Article Text

Abstract
An emphasis on active ageing could help to delay the onset of frailty. In Singapore, Senior Activity Centres provide free and guided group exercise sessions for older adults. However, one such centre had very low participation rates among community-dwelling older adults despite running standardised programmes. Based on a needs analysis from a prior project, this paper reports on strategies implemented to improve the daily centre-based group exercise participation rate among community-dwelling older adults. Using the behaviour change wheel model, participant motivation domains were identified as primary gaps, while the psychological capability and physical opportunity were categorised as secondary gaps. A logic model was used to design a project to respond to these identified gaps and guide the evaluation approach. Three strategies were implemented over a 4-week period and reviewed at 6 months: (1) promotion of the exercise classes, (2) delayed rewards for participation and (3) health ambassadors. Evaluation findings highlighted that more resources were needed for the training of community-dwelling older adult healthcare ambassadors in the use of motivational interviewing. The interventions were found to be efficacious in increasing daily group exercise participation rate at the centre, from an average of three to nine participants per day over the 4 weeks. Furthermore, more than 60% of these participants achieved the WHO’s weekly minimum exercise recommendation for older adults (150 min moderate-intensity physical activity). To increase the engagement of older adults in physical activity or exercise participation, we recommend the use of behaviour change wheel model and the use of community-based health ambassadors. In conclusion, the project found improved daily centre-based group physical exercise participation rates when all the domains in the behaviour change wheel model were addressed.
- community health services
- exercise
- quality improvement
- health behavior
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
A Senior Activity Centre (SAC) in the southern region of Singapore was identified for programme review and improvement. The SAC is a community initiative, typically operated by non-governmental agencies to provide physical and social activities for well older people, aged 60 years and above, and primarily living in the lower to middle socioeconomic strata. A programme coordinator runs exercise programmes daily to assist older adults to meet the recommended physical activity guidelines.1 The SAC runs a series of classes which includes video-recorded instructional exercise demonstrations, resistance band exercises, seated upper and lower limbs exercises, Chinese qigong and instructor-led callisthenics. The SAC primarily serves to support 90 residential households for physical and social activities and serves as a health promotion service for these residents. This SAC has a maximum capacity of 15 participants for each group exercise session, however, at the time of review it only had three participants. Therefore, the aims of this project were to improve the average daily group exercise participation utilisation among the residential older adults from 20% (three participants) to 60% (nine participants) and to assist participants to achieve the recommended daily physical activity standards for older adults.
Background
Ageing well is an important consideration and recent studies have explored the importance of physical and social activities in maintaining the well-being of older adults and in frailty prevention.2 3 Physical impairments can be a barrier to social activity participation among older adults and thus interventions to improve physical health are viewed as crucial for healthy ageing.4 As an illustration, an older adult with difficulty in walking may become reluctant to leave home to participate in community activities, and the family members may prefer the older adult to stay at home, assuming that this would reduce the risk of outdoor falls. The SACs are strategically sited close to where older people live, precisely to improve accessibility to physical and social activities participation for community-dwelling older adults. In this study, a SAC has very low older adult participation in centre-based group physical exercise classes.
To review best practice for exercise programmes for older adults, the first author completed a scoping review of the published and grey literature.5–21 The findings of the review identified the use of exergaming, resistance training, structured Otago exercise programme, tai chi, structured group exercises and high-intensity training, performed once or twice per week for one to 12 months and 60 min per session, to be beneficial for older adults.5–15 Sports and exercises are also common among fit and healthy older adult citizens.16–21 The benefits include reduced falls incidence, reduced fear of falling and improved physical health.22–28 These findings reinforced the importance of formal and regular exercise programmes for older adults and the importance of developing a sustainable programme that is engaging for community-dwelling older adults at the SACs.
As part of a quality assurance project, 56 community dwelling older adults, between the ages of 65 and 75 years were interviewed or participated in focus groups run by the first author. Twenty-six older adults agreed to be interviewed and 30 participated in focus groups and all addressed the question on the primary barriers to engaging with exercise at the SAC. The interviewer used the motivational interviewing approach29 and paid special attention to the participants’ level of motivation to engage with exercise and subsequently categorised each participant on their level of readiness for behaviour change. Motivational interviewing is a communication strategy that engages the individual by exploring the strengths and motivations for change that eventually leads to a behaviour change,29 which is pivotal for them to reflect on their motivation to participate in physical activity.30 Although the majority of respondents found physical exercises important and indicated that they would engage in community physical exercises or activities, such enthusiasm was absent in the SAC studied.
