Article Text

Statistics from Altmetric.com
Introduction
A notable proportion of cases of COVID-19 have occurred among older adults living in congregant settings.1 2 Once an outbreak occurs in such settings, few mitigation strategies exist. Identifying predictors of COVID-19 would facilitate enhanced surveillance to prevent future outbreaks. The Centers for Medicare and Medicaid Services have long required that all skilled nursing facilities (SNFs) report quality metrics, including the Five-Star Quality Rating System for comparing SNFs: 1 star (lowest score) to 5 star (highest score).3 This metric is predicated on patient and stakeholder perceptions. We examined the relationship of star ratings and other facility-related metrics to COVID-19 occurrence among nursing home residents using a newly established reporting mechanism by the state of California.
Methods
Beginning 17 April 2020, the California Department of Public Health (CDPH) started reporting the daily and cumulative numbers of positive cases of COVID-19 among the residents and staff of SNFs.4 For this study, we used the category ‘Cumulative Positive Residents’, and compiled data available through 31 May 2020.
SNF characteristics were obtained from the Facilities Compare Website3 as follows: Overall Star Rating, its three domains—Health Inspections, Staffing and Quality Measures, plus Provider and Ownership Types, Number of Certified Beds and Medicare Claims Quality Measures, and linked using the Federal Provider Number. Descriptive statistics were used for SNF characteristics with and without COVID-19 among the residents, and univariate-adjusted and multivariable-adjusted logistic regression models explored an association between the SNF characteristics with COVID-19 presence in SNF, while handling multicollinearity. The proportion of infected residents was calculated as the ratio of the maximum cumulative number of cases reported to the number of certified beds and visualised as bar plots for all levels of Five-Star ratings—SNFs with ‘<11’ infected residents were treated as having one infected resident per CDPH reporting requirements.4
Results
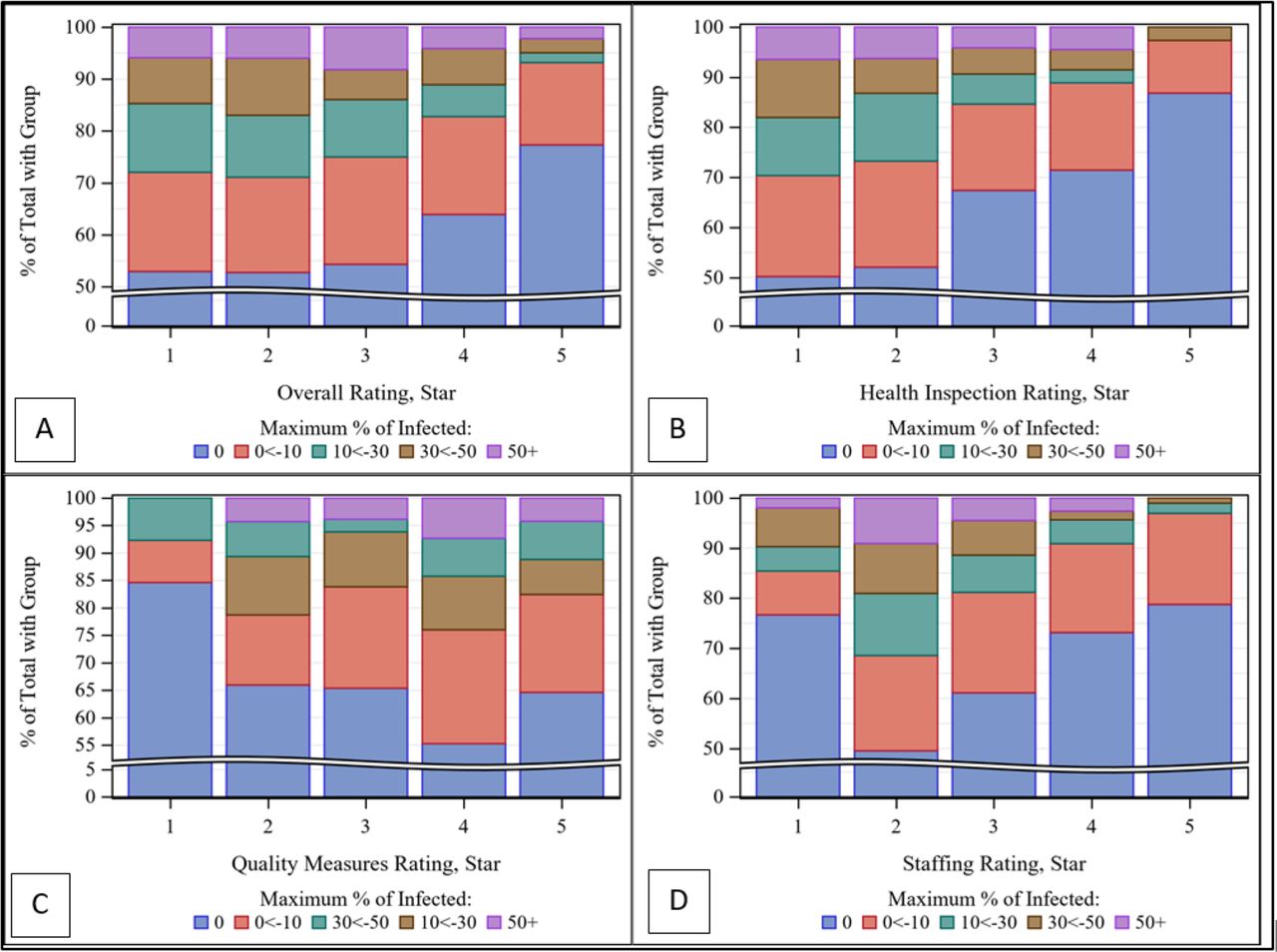
A total of 1184 of 1224 facilities that reported data are included in analyses. The cumulative number of residents with COVID-19 is 9650.4 Approximately 24% of facilities reported COVID-19 as of 31 May 2020. Figure 1 displays the proportions of facilities with residents with COVID-19 by star ratings. There appears to be an inverse relationship with COVID-19 with the Health Inspection and Overall Star ratings. Univariate regression shows that Health Inspection ratings and Overall ratings are significantly associated with facilities reporting COVID-19, and with multivariable adjustment, health inspections, emergency room visits and short-stay hospitalisations remain significant. Particularly, Health Inspection (among the three domains of the Overall rating) showed a consistent monotonic relationship between the star value and the presence of COVID-19, OR 2.6–6.5 (table 1 and online supplemental table S1).
Supplemental material

{kind=link}
