical care and opportunities for improvement for central line and urinary catheter care (from time of evaluation for insertion to time of removal), surgical care (from scheduling surgery to 30 or 90 days from surgery when surveillance for SSI ends) and sepsis care (during the first 6 hours from arrival in ED). Specific interventions were prioritised for implementation and teams were formed to implement these interventions. The infection prevention and control committee provided governance for the entire project, with quarterly reports to the quality committee and the governing board.
In years 1 and 2, infection preventionists engaged clinicians and key stakeholders through online surveys open to all clinicians including trainees, biweekly lunch and learn sessions open to everyone (held in a ‘fair’ format), 1:1 interviews (mostly conducted by the primary author) and focus group meetings. The input gathered was rich and informative, and it was incorporated into gap analysis and intervention design. To give the initiative an identity, the infection prevention department held a naming contest and selected the name ‘Reducing Infections Together in Everyone’ (RITE programme), from over a hundred entries. In years 1, 2 and 3, beginning with a kick-off meeting with executive leaders, the department ran a communication and awareness campaign with screen savers on computers, monthly updates via a newsletter called ‘IP Beat’, rounding by infection preventionists in the wards and ICUs, recognition for those observed using best practices, (eg, stop the line) and dissemination of surveillance data throughout the hospital. The project managers represented the hospital in a regional collaborative of all healthcare systems participating in the state DSRIP programme to share and learn lessons and best practices from each other.
In addition to the above ‘horizontal’ interventions, most of which were ‘social’ and ‘adaptive’ as opposed to ‘technical’ interventions, about 550 managers and leaders (approximately 5% of workforce) including hospital unit-based nursing and operational leaders, charge nurses, senior nurses, as well as medical directors and physician chiefs of service were trained in key concepts of quality and safety through inperson training sessions that offered 3 credit hours. Fifty-eight (10.5%) of these leaders completed a 9-day training programme in clinical safety and effectiveness sponsored by the medical school. The specific disease-targeted prevention measures, that is, the ‘vertical interventions’, are described in the following sections.
Specific interventions to reduce CLABSI
A maintenance care bundle was developed and staff educated. Elements of the bundle included central line medically indicated; dressing dry, intact, dated and timed; Biopatch present; and intravenous tubing dated and timed. A standardised insertion kit with checklist was used. Nursing policies were updated to reflect evidence-based practice. An interprofessional standardised curriculum for insertion and maintenance was developed. Maintenance audits called ‘device rounds’ for both central lines and urinary catheters were implemented initially daily and then monthly. Unit-level results of device rounds were shared monthly in divisional quality improvement committees to promote awareness and generate healthy competition between units. An all-inclusive, standardised central line dressing change kit was developed, which served as a ‘visual checklist’ with items arranged in order of use during a dressing change procedure. In year 4, a change was made to the dressing kit with the replacement of the Biopatch with a chlorhexidine gel window occlusive dressing. This allowed for a visual assessment of the line insertion site. Dressing changes were completed within a 6-hour window after a chlorhexidine bath to capitalise on a 6-hour constant kill time. A disinfector cap was added to all intravenous ports for intensive care patients and on central lines only for non-intensive care patients. A ‘scrub the hub’ campaign initiative was launched promoting awareness of using proper technique when accessing ports.
Specific interventions to reduce CAUTI
A maintenance care bundle was developed and staff educated. Elements of bundle included urethral catheter medically indicated; catheter secured with StatLock device to reduce meatal irritation; positioned to promote drainage; and closed system maintained and a separate container used to empty urine bag. A nurse-driven discontinuation protocol was launched. Maintenance audits were implemented initially daily and progressed to a monthly frequency. The need to maintain a closed urine collection system was emphasised and opportunities for breaking the closed system were minimised. Patients’ bath basins were made single-use items to prevent cross contamination. Chlorhexidine-based wipes were used for perineal and incontinence care.