Primary barriers reported were the lack of awareness of the exercise classes, impaired mobility making it difficult to attend classes, limited health literacy in understanding the value of exercise and in the value of having physical signs and symptoms managed by a physiotherapist. A key theme identified was issues with motivation, with individuals being at different stages of readiness for change according to the transtheoretical model.31 Transtheoretical model is an individual-level behavioural change theory that recognises the individual’s specific stage of readiness for change. The person could move from one stage to another, in either direction depending on decisional balance that is influenced by incentives or disincentives for change.31
In response to these findings, the authors designed a project to use health behaviour change strategies to increase regular centre-based exercise participation among the older adult residents. The behaviour change wheel was originally designed to promote successful behaviour change by systematic attention to three key domains of behaviour change (Capability, Opportunity and Motivation, COM) and their subdomains of physical and psychological capability, physical and social opportunity, and reflective and automatic motivation. Refer to figure 1, in which words in black font form the original behaviour change wheel.32 Since all domains of the COM-Behaviour (COM-B) model must be present for effective behaviour change, all domains were used to identify behavioural domain gaps with a view to design feasible and sustainable activities to address these gaps and promote lasting behaviour change.

Behaviour change wheel gap identification for intervention implementation.
Measurement
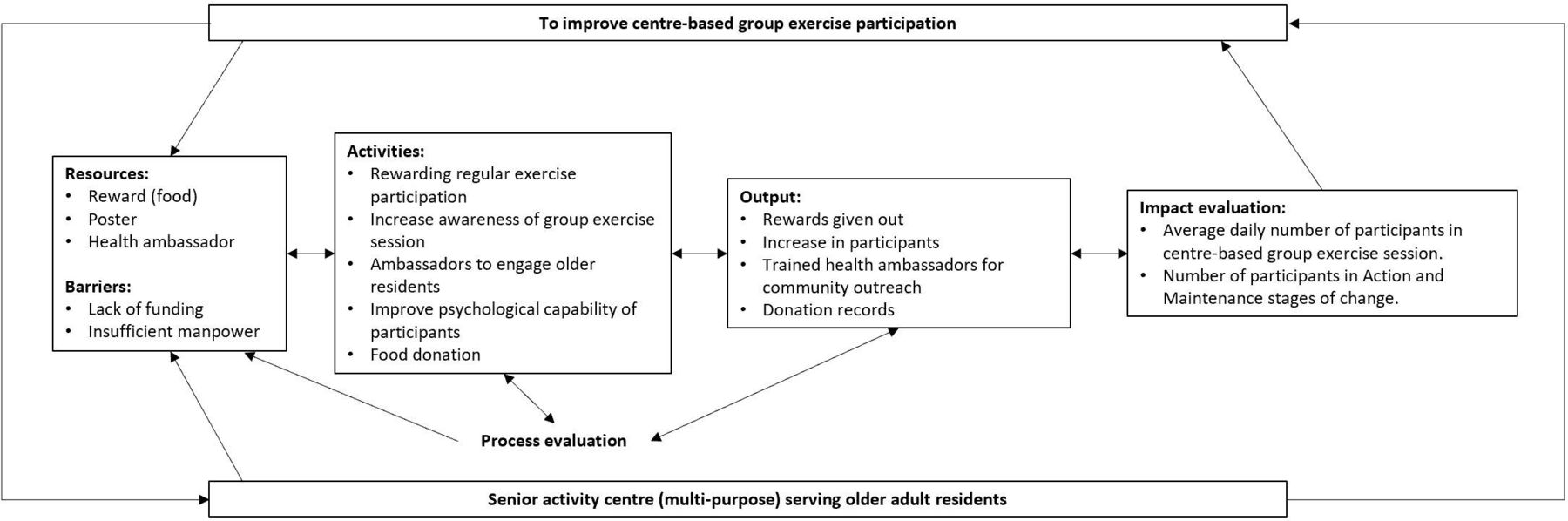
A logic model was adapted to guide the project design and evaluation (figure 2).33 First, process evaluation was used to identify barriers to the project and facilitators to steer the project towards its objectives.34 Process evaluation at every phase of the implementation of this project served as an important control to improve the chance of project success by overcoming barriers. Evaluation of the changes in average daily group exercise participation rate in the SAC helped to determine if the primary aims had been achieved, alongside the participants’ stage of change. The baseline measure is tabulated in table 1. A participant register was used by the programme coordinator to collect daily attendance records and at the end of each month, the weekly exercise frequency of each participant was computed. To ensure reliability, the centre manager audited the accuracy of the soft-copy attendance records prepared by the programme coordinator against the physical attendance records. The stage of change was obtained from the participant register that included the exercise participation start date (table 2). Apart from the interventions described in this paper, no other competing interventions or national initiative occurred during the period of project evaluation.

