Article Text

Abstract
COVID-19 is an established threat whose clinical features and epidemiology continues to evolve. In an effort to contain the disease, the National Health Service has adopted a digital first approach in UK general practice resulting in a significant shift away from face-to-face consultations. Consequently, more consultations are being completed without obtaining objective recording of vital signs and face-to-face examination. Some regions have formed hot hubs to facilitate the review of suspected COVID-19 cases and keep their practice site ‘clean’ including the use of doorstep observations in avoiding the risk of face-to-face examination. To support the safe, effective and efficient remote assessment of suspected and confirmed patients with COVID-19, we established a doorstep assessment service to compliment telephone and video consultations. This allows physiological parameters such as temperature, pulse, blood pressure and oxygen saturation to be obtained to guide further triage. Quality improvement methods were used to integrate and optimise the doorstep assessment and measure the improvements made. The introduction of a doorstep assessment service increased the proportion of assessments for patients with suspected COVID-19 in routine care over weeks. At the same time we were able to dramatically reduce face-to-face assessment over a 6-week period by optimising through a range of measures including the introduction of a digital stethoscope. The majority of patients were managed by their own general practitioner following assessment supporting continuity of care. There were no adverse events during the period of observation; no staff absences related to COVID-19. Quality improvement methods have facilitated the successful integration of doorstep assessments into clinical care.
- infection control
- PDSA
- general practice
- quality improvement
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The COVID-19 is an established healthcare threat whose epidemiology continues to evolve.1 In an effort to contain the disease, the National Health Service (NHS) has adopted a digital first approach in UK general practice resulting in a significant shift away from traditional face-to-face consultations.2 In response to the pandemic, general practitioners (GPs) have moved to a total triage model following NHS England guidelines.2 Using online, telephone and video consultations to reduce avoidable footfall in practice and protect patients and staff from infection.3 Consequently, more consultations are being completed without obtaining objective recording of vital signs and face-to-face examination.4 Some regions have formed hot hubs to facilitate the review of suspected COVID-19 cases and keep their practice site ‘clean’ including the use of doorstep observations in avoiding the risk of traditional face-to-face examination.5
Prior to 20 April 2020, there were 152 confirmed cases of COVID-19 for 34 practices in St. Helens covering a population of ~192 000. A retrospective case audit of 4831 patients in a single surgery in the same population prior to 22 April 2020 identified 21 patients with suspected COVID-19 (0.4% of population). While all of these patients had a remote assessment, only two had a physical assessment (10%), and both of these were done in an urgent care setting; none (0%) were done in routine care. Two of the patients with suspected COVID-19 went to hospital without prior examination in primary care (10%). There was one death with COVID-19 on the certificate in one of the hospitalised patients. A GP provider group of 26 practices in the St. Helens area covering a total population of 140 957 patients setup a local hot hub following discussions about local service needs in response to the COVID-19 pandemic. The hub was staffed by participant practice GPs and advanced nurse practitioners who have volunteered and meet ‘lower infection risk’ assessment. The aim of the service was to allow community assessment of those patients with suspected COVID-19 infection who are not able to attend the hot clinic while minimising exposure to primary care workforce and community spread. The service was commenced on 22 April 2020 and planned to run until 30 June 2020 with the doorstep assessment introduced on 27 April 2020; this was in anticipation of the peak of COVID-19 in early May, ~2 weeks behind that in London. A retrospective case review of patients reviewed at the hot hub in the week prior to the introduction of the doorstep assessment service indicated that all patients (4) were receiving traditional face-to-face assessment in full personal protective equipment (PPE).
The SMART objectives assessed in this study include: (1) increase the proportion of assessments of vital signs for patients with suspected COVID-19 in routine care by 10% in 2 months (baseline 0%) and (2) increase the proportion of non-face-to-face assessments for patients with suspected COVID-19 at the hot hub by 10% in 2 months (baseline 0%). Other outcomes to be reported includes: (3) number of doorstep assessments in patients with suspected COVID-19; (4) absences from work due to COVID-19 among clinicians; (5) hospitalisations of clinicians from COVID-19; (6) hospital admissions from doorstep assessment service; (7) number of deaths within 4 weeks of using the doorstep assessment service; and (8) number of adverse event and serious adverse events within the doorstep assessment service.
