Article Text

Abstract
Venous thromboembolism (VTE) is the fourth most commonly reported complication in trauma patients. For these patients, thromboprophylaxis is a standard of care. Patient compliance with sequential compression devices (SCDs), a form of mechanical VTE prophylaxis, has been a focus of efforts to improve patient safety. At our institution, a baseline audit in July 2020 revealed that patients admitted to the trauma floors have poor compliance with the use of SCDs. In this quality improvement project, we developed a patient education intervention to improve SCD compliance. We distributed an informational flyer to patients and led short educational sessions on VTE risk factors and proper SCD use. Our aim was to increase our SCD compliance rate by 30% in 4 weeks. We used three plan-do-study-act (PDSA) cycles to implement and refine our intervention. We measured SCD compliance during morning and afternoon patient observations and generated run charts to understand how our cycles were leading to change. After a 4-week period, we did not achieve our aim, but increased our overall compliance from 45% to 60% and sustained this improvement throughout our PDSA cycles. Morning compliance was lower than afternoon compliance both at baseline (45% vs 48.5%) and at the end the project (45% vs 53%). Our results suggest that patient education should be coupled with interventions that address other barriers to SCD compliance.
- patient education
- PDSA
- quality improvement
- venous thromboembolism
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Venous thromboembolism (VTE) is a potentially fatal adverse event in hospitalised patients. This is particularly true for patients suffering from trauma. In these patients, the physiologic hypercoagulable state following trauma coupled with emergent procedures and reduced ability to ambulate secondary to injuries increases risk for VTE. Mechanical VTE prophylaxis in the form of sequential compression device (SCD) is an important intervention for reducing VTE risk in this population.
For trauma patients at Kings County Hospital Center (KCHC), SCD application is a focus of efforts to improve patient safety because the device is important for thromboprophylaxis yet compliance rates in patients are poor. KCHC is an urban, teaching hospital in Brooklyn, New York, with an active level 1 trauma centre. A 1-week baseline audit of SCD compliance among patients admitted to the trauma floors in July 2020 revealed a median compliance rate of 45%. The reasons for non-compliance were: (1) patients found the SCD sleeves uncomfortable (62%); (2) patients took SCD sleeves off at night before sleeping (15%); (3) SCD sleeves were not replaced after patients returned to bed (13%) and (4) SCD machines were not turned on (6%) (table 1).
Baseline audit: reasons for SCD non-compliance
The findings from this audit were discussed with the director of the trauma service, physicians and nursing staff, who all confirmed that SCD compliance was an ongoing issue. Nurses highlighted patient discomfort with wearing SCDs as a prominent reason for non-compliance. At the time of the audit, no standard protocol or compliance strategy existed at our institution for encouraging the use of SCDs. When rounding, physicians and medical students occasionally reminded patients to wear their SCD sleeves. Additionally, some nurses, physical therapists and other clinical staff reapplied SCD sleeves when they observed patients not wearing them. However, these were not universal practices.
The audit findings and team discussions motivated an improvement project to address poor SCD compliance. The specific, measurable, applicable, realistic and timely aim of this quality improvement (QI) project was to increase the SCD compliance rate in patients admitted to the trauma floors from 45% to 75% in 4 weeks.