Specific interventions to reduce SSI
We addressed SSI prevention by optimising perioperative antimicrobial prophylaxis through implementation of standardised ‘smart’ order sets in our electronic medical record that allowed cascading of information. We implemented chlorhexidine bath the night before and the day of surgery for patients undergoing elective procedures. In year 3, we implemented interventions that included glucose control in patients with diabetes, smoking cessation prior to procedure and negative pressure wound therapy in select populations. A colorectal SSI reduction multidisciplinary workgroup was formed in year 4 which designed and implemented a reduction bundle that included hair removal in preoperative area, use of antimicrobial incision drape for all cases, and use of a separate closing set with change of gloves, gown and separate drape if visibly contaminated.
Specific interventions to reduce sepsis mortality
An electronic medical record-based sepsis early warning system that was developed by Parkland Center for Clinical Innovation was implemented in 2014 for early detection and standardisation of care. Clinical decision support tools were used to create best practice alerts to ED triage nurse to follow a standard delegated order with initial labs including lactate and blood cultures. Patients who had laboratory values and vital signs consistent with severe sepsis or septic shock had a separate best practice alert triggered for the physician that linked to an order set with all the components of the sepsis bundle,11 that is, blood cultures prior to broad spectrum antibiotics, intravenous fluids, serial lactate measurements as applicable and intravenous vasopressors in the presence of refractory hypotension. Choice of antimicrobial agents was standardised in