Background
COVID-19 is an established threat whose clinical and epidemiological characteristics continue to evolve.1 In an effort to contain the disease, the NHS has recommended that remote consultations should be used when possible resulting in a significant shift away from in-person traditional face-to-face consultation.2 To support the safe, effective and efficient assessment of patients with suspected and confirmed COVID-19, we established a doorstep assessment service to compliment telephone and video consultations. This allows physiological parameters such as pulse, and temperature and oxygen saturation to be obtained to support further triage.
What existing evidence is there that this problem exists?
COVID-19 is a significant cause of morbidity and mortality globally with the UK having among the highest mortality rate in the world.6 Notably, health professionals are at increased risk of contracting COVID-19.7 Patients with suspected COVID-19 who need face-to-face examination beyond telephone or video consultation are typically assessed in either the GP surgery, the patient’s home, the local hot hub or admitted directly to hospital. There have also been a number of significant events across the uk related to a failure to assess physiological parameters that has resulted in avoidable deaths in patients with COVID-19 not least failures to identify silent hypoxia. To complicate the situation further, full PPE in primary care has been in short supply, and there is a widespread concern about personal safety.8 Even with the availability of PPE, risk assessments meant that some clinicians were unable to conduct face-to-face assessments.9
What evidence is there that other people have tried to solve this problem in the past?
Novel smartphone apps such as LifeLight that attempt to measure blood pressure, pulse respiratory rate and pulse oximetry without making physical contact with the patient have not as yet been validated to the standard required for accurate and safe assessment in acute primary care.10 On demand home-based self-guided examination devices are commercially available. Devices such as Tytohome are designed for mobile capture and transmission of ear, throat and skin images, heart and lung auscultation and temperature but not blood pressure and oxygen saturation.11 The current retail cost of each device is ~£236. The device is Food and Drug Administration (FDA) approved and have been evaluated in feasibility studies in clinically stable patients in the USA. There are no published reports that they have been used in COVID-19 and no data relating to their use in elderly patients. Remote assessment of patients with stable chronic disease using kiosks has also been reported. These are often placed in strategic locations in the community and clinical setting to provide remote access to a diagnostic assessment but are not suitable for doorstep assessment. During the current pandemic, other clinical commissioning groups have established an oxygen saturation probe monitor drop and collect service but as yet no data have been published.5 Equality and diversity issues have been reported in relation to the use of some technology used in remote assessment, especially those that require the use and operations of a mobile phone.
Is there any evidence for what works and what does not to solve your problem?
The equipment proposed for use in our doorstep assessment has been extensively researched and approved by the Medicines and Healthcare products Regulatory Agency (MHRA). As COVID-19 is an emerging disease, evidence of what works in terms of assessment remains limited. National Early Warning Score 2 (NEWS2) includes blood pressure measurement and oxygen saturation, although use has been suggested without the need for Blood Pressure (BP) if measurement does not alter management. There is no high-quality research on the value of NEWS2 outside of the hospital setting. If used, it should be done so alongside wider clinical assessment of the patient and in the context of changes over time. For the rapid diagnosis of suspected pneumonia in COVID-19, temperature, pulse oximetry, respiratory rate and heart rate are required. Blood pressure and auscultation should be reserved for situations where it will help to alter management when clinically indicated.
Measurement
Initial data collection focused on the number of assessments at the hot hub clinic during a single working week prior to the implementation to the doorstep assessment service to get a ‘snap shot’ of the problem. A retrospective case analysis was undertaken to identify the number of appointments that were available and how many traditional face-to-face appointments were being undertaken along with how much PPE was being used. In order to meet our project aim, we used the electronic medical record to measure the number of appointments available for both the doorstep assessment and hot hub clinic and the number of face-to-face assessments undertaken in both the doorstep assessment service and hot hub. Hospital admissions and deaths were also measured as secondary outcomes as they formed part of routine data collection. The cost of the service was also quantified.
Design
The doorstep assessment service was established alongside the implementation of a COVID-19 hot hub by St. Helens Clinical Commissioning Group (CCG). The quality improvement team included the local COVID-19 lead for primary care (SC), primary care network lead (DL), healthcare assistants (HCAs) (HJ), hot hub practice manager (CW) and local GPs (AT, DL, GI, HP, SC). The aim of the service was to allow community assessment of those patients with suspected COVID-19 infection while minimising exposure to primary care workforce and community spread. If needed, patient could be referred on for further assessment at the hot clinic, admitted to Accident and Emergency department (A+E) or managed by their own GP. A standard operating procedure (online supplemental appendices 1–8) was developed based on the application of principles of COVID-19 risk reduction for NHS staff—elimination if possible by minimising traditional face-to-face contact, hygiene measures and safe systems of work with election of correct use of PPE when needed (online supplemental appendices 9–11).7 Children were not included in the service. We followed the best available evidence emerging from the literature for how clinical assessment of patients with suspected and confirmed COVID-19 should be assessed; action points from regional significant event reports relating to need for physical assessment to take place where needed; epidemiological data identifying high-risk populations; and equality and diversity considerations including a need to provide care for shielded patients. We engaged with stakeholders in the development of the service through a weekly series of remote meetings. We refined our protocol by simulating assessments. A premortem analysis of the proposed service was undertaken to anticipate potential problems: lack of guidance and training on how to undertake an assessment; technology failure; infection control issues; and equality and diversity issues.