Background
VTE, which includes deep venous thrombosis (DVT) and pulmonary embolism, is the leading cause of preventable hospital death in the USA, causing nearly 100 000 deaths annually.1 In trauma patients, DVT is the fourth most commonly reported complication, with an incidence of 5%–63%.2 In these patients, a systemic inflammatory response causes a hypercoagulable state that increases risk for thrombotic events.3–6 Emergency surgeries and invasive procedures further increase VTE risk in this population.7
Because management of VTE is expensive and associated with significant sequelae,8 the use of VTE prophylaxis is a standard of care.9 10 Although no consensus exists concerning the optimal method of VTE prophylaxis in trauma patients, the American College of Chest Physicians and the Eastern Association for the Surgery of Trauma recommend the use of chemical (eg, low molecular weight heparin) and/or mechanical thromboprophylaxis.11 12
SCDs are a form of mechanical thromboprophylaxis with inflatable sleeves that are connected to a machine. The sleeves intermittently compress the extremities, improving extremity blood flow and potentially decreasing the risk of DVT.13 Ibrahim et al reported a higher incidence of DVTs among adult trauma patients who did not receive VTE prophylaxis, compared with those who used SCDs.14 SCDs may be of particular importance to critically injured trauma patients for whom chemical prophylaxis is contraindicated. A study of 411 trauma patients found that 7% of injured patients who could not receive chemical prophylaxis developed VTE.15