consultation with infectious diseases and incorporated into the order set. To improve workflow for antibiotic administration, we engaged pharmacy services and moved the most used antibiotics to a local Pyxis. We engaged laboratory services to expedite the lactate turnaround time; when that was maximised, we implemented a conditional lactate order to ensure that a repeat lactate was automatically ordered if the initial lactate was >2.0 mmol/L. Finally, a sepsis worksheet was used so that the local nurse champion can ensure that all of the bundle components were met within the first 6 hours of sepsis presentation for each patient.
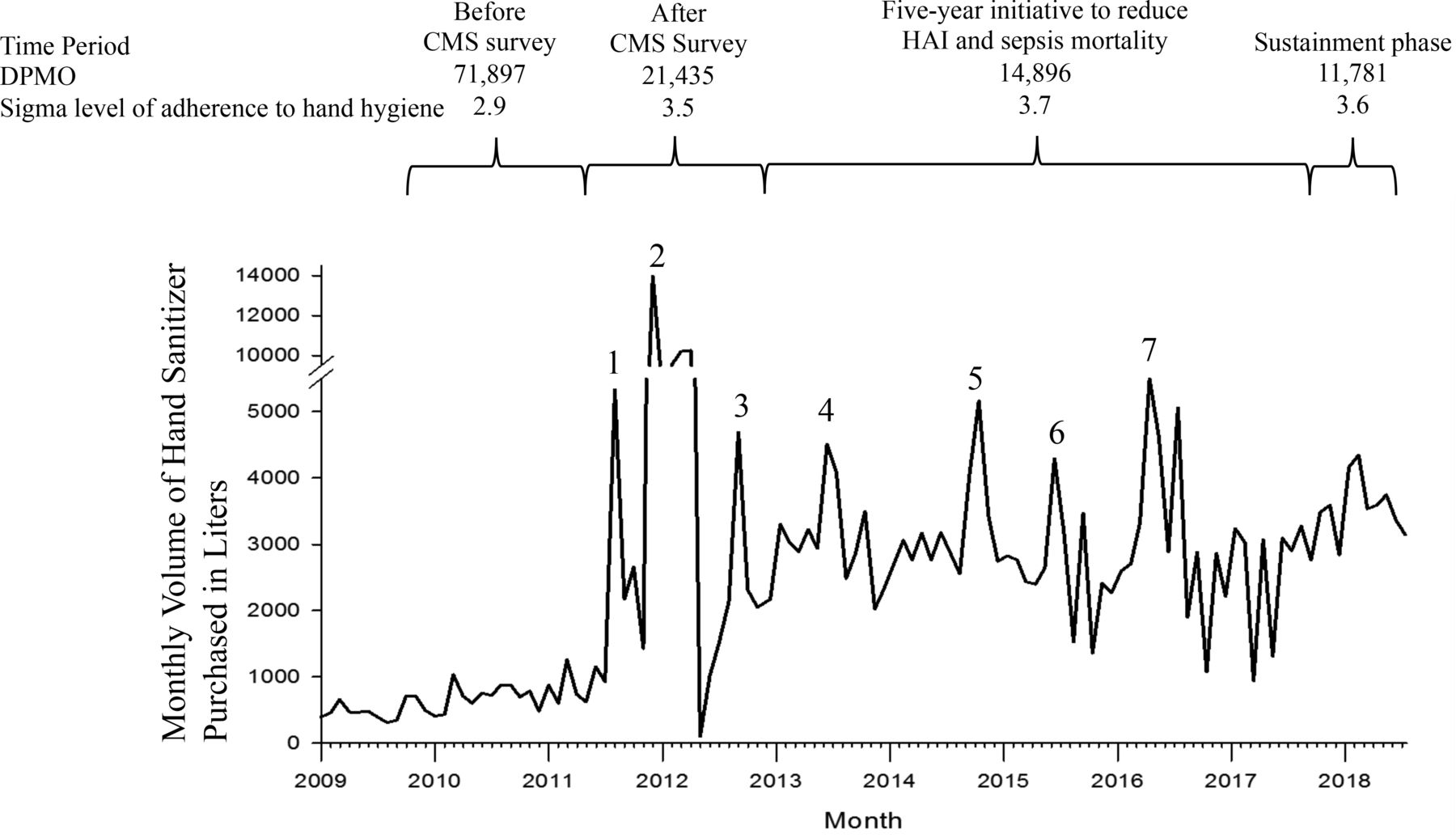
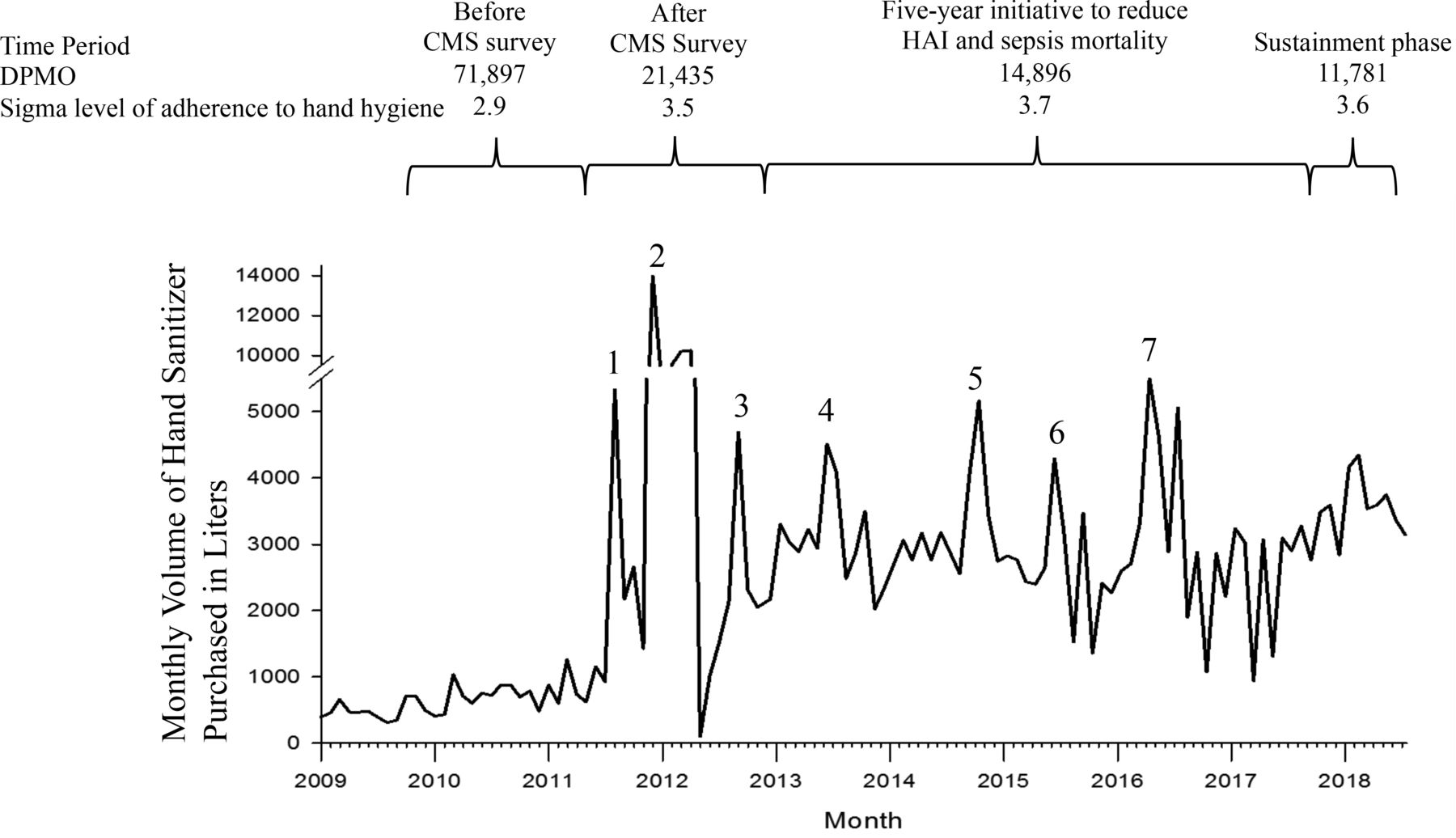
During the 5-year period of the initiative, leadership made quality and safety a priority for the institution. We addressed ‘initiative fatigue’ through frequent huddles and conversations. The proactive nature of the initiative, in contrast to reactive nature of responding to regulatory failures, and initial successes served as great motivators for teams. Hand hygiene continued to be a main focus and regulatory oversight continued. Adherence to hand hygiene was measured using direct observation method per the WHO12 by over 200 trained observers. Hand sanitiser availability was standardised throughout the health and hospital system. Culture of safety was measured every 1–2 years using the Agency for Healthcare Research and Quality methodology.13
Data collection
Clinical outcomes
CLABSI, CAUTI and SSI outcome data were collected retrospectively for 2013 and prospectively from 2014 to 2017 by trained infection preventionists through review of electronic medical records of all patients with positive blood cultures, positive urine cultures and those who underwent one of the 18 