Supplemental material
Supplemental material
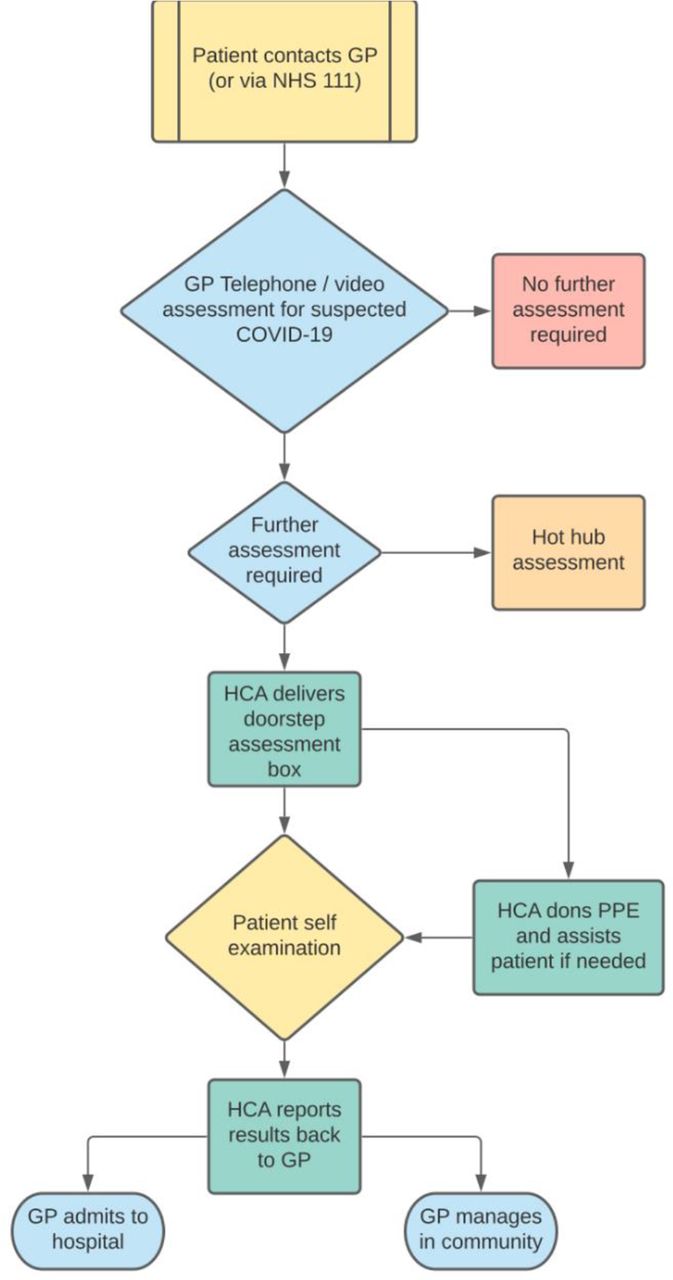
Suitable inclusion criteria include those patient with symptoms consistent with COVID-19 when a clinician in general practice has completed a telephone/video assessment and feels obtaining a NEWS2 score and more specifically an oxygen saturation would change management (online supplemental appendices 1–5). Notably, this included housebound patients or patients without own transport. In addition, clinicians at the hot hub who would potentially be undertaking face-to-face assessment on referred patients were also able to retriage patients referred for traditional face-to-face assessment to the doorstep assessment service if needed. Two forms of doorstep assessment review are available: (1) an assessment review for observations only undertaken by the patient themselves with support of a visiting HCA if needed or (2) a diagnostic review undertaken by a GP via video link with full vital signs (figure 1).The assessment involved delivering the assessment at the earliest opportunity and within the time frame of the review request. The equipment required to undertake the assessment is listed in box 1.

Doorstep assessment care pathway.
Doorstep assessment drop box equipment
Equipment.