Compliance with SCD use is a problem in the care of trauma patients.16–20 Reports have suggested that compliance is lower in non-intensive care unit (ICU) patients when compared with those in an ICU, possibly because hospital staff subjectively perceive non-ICU trauma patients as having a negligible risk of developing VTE.16 One quality assurance study followed 1356 patients admitted to the orthopaedic unit of a level 1 trauma centre and found an SCD compliance rate of 32%.21 The investigators reported that compliance was higher on weekdays than weekends and on morning observations when compared with afternoon observations.21
Limited patient education on VTE and mechanical thromboprophylaxis has been cited as a barrier to SCD compliance. Beachler et al placed an SCD educational flyer in the rooms of non-ICU orthopaedic patients and held nursing training sessions on the importance of SCDs for the surgical patient.22 The authors reported a significant increase in SCD compliance rate in these patients following a 2-week period (from 28% to 59%, p<0.0001).22 Similarly, Bohnenkamp et al found improved SCD compliance following patient education initiatives.23 No group has investigated patient education for trauma patients.
Design
Our baseline audit revealed that non-compliance was largely driven by patient factors. Patients found SCD sleeves uncomfortable (45%) and patients removed sleeves before bedtime (15%) (table 1). In this background, patient education initiatives proved successful at other institutions.22 23 For this reason, we developed an intervention focusing on patient education to improve SCD use in trauma patients at our hospital.
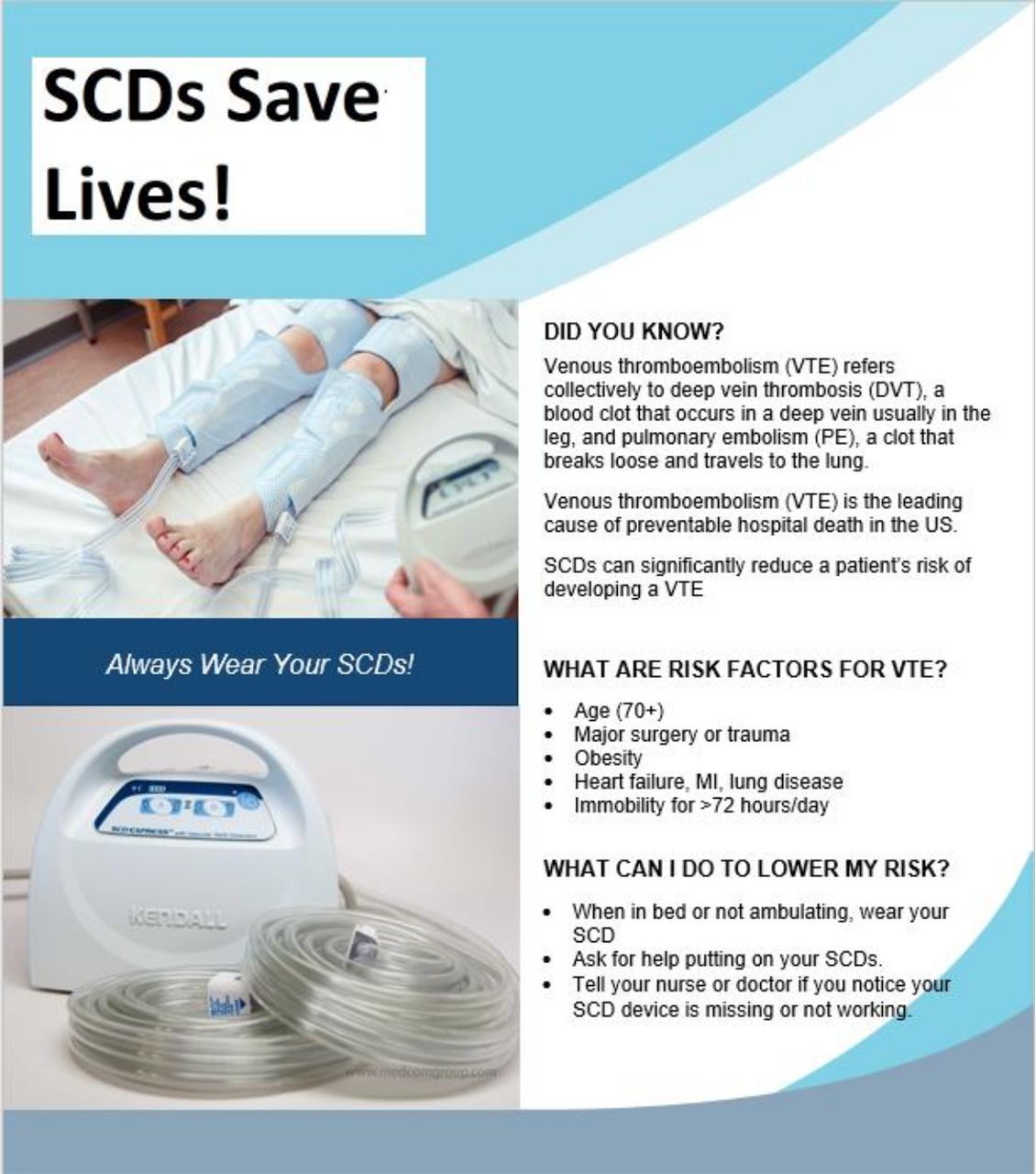
We designed an educational flyer (figure 1) aiming to educate patients on VTE and mechanical thromboprophylaxis. The flyer contains an image of SCD sleeves placed around the lower extremities and another image of an SCD machine. The three sections of text outline the definition of VTE, the risk factors for VTE and tips for properly using SCDs. The flyer was printed in English, Spanish and Haitian Creole.