surgical procedures of interest, respectively. Surveillance definitions per the Centers for Disease Control and Prevention National Healthcare Safety Network14 were used. Mortality data were obtained by electronic abstraction of data, by determining death during hospitalisation within 28 days from the date of admission. Sepsis bundle adherence was measured according to recommended criteria.15
Process measures
Adherence to hand hygiene and bundled processes of care for central line and urinary catheter was obtained from the infection prevention department. Adherence to perioperative antimicrobial prophylaxis guidelines, sepsis bundle and sepsis mortality was measured via Clarity reports programmed in electronic medical records (Epic) and validated for accuracy. Although utilisation of hand sanitiser in the patient care areas could not be measured because it is cumbersome to do so, the volume of hand sanitiser purchased per month was obtained from purchasing records. Data on culture of safety were obtained from the patient safety department.
Data analyses
To determine the significance of trends in clinical outcomes and clinical processes, Poisson regression was used to model the number of events, that is, CLABSI, CAUTI, SSI and sepsis-associated deaths per year, while using the log of the respective denominators as ‘offset’ to scale the results appropriately. To determine the reliability of hand hygiene adherence data, defects per million opportunities and six sigma level of adherence were measured using an open access online calculator.16 To measure the significance of linear trend in culture of safety results over time, Cochran-Armitage trend test was used. All tests were two-tailed and the level of significance was set at α of 0.05. SAS 9.4 for Windows was used for analyses.