Pulse oximeter.
Digital thermometer.
Sphygmomanometer with disposable cuff.
Tablet with Wi-Fi.
Digital stethoscope (Plan, Do, Study, Act (PDSA) 3 only).
The implementation team met remotely about every 4 weeks during the service. Providers and staff were educated about the service and questions about clinical flow were answered. New providers and staff, when orientated from doorstep assessment champions, were provided with an induction manual and were included in meetings were appropriate.
To ensure the sustainability of the service, we aimed to empower frontline staff and service users. We used data to identifiy and variation in performance and measure the impact of the service over time. We planned for the service to be scaled up and extended post-COVID-19 with adaption to local needs, new environments, patient and staff groups by making use of currently available equipment and resources and becoming the new way of operating
Strategy
In our first PDSA cycle, we decided to implement the assessment service for patients with suspected COVID-19 carried out by HCAs. This was done to find out the impact of running the service during a busy time for the local primary service during the pandemic. After discussions with the participating practices and St. Helens CCG. doorstep assessment result could also be entered directly into the patient’s notes using Egton Medical Information System (EMIS) Enterprise. This PDSA cycle was done primarily to test feasibility of the service for patients. Informal feedback from staff, providers and patients were mostly positive and was used to inform our second cycle. Only 15% of patients using the service were male. The mean age of patient mean age of patients was 54 (range 21–83) years. A small number of referrals received were not appropriate for the service.
For PDSA cycle 2, we enabled referrals to be made directly through EMIS using the existing extended access appointment booking service. We introduced an online template for clinicians to follow when making a booking to ensure the referrals received were appropriate. We shared emerging UK observational data for risk of death and relevant service perfromance data, encouraging GP surgeries to have a low threshold for referring individuals at high risk of death. We tailored the service to align with local and national NHS England recommendations on shielding and testing. For PDSA cycle 3, we assigned hot hub champions to help maintain continuity and share experience within the service. A digital stethoscope (Thinklabs) was made available to clinicians at the hot hub. One of the GP assistants was trained to set this up for clinicians to use.
Result
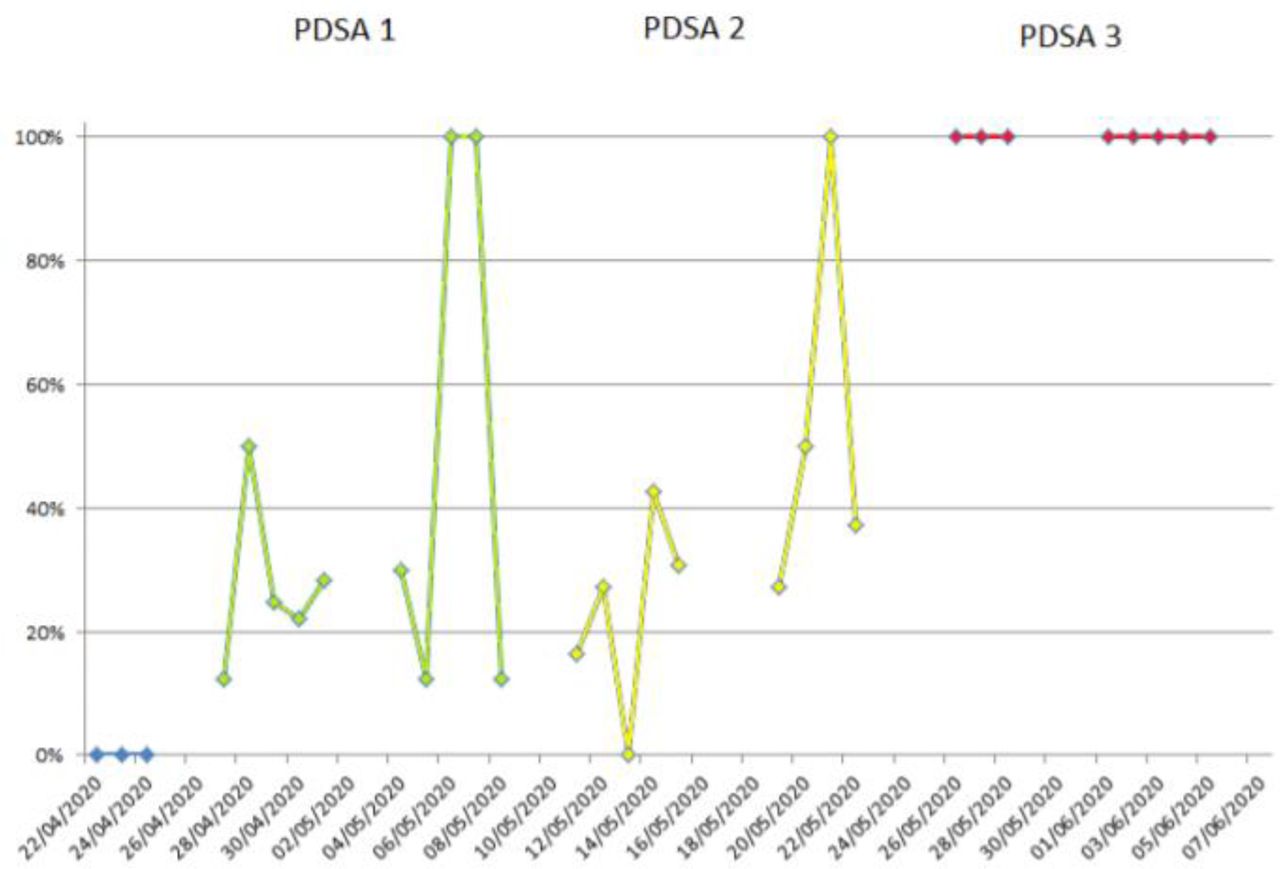
The main outcomes for the study were change in the proportion of assessments of vital signs for patients with suspected COVID-19 in routine care and change in the proportion of non-face-to-face assessments for patients with suspected COVID-19 at the hot hub. At baseline, all patients were being assessed through traditional face-to-face assessment at the hot hub. After PDSA 1 with the introduction of the doorstep assessment, 27% of patients had non face-to-face assessments. This increased to 28% after PDSA cycle 2% and 100% after PDSA cycle 3 (figure 2)