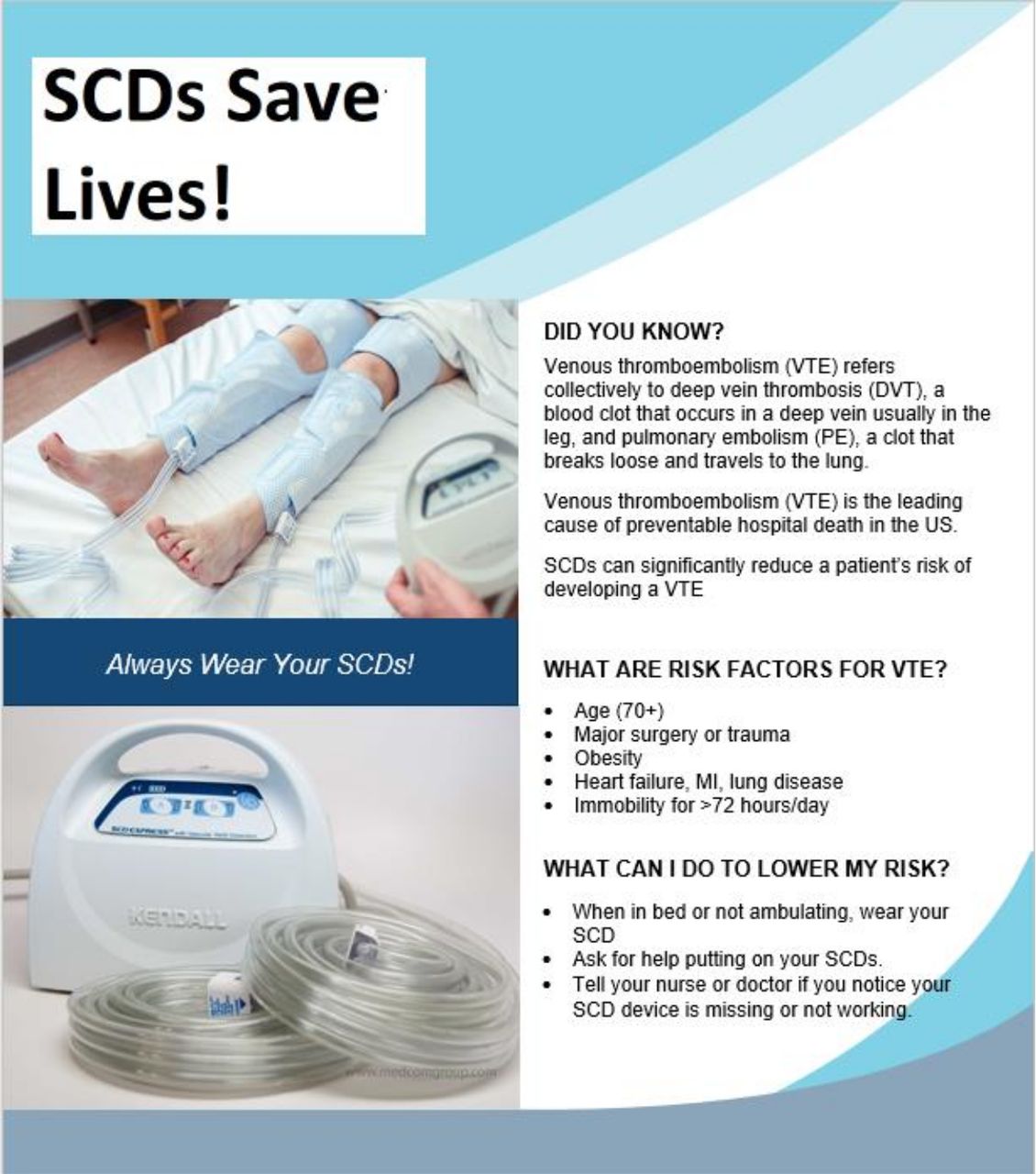
Patient education flyer on VTE risk factors and proper sequential compression device (SCD) use. Flyer was distributed to each patient as part of our patient education intervention. Flyer was available in English, Spanish, and Haitian Creole. MI, myocardial infarcation.
At the first encounter with each patient, a medical student distributed the flyer and spent 5–10 min going over its contents with the patient. In this short educational session, the student emphasised that SCD sleeves should be worn anytime the patient is in bed, including at night, and that the sleeves should fit firmly around the extremities. The student encouraged the patient to ask for help reapplying the sleeves after getting out of bed. At the end, the patient was asked to briefly summarise how to properly wear SCDs. The flyer was kept in the patient’s room at bedside. At subsequent encounters, the medical student provided brief reminders that SCDs should be worn to help prevent VTE.
Measurement
When a patient is admitted to the trauma floor at KCHC, the resident physician places an order for an SCD. The floor nurse then locates an SCD machine, places it on the foot of the bed and connects it to SCD sleeves. At our institution, a standard protocol does not exist for measuring how frequently a patient wears the SCD sleeves. At the beginning of their shift, some nurses comment in their nursing notes whether patients are wearing SCD sleeves (eg, ‘patient lying in bed with SCDs in place.’). However, this is not a universal practice and there is no official protocol for tracking SCD usage in the electronic medical record (EMR).