Results
In 2013, which was the baseline year, the rates of the four outcomes of interest, CAUTI, CLABSI, SSI and sepsis mortality, were 4.7 per 1000 catheter-days, 1.6 per 1000 catheter-days, 3.4% and 9.4%, respectively. To intentionally engage front-line clinicians, leaders and stakeholders in identifying gaps and potential solutions, 94 inperson, 1:1, 1-hour interviews, 20 lunch and learn sessions (average attendance of 60 per session) and an email survey to ~5000 clinicians (response rate of 4%) were conducted. They yielded important qualitative information on readiness and levels of commitment for change.
The results of interventions on primary outcomes are shown in figure 1. From 2013 to 2017, overall infection rates reduced by 73% for CAUTI (from 6.1 to 1.0 infections per 1000 catheter-days in the adult ICUs and rehabilitation unit; from 3.1 to 1.6 in the wards), 52% for CLABSI (from 1.5 to 0.9 infections per 1000 central line days in the ICUs; from 1.7 to 0.2 in the wards) and 62% for SSI, and unadjusted mortality rate reduced among patients with suspected sepsis by 69%. These improvements are statistically significant. In patients undergoing surgery, the unadjusted infection rates in 2013 and 2017 were, respectively, 2.3% and 1.5% for abdominal hysterectomy, 5.1% and 1.7% for breast surgery, 3.9% and 0% for carotid endarterectomy, 3.6% and 1.5% for caesarean section, 1.4% and 0.7% for cholecystectomy, 14.7% and 4.5% for colon surgery, 4.9% and 1.5% for craniotomy, 0% and 0% for elbow prosthesis, 3.3% and 1.0% for hernia repair, 2.5% and 0% for laminectomy, 2.1% and 0.3% for open reduction internal fixation, 21.2% and 0% for peripheral vascular bypass graft, 9% and 0% for shoulder prosthesis, 2.4% and 0.5% for spinal fusion or refusion, 4.7% and 1.9% for total hip replacement, 1.4% and 2.8% for total knee replacement, and 1.8% and 0% for vaginal hysterectomy. Two years after the initiative ended, in 2019, the rates of CAUTI, CLABSI and SSI for the same patient population were 1.2, 1.1 and 1.3, respectively, which were not significantly different from 2017. The measurement of sepsis mortality in the institution changed to newer Centers for Medicare and Medicaid Services (CMS) guidelines after 2017. The results of intervention on process measures are shown in table 2.
Performance on key hospital-wide process measures during the initiative to reduce HAI and sepsis mortality

Trends in outcomes of healthcare-associated infections and sepsis mortality during the initiative. The following are the Poisson regression estimates for trend in reduction for each outcome over the 5-year period, the 95% CIs and the p values: CAUTI: estimate −0.34 (−0.43 to −0.26), p<0.0001; CLABSI: estimate −0.19 (−0.29 to −0.09), p=0.0002; SSI: estimate −0.29 (−0.34 to −0.24), p<0.0001; sepsis mortality: estimate −0.42 (−0.49 to −0.36), p<0.0001. CAUTI, catheter-associated urinary tract infection; CLABSI, central line-associated bloodstream infection; SSI, surgical site infection.
Secular trends in hand hygiene and culture of safety were measured. Hand hygiene adherence improved over time, as measured by the number of defects or failures per million opportunities for hand hygiene and sigma level to assess how the process varied from a perfect sigma level of six (figure 2). In addition, the monthly volume of hand sanitiser purchased in the entire health and hospital system was measured. The average monthly volume increased from 703 L during 2009–2011 before the CMS survey, to 4705 L during 2011–2013 when aggressive efforts to improve hand hygiene were implemented. The monthly volume purchased reached a plateau of 2917 L during the 5 years of the RITE initiative and 3631 L in subsequent years (figure 2). Overall, culture of safety improved significantly in the health and hospital system from 2012 to 2019 (table 3).