Proportion of non-face-to-face assessments.
On the single day when the doorstep assessment service was not available, the proportion of traditional face-to-face assessments reverted back to 100%. At baseline, there was no doorstep assessment service available, and therefore, no extra physical assessment made. After PDSA 1 with the introduction of the doorstep assessment, 27% (20) of patients had non face-to-face assessments. This increased to 28% (23) after PDSA cycle 2 and 100% (43) after PDSA cycle 3 (figure 3).

Number of physical assessments over time.
The total number of doorstep assessments carried out over the three 2-week cycles was 61 (PDSA 1=20, PDSA 2=23 and PDSA 3=18) (figure 2). There were five (8%) hospital admissions to hospital from the doorstep assessment service; in one case, an ambulance was called prior to the arrival of the GP assistant. Four of these patients referred from the doorstep assessment went on to have COVID-19 (mean duration of admission 5 days, range 1–12). This compares with seven admissions (5%) from the 138 patients reviewed at the hot hub over the same time period (figure 4). Five of the patient referred from the hot hub patient went on to have a diagnosis of COVID-19 (mean duration of admission 5 days, range 1–13) (figure 4). All remaining assessments 56 (92%) were followed up by the patient’s usual GP. Three patients had a follow-up doorstep assessment. No patient who underwent a door step assessment went on to have an assessment in the hot hub or vice versa. There were no patient deaths within 4 weeks of using the doorstep assessment service. There were no adverse events or significant adverse events associated with the doorstep assessment service. Data from one of the referring GP surgeries (list size 4831 patients) during the period of the project reported 11 cases of suspected COVID-19. Of these, seven were referred for the doorstep assessment service and one to the hot hub. Three patient did not have any further assessment (mean age 34 years). For these three patients, assessment beyond video consultation was not considered necessary by the GP. All three patients made a full recovery. All patients with frailty were reviewed through the doorstep assessment service. There were no clinical staff absences with suspect COVID-19, and no clinicians were hospitalised with COVID-19. The mean age of patients assessed with the doorstep assessment was 56 (range 21–84) years, and 26% were male. The cost of running the service using the GP assistant was £520 per week. The cost of the drop box was £50 for the basic box (oxygen saturation monitor: £25 and blood pressure machine: £25), £100 with a tablet included (Amazon Fire: £60) and £507 with a digital stethoscope (Thinklabs stethoscope: £397).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient flow through the hot hub and doorstep assessment service.