We measured compliance rates during morning (6:00) and afternoon (18:00) patient observations. We counted the number of compliant patients and divided by the total number of patients on the trauma floors with SCD orders. SCD use was considered compliant if the sleeves were applied firmly around the lower extremities and the SCD machine was turned on and working while the patient was in bed. SCD use was also considered compliant if the patient was standing, ambulating, sitting in bed or in a chair or transferring in or out of bed. This method of measuring and defining SCD compliance was used in previous QI work.24 25
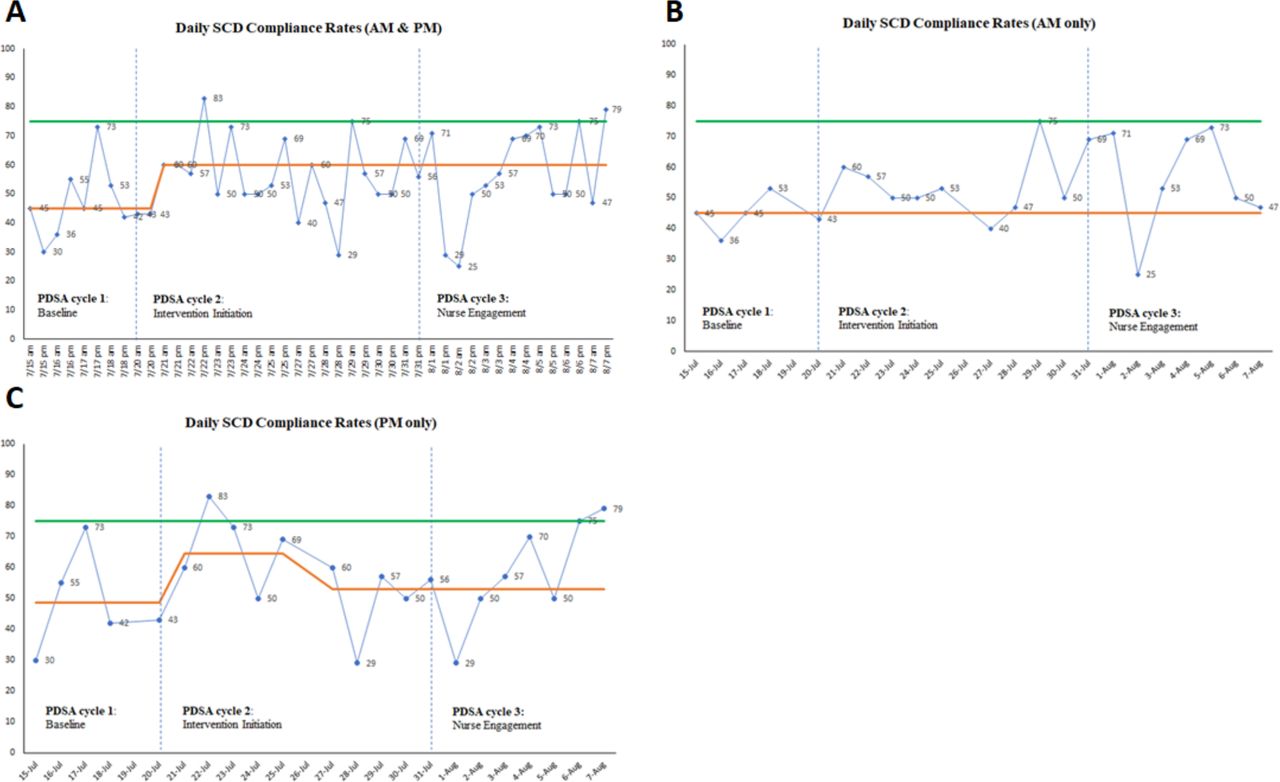
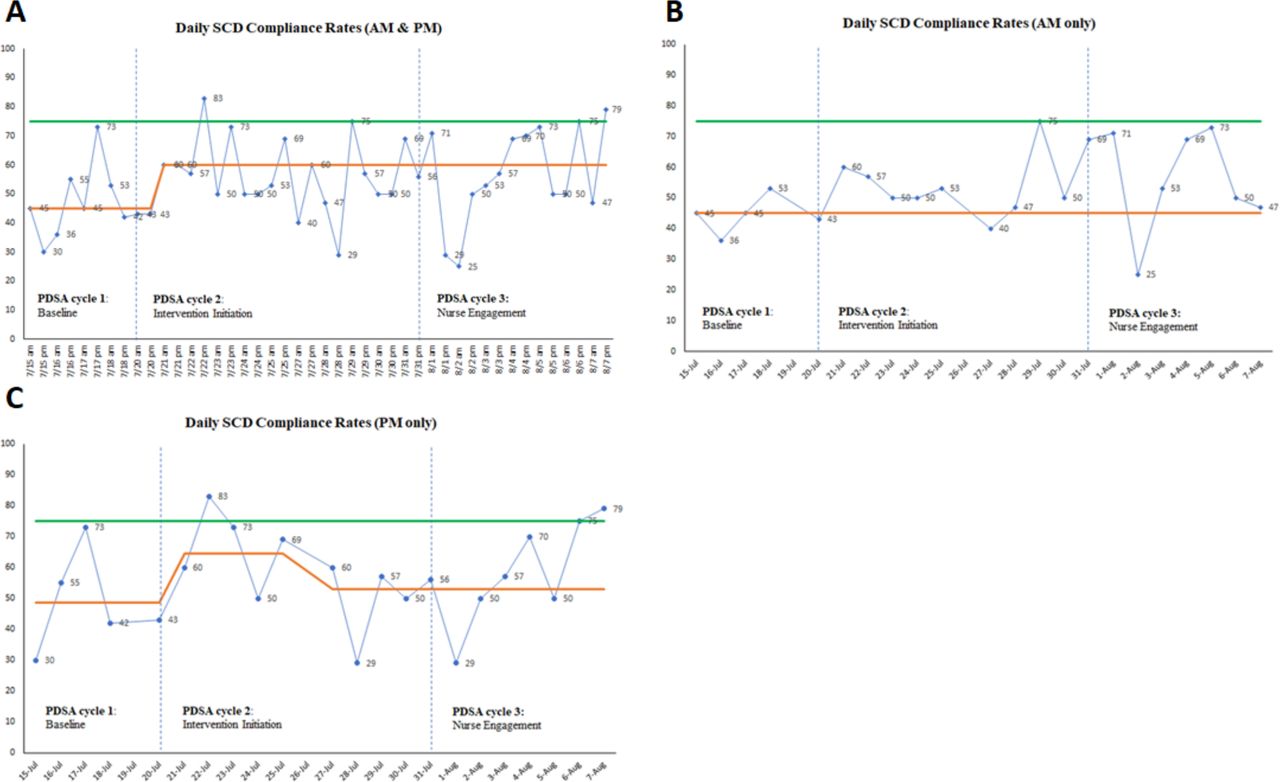
During our 1-week baseline audit, we plotted daily morning and afternoon compliance rates on a run chart and determined the overall median compliance rate to be 45% (figure 2A). The median morning rate was 45% (figure 2B) and the median afternoon rate was 48.5% (figure 2C). In this period, there were 163 patient observations. We continued to measure and chart compliance rates two times per day throughout the project and used them to assess how effectively our plan-do-study-act (PDSA) cycles were leading to change.
{kind=link}
{kind=link}
Run chart of SCD compliance rates. The green lines represent goal compliance rate (75%) and the orange lines represent the median compliance rate. (A) Run chart of morning and afternoon SCD compliance rates. Beginning at 7/21, a shift occurred in the dataset, increasing the median from 45% to 60%. No further shifts were observed. (B) Run chart of morning SCD compliance rates. No shifts were observed in the dataset. (C) Run chart of afternoon SCD compliance rates. At 7/21, a shift occurred in the dataset, increasing the median from 48.5% to 64.5%. At 7/27, a second shift occurred, decreasing the median from 64.5% to 53%. No further shifts were observed. PDSA, plan-do-study-act; SCD, sequential compression device.
Strategy
This QI project was led by the medical students rotating on the KCHC trauma service. We used a series of PDSA cycles to implement and refine our patient education intervention.
PDSA cycle 1: days 1–5
In this initial PDSA cycle, we determined timepoints for morning and afternoon patient observations that were compatible with the clinical responsibilities and schedule of a medical student. We also refined our definition of SCD compliance and addressed how patients with COVID-19 would be considered in our analysis. At the same time, we continued to collect baseline data on SCD compliance.
In our initial design, observations were scheduled for 6:00, before morning chief rounds, and again at 18:00, before afternoon chief rounds. About 3 days into this cycle, we recognised that morning observations were more feasible for students at 9:00, immediately following a daily departmental meeting. Meanwhile, afternoon observations consistently occurred at 19:00. We therefore redefined our timepoints for daily patient observations to be 9:00 and 19:00.
During this cycle, we encountered two floor patients whose COVID-19 statuses were unknown and one patient who was COVID-19 positive. To minimise exposure with these patients, we decided to exclude patients with unknown or positive COVID-19 statuses from our compliance analysis and educational intervention. Patients with unknown or positive statuses who later tested negative were included in subsequent observation periods.