Hospital-wide results of patient safety climate survey in healthcare personnel
{kind=link}
{kind=link}
Volume of alcohol hand sanitiser purchased per month and hand hygiene adherence in the health and hospital system during different time periods in the hospital system. DPMO is defects or failures per million opportunities. Sigma level is a measure of how much the process varies from perfection: a level of six is perfect. Numbers corresponding to each peak of volume purchased in the graph represent the following events: 1: CMS regulatory survey; 2: beginning of health and hospital system response to negative findings of regulatory survey; 3 and 4: anticipation of follow-up CMS survey; 5: occurrence of Ebola virus infection in the local community; 6: opening of new hospital facility; and 7: opening of new subspecialties clinic facility. CMS, Centers for Medicare and Medicaid Services; HAI, healthcare-associated infection.
During the initiative, the number of healthcare personnel offered training in bundles of care and the percentages who completed were 10 601 (91%) for basics, 3389 (90%) for central line, 3117 (91%) for urinary catheter, 895 (83%) for surgery and 1455 (85%) for sepsis care. In addition, 550 key leaders, managers and personnel completed training in quality improvement methods, including 58 (10.5%) who completed a 9-day training programme in clinical safety and effectiveness.
The direct cost of the 5-year initiative for programme management was $1.16 million in addition to the time spent by the project team members. In addition, the institutional direct cost incurred on hand sanitiser during this period was $540 664. The estimated impact of this initiative was prevention of 318 CAUTI, 119 CLABSI, 580 SSI and 526 lives saved among patients with suspected sepsis. The healthcare cost avoided because of HAI prevention is estimated to be over $17 million based on previously published data.17
Discussion
Through this initiative, we found that system-wide improvements in HAIs and sepsis mortality are possible in a large public academic safety-net medical centre using a change strategy that included a balanced combination of different types of interventions. Other organisations have reported similar improvements through system-wide initiatives18–20; however, these initiatives did not attempt to improve multiple clinical outcomes simultaneously, and their commitment was not associated with a significant financial downside risk if results were not achieved. Horizontal interventions provided a system-wide framework for preventing potential complications of care related to infections, the importance of which was emphasised in previous publications.7 8 21 Implementation of the initiative in the context of ongoing improvements in hand hygiene22–24 and culture of safety may also have contributed to success, as was the case in other institutions.25 Future direction of the initiative is further sustainment using the framework in published models.26
Because this was a pragmatic quality improvement initiative, the results achieved cannot be conclusively attributed to any or few particular interventions. Audits of process measures were time-consuming and were not conducted in all the years of the initiative. The device utilisation ratios did not improve, contrary to expectations. The number of urine cultures and blood cultures performed in the hospital increased significantly during the 5-year period, which could be a reflection of increased awareness to diagnose HAIs and sepsis. Previous publications reporting HAI reduction have discussed that bundles of care by themselves may not be sufficient for improvement.27–29 Discussion of trends in specific pathogens like multidrug-resistant organisms, or trends in individual wards, ICUs or surgical services, is beyond the scope of this paper. In 2015, the hospital moved to a newly constructed facility, and the specific impact of this move on study outcomes is not clear.
Several key lessons were learnt from this initiative. A formal requirement to implement this programme helped everyone to stay focused on improving care for patients. It is critical for healthcare epidemiologists, physicians and quality professionals to work with healthcare administrators and identify government programmes that afford opportunities to innovate and transform patient care. Engaging clinicians and stakeholders at the beginning of the initiative helped assess readiness for change and gather valuable insights. Providing infection prevention education and quality improvement skills to key leaders and managers in the health system without being too prescriptive encouraged innovation at the bedside (eg, design of a central line dressing change kit with items arranged in order of their use, ie, a visual checklist, during dressing change procedure). The momentum generated during the aggressive infection prevention response to negative findings of a regulatory survey that occurred 2 years prior to the start of this initiative was leveraged to implement a proactive approach to infection prevention.