Star ratings (overall and its three domains) and percentage of having COVID-19 case among residents. (A) Overall Star Rating*; (B) Health Inspection star rating**; (C) Quality Measures star rating*** and (D) Staffing star rating****. Within each panel, the percentage of total COVID-19 cases by numeric value of the star rating, 1 (minimum) to 5 (maximum). *Overall Five-Star Rating includes components of the three domains of star ratings. **The Health Inspection rating contains the three most recent health inspections and investigations due to complaints, with the most recent survey findings are weighted more than the prior year. ***The Staffing rating has information about the number of hours of care provided on average to each resident each day by nursing staff, and considers differences in the levels of residents' care need in nursing home. ****The Quality Measures rating has information on 15 different physical and clinical measures for nursing home residents to assess care delivery for their residents’ physical and clinical needs (see https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/CertificationandComplianc/downloads/usersguide.pdf for more details).
Univariate and multivariable logistic regression models of facility characteristics with no reported cases or at least one reported COVID-19 case among residents as the outcome
Discussion
Publicly reported SNF metrics are associated with COVID-19 presence in facilities. While not directly compared with each other, the findings suggest that facility star ratings directly driven by recent patient and stakeholder complaints are more potent predictors of COVID-19 than staffing or quality ratings. Hospital and emergency utilisation are also predictive but less directly patient focused than the star ratings. While the relationship with the Quality Measures star ratings, a subset of the Overall Quality Ratings with COVID-19 seems counterintuitive, it may be the result of hospital practice driving referrals of residents with high comorbidities to facilities with presumably high-quality ratings (≥3 stars) and away from facilities with low-quality ratings.5
As local governments attempt to mitigate multiple future outbreaks of COVID-19, these readily available metrics may help public health officials triage resources to select facilities, including the use of patient-focused surveys. Preventing outbreaks in congregate groups with heightened morbidity has obvious benefit.6 Yet, the gain may extend beyond as a substantial proportion of its residents have high contact rates with other healthcare venues. For example, nearly 32% of maintenance dialysis patients use SNFs during a calendar year.7
We acknowledge the data are limited to a single state in the early stage of the COVID-19 pandemic. Yet, California has a large population and sample size with standardised reporting and high participation by facilities4 (near 95%) compared with other states. As national governments begin reporting national data on COVID-19 morbidity in SNF, an opportunity to better align prediction with COVID-19 outcomes may soon arise.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AVK, EP and HB conceptualised the study. EP acquired the data. EP and HB analysed the data. AVK and EP drafted the manuscript. HB, AAT and PSR made critical changes to the original and revised manuscript.
Funding HB was partly supported by the National Institutes of Health through grant UL1 TR001860.
Disclaimer The opinions expressed in the paper are solely of the authors and do not represent the views of their affiliations.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.