Project logic model.
Participation rate (formative evaluation)
Readiness of change (impact evaluation)
Design
Preintervention data collection was completed ordinally from April to July 2018 and the interventions were implemented from August 2018 with a final evaluation at the end of January 2019. The subdomain gaps identified with the COM-B model were primarily automatic and reflective motivation, and secondarily gaps were psychological capability and physical opportunity (figure 1). Hence, the interventions for implementation were designed to address these gaps. Three interventions were implemented to increase participation rates within the SAC: (1) poster publicity, (2) participation rewards and (3) health ambassadors.
Poster publicity raises awareness about the exercise session (physical opportunity) and introduces rewards (automatic motivation) for regular centre-based group exercise participation. The poster was prepared in two languages, English (the default lingua franca of Singapore) and Mandarin (main language used among majority of participants in the SAC) and prominently placed at the entrance of the SAC. The rewards for participation included non-perishable food such as rice and cereal, and other daily commodities such as toiletries.
Health ambassadors were introduced to improve daily participation rate through active engagement and an effort to socially influence older adults new to the SAC.35 36 Two regular SAC group exercise participants verbally consented to help as onsite health ambassadors and were trained on the motivational interviewing approach to engage new participants. Open-ended questions were used to explore new participants’ perspectives of healthy behaviour and on the benefits of physical exercise (psychological capability). The health ambassadors would refer the exercise participants to a physiotherapist in the centre if they were unable to address in-depth knowledge queries. The benefits of exercise were further reinforced with existing Health Promotion Board booklet for the older adults, which conveyed falls prevention and exercise information to the participants in the four national languages, namely, English, Mandarin, Malay and Tamil. Existing participants supported the health ambassadors within the centre through social opportunity with the new participants. The social opportunity allowed participants to mutually share their experiences of the benefits of exercise and prospectively, the new participants would develop self-awareness on these benefits to reinforce motivation (reflective motivation).37
Strategy
To ensure the successful implementation of the project, we evaluated each intervention adopted. Process evaluation was used to address barriers encountered during the 4-week project, while impact evaluation captured change at 4 weeks and again at 6 months postimplementation.
First, the food donation process was reviewed to ensure that the centre had complied with the policy in accounting for the values of donated goods. A challenge highlighted by the programme coordinator was a delay in procuring the rewards. Receiving rewards provided an opportunity to reinforce the importance of exercise and physical activity participation beyond the minimum weekly recommendation.
Second, the team sought opinions from four new participants who were attracted by the poster and a common comment was to enlarge the section on rewards to better attract public attention. The team noted the feedback and edited the poster. Another suggestion was for the A4-poster to be enlarged to A3 print, however, due to space constraints for notices, we were not able to use the suggestion. The posters were placed at approved and prominent locations within and around the centre.
Third, the two health ambassadors approached eight residents and successfully encouraged six residents to attend the SAC exercise sessions, while two declined because of other daily routine. Half of the new participants motivated to participate by the health ambassadors influenced another three peers to participate in the exercise session. Additional supportive training was conducted for the health ambassadors to ensure that motivational interviewing was used correctly.
Results
The baseline number of exercise participants per day ranged from two to four. In the intervention implementation week, the participation improved (average of 8 participants per day). By the end of the 4-week intervention implementation, all 15 participants achieved a minimum of twice weekly moderate intensity exercises and more than 60% of the participants achieved at least 150 min/week of moderate intensity exercises (table 1).