The results of this initiative have important implications for public policy. Accountability programmes such as value-based purchasing, public reporting and regulatory requirements related to infection prevention and sepsis care do not require an institution to commit to goal achievement, even though several institutions have achieved improvements after these programmes were implemented. On the other hand, the DSRIP opportunity allowed the institution to take a ‘moonshot’ approach to improve infection prevention, by allowing the institution to commit to achieve deliverables and goal outcomes that were significant, achievable, local context-driven and associated with substantial payments at risk if they were not achieved. Goals were supported by local evidence and aligned with meaningful needs previously identified by the institution. Safety-net systems like the study institution have lower profitability than traditional for-profit or not-for-profit health systems30 and see very high demand for their services. In many health systems, modest penalties, for instance, for excess hospitals readmissions, may be offset with revenue from additional admissions. This was not the case at the study institution, where over 6% of unfunded care reimbursement was at risk in a system with limited ability to generate those funds from other payers. The programme payments were not new funds but critical supplemental funds previously paid for the care of low-income uninsured or Medicaid beneficiaries. Without new funding but rather to ensure maintenance of existing funds to serve a large population in need, the institution focused heavily on projects aimed to improve care for the existing population as opposed to other project options that encouraged expansion of services. The programme payments were weighted heavily towards implementation of processes in the first 3 years and towards achievement of outcomes towards the remaining 2 years, which was helpful. Similar DSRIP programmes successfully supported quality transformation work in several states including New York and California.31–34 Our interventions and results are generalisable to academic medical centres of similar size and complexity. It might be possible to replicate the results of this programme in other hospitals with modest financial investments and streamlining efforts of multiple leaders and stakeholders in the absence of DSRIP or a similar programme.
In conclusion, a combination of several types of interventions along with improvements in hand hygiene and culture of safety were effective in improving rates of HAI and sepsis mortality. The Delivery System Reform Incentive Payment programme provided a novel opportunity to transform healthcare delivery related to infection prevention and sepsis care in a large academic safety-net health and hospital system.
Acknowledgments
The authors acknowledge the contributions of Joselin Anandam, MD, John Michael Ashworth, Marianne Bartlett, Deanna Bokinsky, Jacqueline Brock, Deborah Brooks, Katherine Collinsworth, Deborah Couger, Roberto de la Cruz MD, Pamela Fox MD, Donna Gaffney, Janet Glowicz, Robert Hendler MD, Maurice King, Jennifer Masengill, Christina Mintner, Herron Mitchell, Brett Moran MD, Joanne Muturi, Jennifer Ochieng, Ellen O’Connell MD, George Oliver MD, Esmaeil Porsa MD, John Raish, Gary Reed MD, Donna Richardson, Monal Shah MD, Jeanne Sheffield MD, Suzanne Sims, Jacqueline Sullivan, Dena Taherzadeh, Sylvia Trevino and Karen Watts for their invaluable assistance with programme design, implementation or data collection.
References
Footnotes
Twitter @Pranavi_MD
Contributors Initial project design: PS, CM. Intervention design and implementation for CLABSI, CAUTI and sepsis mortality: CG, JH. SSI intervention design and implementation: JM. Sepsis mortality intervention design and implementation: CG, RR. Overall project implementation: PS, KV-H, CW. Data collection: KV-H, CW. Patient safety culture data: KG. Data analysis: PS, AM, RH. Manuscript first draft and coordination of authors: PS. Critical additions to the manuscript: KV-H, JH, RR, RH, FC. Data interpretation, critical manuscript review with final edits and approval: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The UT Southwestern Medical Center institutional review board deemed this study quality improvement and not research.
Provenance and peer review Not commissioned; externally peer reviewed.