We also encountered a patient with a left lower extremity external fixation device who was initially wearing an SCD sleeve on her right extremity, but on her second day of hospitalisation, had the right extremity splinted. If patients had a fixture on an extremity (eg, external fixation, splint, wound vacuum-assisted closure device(VAC), dressing, etc) that precluded wearing an SCD sleeve, we only considered the other extremity when documenting compliance. If patients could not wear sleeves on either extremity despite having an SCD order, we excluded them from our analysis. They were included in subsequent observation periods if they had the fixture removed.
We did not begin our education intervention in this cycle. Rather, we continued our prior practices for encouraging SCD use, which included informal reminders to patients to wear SCD sleeves. At the end of PDSA cycle 1, there were a total of 163 patient observations and the overall median SCD compliance rate was 45% (figure 2A). The median morning rate was 45% and the median afternoon rate was 48.5% (figure 2B,C).
PDSA cycle 2: day 5–week 2
In PDSA cycle 2, we initiated our intervention. On the first day of the cycle, students distributed the educational flyer to each patient on the trauma floors and led short educational sessions with the patients. On subsequent days, this process was repeated only for new floor admissions. For patients who had already received the flyer and educational session, we checked to see that the flyer was still at bedside and spent 1–2 min reminding patients to wear SCD sleeves whenever in bed.
In this cycle, two patients discarded their flyers and were given new ones to keep at bedside. One patient whose primary language was Spanish was given an appropriately translated flyer. Her daughter, who was present at bedside during the educational session, served as a translator.
In our original design, initial educational sessions were scheduled to last 5–10 min. While this represented our experience with most patients, a few patients struggled to summarise key points at the end of their sessions, so we spent extra time educating them until they were able to provide an adequate summary. For these patients, educational sessions lasted for about 15 min.
Towards the end of this cycle, new medical students arrived on the trauma service. They were briefed on the project’s goals and agreed to continue data collection and intervention implementation. There were 4 days of overlap between the old and new medical students, ensuring adequate training. At the end of PDSA cycle 2, there were a total of 182 patient observations and the overall median compliance rate increased to 60% (figure 2A). The median morning compliance rate remained at 45% and the median afternoon compliance rate increased to 64.5% (figure 2B,C).
PDSA cycle 3: weeks 3–4
In PDSA cycle 3, we encountered a patient with traumatic brain injury who was unable to speak. This precluded his active participation in our intervention. To ensure SCD compliance, we recruited his nurses to help monitor that SCD sleeves were always applied firmly around his legs and that the SCD machine was always turned on.
After a team discussion, we decided it would be productive to engage all patients’ nurses. After an encounter with a patient, we located the nurse and explained our project goals. We showed the nurse our educational flyer and requested help in ensuring SCD sleeves were always on and reapplied after the patient returned to bed and that the machine was turned on. We informed nurses that our intervention was already leading to improvements in compliance. All nurses were receptive to our project goals and agreed to participate.
In this cycle, we attempted to expand our intervention to include patients on the general surgery service. However, the fragmented schedules of the general surgery medical students did not allow for the continuity necessary to carry out our intervention. At the end of PDSA cycle 3, there were a total of 126 patient observations and the overall median compliance rate remained at 60% (figure 2A). The median morning compliance rate was 45% and the median afternoon compliance rate was 53% (figure 2B,C).
Results
In total, there were 471 patient observations. Characteristics of the patient population assessed during the project period are shown in table 2.
Patient characteristics
After three improvement cycles, our overall median SCD compliance rate shifted from 45% to 60% (figure 2A). This shift occurred early in PDSA cycle 2 and was sustained throughout cycles 2 and 3 (figure 2A). No further shifts were observed. Despite this improvement, we did not meet our aim of increasing the SCD compliance rate from 45% to 75%.
At baseline, the median afternoon compliance rate (48.5%) was greater than the median morning rate (45%). The morning compliance rate did not shift from baseline throughout the three improvement cycles (figure 2B). In PDSA cycle 2, the afternoon rate increased to 64.5% but later decreased to 53% (figure 2C). At the end the project, the afternoon compliance rate (53%) remained greater than the morning rate (45%) and the difference was larger (8% vs 3.5%) than what existed at baseline.
Additionally, we were successful in developing a system of measuring compliance at our institution. Whereas before no protocol existed for documenting SCD compliance, in this project, we were able to measure compliance rates two times per day for nearly 4 weeks. We missed two Sundays of data collection when there were no medical students on the service.