Lessons and limitations
The project’s aim was to try to increase the proportion of assessments of vital signs for patients with suspected COVID-19 at the same time increase the proportion of non-face-to-face assessments for these patients, which was achieved. Trying to improve the quality of the doorstep assessment service during the COVID-19 pandemic was challenging given the evolving nature of the pandemic, changing public health measures and the emergence and evolution of new evidence and guidelines during the pandemic. Establishing PDSA cycles and regularly communicating back to hub was vital given the changing situation so that the service could adjust and adapt. Given the cooperative nature in which the service was run, there was a relatively high turnover of clinicians running the hot hub service, which made establishing and maintaining expertise within the service challenging in terms of maintaining institutional knowledge and expertise. In contrast, we were fortunate to have a small number of GP assistants (three) running the doorstep assessment service.
Evaluating data from the service within the PDSA cycles was useful in that it allowed us to identify that service was not necessarily being used in patients at the highest risk of death, for example, male, elderly and obese.12 The typical GP surgery in St. Helens has approximately ~38% male population. Coupled with this, the proportion of males contacting their GP with suspected COVID-19 symptoms appears to be lower than in females. There is also a long history of late presentations with other illnesses such a cancer and cardiovascular disease in male population in the region. We hypothesise that male patients are presenting later with more severe symptoms and going directly to secondary care. It also highlights the potential for inequality when introducing such a service and that the inverse care law may be in operation.13
Establishing a baseline during the pandemic was difficult given the changing epidemiology of the disease and the reconfiguration of local services. The baseline measurement period was relatively short due to: (1) patient and practitioner safety concerns along with (2) local and national concerns regarding the availability of effective PPE and (3) increasing patient demand. The target of a 10% increase in the proportion of patients with vital signs assessment and the 10% increase in non-face-to-face assessments was arbitrary and should we conduct the project again would recommend a much higher target of 50%–100% as we found it at least theoretically possible for all assessments to be conducted non-face-to-face. The study was conducted during the first lockdown, and the number of patients presenting to local GPs with suspected COVID-19 symptoms was falling in PDSA cycle 3, and as a result, the number of physical observations remained static. Future research under experimental conditions would help to evaluate the safety and effectiveness of doorstep assessments.
The changes made in PDSA 2 resulted in a marginal improvement in reducing the proportion of traditional face-to-face contacts with PPE. In contrast, the introduction of the digital stethoscope in PDSA 3 resulted in a step change, which eliminated traditional direct face-to-face contact. Training one of the GP assistants to set up the stethoscope for clinicians reduced the anxiety of using a new device. The lack of utilisation of the remote video consultation service was surprising given the attention this has received nationally. Some clinicians felt this was ‘not needed’ and ‘added little to assessment over the phone’. A number of regions have established a hot hub service, but to our knowledge, relatively few have introduced a doorstep assessment service. We anticipate that our findings may be useful should a second wave of COVID-19 or future pandemic occur. We reflected on the scalability of the intervention using the Intervention Scalability Assessment Tool identified workforce provision as a key challenge.14 We achieved this during the project through a high level of cooperation between local GP providers, but we are now looking to make this more sustainable by linking this workforce provision with the roll out of NHS virtual wards. Evaluating the service through a quality improvement project has helped to facilitate local discussions on how urgent care could be better coordinated following the COVID-19 pandemic given that a number of the findings and service changes were felt to be generalisable to the existing and emerging urgent care and chronic disease services; indeed, the doorstep assessment service has recently been adopted locally by the community nursing team to assist with chronic disease management.
Conclusions
To our knowledge, this is the first quality improvement project completed during the COVID-19 pandemic. The doorstep assessment service was able to increase the proportion of assessment completed for patients with suspected COVID-19 while at the same time reducing the number of traditional face-to face assessments required and preserving PPE equipment. The majority of patients undergoing a doorstep assessments are followed up by their own GP maintaining continuity of care rather than leading to admission to hospital. Further evaluation of doorstep assessment services under experimental conditions would help to establish their utility beyond the COVID-19 pandemic and whether their use should be scaled up and spread in urgent care and different settings, for example, care homes, work places and local communities.
Data availability statement
All data relevant to the study are included in the article.
Acknowledgments
We would like to thank St. Helens general practitioner provider group and St. Helens Clinical Commissioning Group and the Royal College of General Practitioners (RCGP) for their support on this project.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was published. A misplaced ‘The’ has been removed from the starting of the abstract.
Contributors Conception or design of the work: GI, DL, AT and SC. Data collection: GI, AT and HJ. Data analysis and interpretation: GI, DL, AT and SC. Drafting the article: GI, DL, AT, HJ, CW and SC. Critical revision of the article: GI, DL, AT, HJ, CW and SC. Final approval of the version to be published: GI, DL, AT, HJ, CW and SC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.