Lessons and limitations
Our project is not without limitations. Studies report that SCD sleeves should be worn for 18–21 hours a day for optimal benefit,26 a length of time that our twice daily observations do not measure. Although morning and afternoon observation of SCD use is frequently used as a measure of SCD compliance, other methods have been employed. Murakami et al,27 for example, attached digital timers to SCD devices and recorded the length of time that patients wore SCD sleeves throughout the day and Cornwell et al performed six observations daily (two in the morning, two in the afternoon and two in the evening) to measure compliance.28 Another group relied on nurse charting of SCD use in their EMR to monitor compliance.29 Adopting some of these methods at our institution would be challenging. In our EMR, for example, nurses cannot input data regarding SCD use and at KCHC, we do not currently have the infrastructure to collect and store data from timers. Still, strengthening our ability to understand true SCD use on our trauma floors will involve developing better ways at measuring compliance.
Another limitation of our project was the late involvement of nursing staff. Up until our third PDSA cycle, we implemented our intervention largely without nursing support. Although we identified patient factors (eg, patients finding the sleeves uncomfortable, patients taking sleeves off at night, etc) as the primary causes of non-compliance, these are inextricably influenced by hospital factors such as nursing behaviour. Our finding that afternoon compliance was consistently higher than morning compliance suggests that the presence of nurses and daytime ancillary hospital staff is important for reinforcing SCD use. Indeed, similar QI work that involved nursing staff and administration reported improved outcomes. Beachler et al demonstrated increased SCD compliance on surgical floors after nurses were trained and educated on VTE risk and proper SCD application.22 Moreover, nurses and other clinical staff are important architects of a hospital’s culture of safety30 and if they are excluded from improvement interventions, we risk the development of normalised deviance, learnt helplessness and other behaviours that pose latent threats to optimising SCD compliance.
Part of the rationale for developing our intervention was that if we highlighted the clinical consequences of not wearing SCD sleeves through direct patient education, then patients would be motivated to practice better SCD habits. This reasoning assumed that our patients were in the contemplation stage of Prochaska’s transtheoretical model of behaviour change.31 At this stage, patients are receptive to facts and weigh the pros and cons of behaviour change. Perhaps, then, the increased compliance we observed during our project was due to a cohort of contemplation-stage patients who were incentivised by our educational intervention to wear SCDs despite their perceptions of SCD sleeves being uncomfortable and bothersome. Likewise, this would imply that we were unable to further increase our compliance rate because other patients were not in the contemplation stage and were not benefiting from our intervention. This motivates exploration for additional barriers to SCD compliance at our institution.
During project implementation, we noted that medical students had varying levels of confidence when interacting with patients and hospital staff. This was particularly true of new third year medical students beginning clerkships. To mitigate any effect this might have on the project, we ensured that there was appropriate training for new medical students and adequate overlap between the fourth year and third year medical students on the service.
Conclusions
Our description and assessment of a patient education intervention adds to a growing body of literature examining ways to improve SCD use in hospitalised patients. Previously, our institution lacked a compliance strategy for encouraging SCD use and a structured protocol for measuring SCD compliance. In this improvement project, we developed a basic system of monitoring compliance that was led completely by medical students. We also designed an intervention for promoting SCD use in trauma patients that focused on patient education. To our knowledge, this is the first report of a patient education initiative being used to address SCD non-compliance in trauma patients. This simple intervention led to an improvement in compliance rates that proved to be sustainable. Such an intervention can be adapted by other inpatient units looking to optimise SCD use in vulnerable patient populations. Finally, our project results suggest that SCD non-compliance is a complicated problem that requires identifying and appropriately addressing both active and latent barriers to SCD use.
References
Footnotes
Twitter @HamidSafraz, @BGalloMarin, @dr_badami
Contributors SH, AB and AG conceptualised the intervention; SH led the improvement cycles; SH, LS, KA-K, TW and CG performed data collection; SH, BGM and LS performed data analysis and interpretation; SH and BGM wrote original draft; SH, BGM, LS, TW, CG, AB, AG and VR reviewed and edited draft and VR administered the project.
Funding BGM was supported by NIH/NIAID R25AI140490.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.