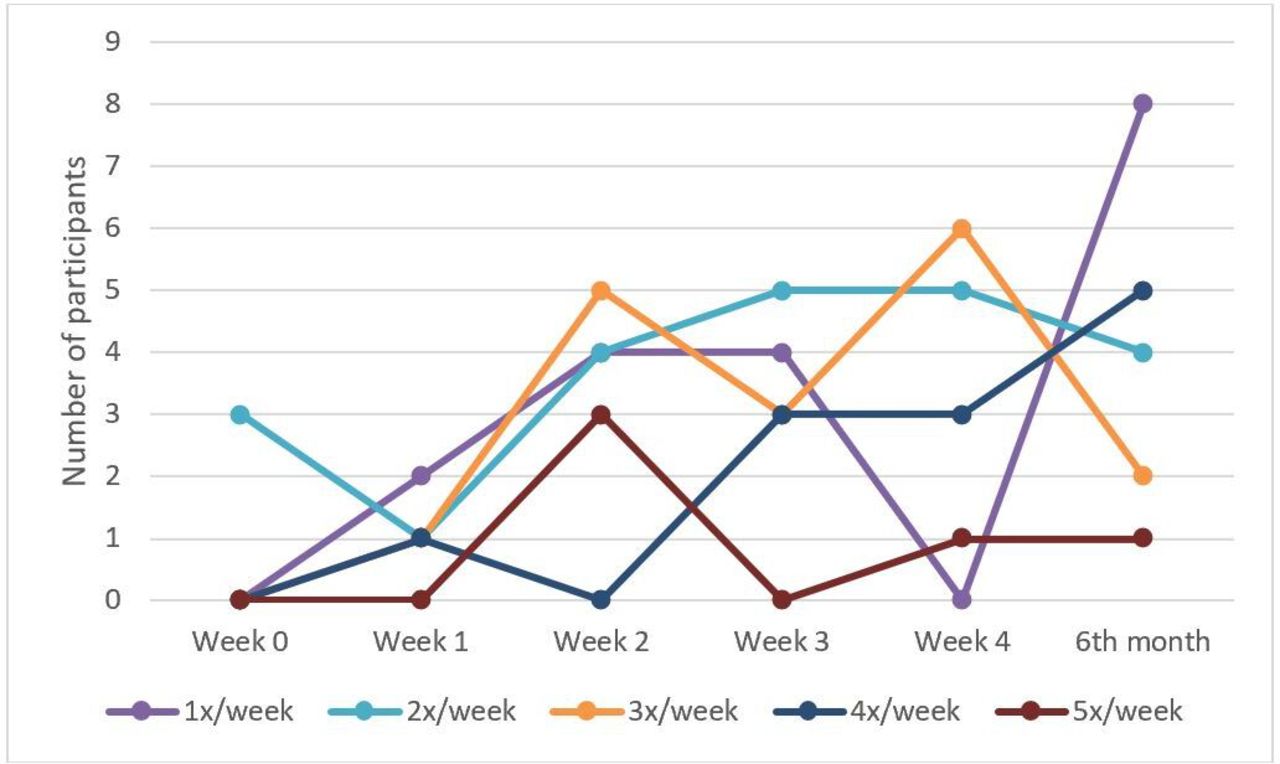
In week 1, the health ambassadors identified four participants in the precontemplation stage of change and two in the contemplation stage of change for progression into the action stage. Another three peers of the newly approached participants were contemplating about group exercise session participation. Those who were influenced by the poster had plans to participate in some form of physical activity and they managed to influence an accompanying peer in the precontemplation stage to exercise. By the end of week 2, all new participants were in the action stage of change (table 2), but one of them regressed from the action to the contemplation stage in subsequent weeks as the functionally independent participant felt that exercise was unnecessary. The results are charted in figure 3.

{kind=link}
{kind=link}
{kind=link}
Run chart for participation frequency change.
Overall, the project demonstrated sustainability at 6 months and continued to show improvement for the number of participants in the maintenance stage (eight participants), whereas in formative evaluation, the average number of participants per day was maintained (table 2). There were also more participants (20 participants) who registered to participate by 6 months. The data audit of soft-copy tallied against physical record, indicated that the data collected and analysed were accurate with no missing data.
Lessons and limitations
A strength of this project was the use of the COM-B model to identify health behaviour gaps and to design a project to influence positive behaviours among older adults. Our quality improvement project followed the recommendation of a recent systematic review that suggested a multifactorial approach in promoting physical activity among community-dwelling older adults.38 Our project had successfully addressed the gaps of the group exercise programme in automatic motivation, reflective motivation, physical opportunity and psychological capability domains of the COM-B model.
Rewards can change behaviour through physiological arousal and encourage learning, although effectiveness varies between individuals.39 This project demonstrated that indirect monetary reward sufficed in achieving automatic motivation in improving physical activity participation among the older adults, which was similar to direct monetary incentives used in a recent randomised controlled trial among working adults.40 A similar effect was noted in an earlier national initiative, the National Steps challenge, which was designed to encourage citizens to be physically active through rewards such as grocery vouchers.41 This phenomenon could be explained through the Maslow’s hierarchy of needs model and food is a basic need in the model,42 especially for older adults who may have a limited budget for meeting their primary needs.
This project used delayed reward and found that a higher proportion of older adults maintained regular exercise. The timing that rewards are given could influence the maintenance of desired behaviour.43 If the reward was given too early (immediate), the participants were less likely to stay engaged in the physical activity, whereas when reward was delayed, participants were three times more likely to maintain their physical activity.43 Delayed reward is also a long-term motivator because it can maintain novelty and interest.39
In a recent systematic review, the authors concluded that the use of self-regulatory strategies to achieve behaviour change were insufficient and had low efficacy in achieving desired change.44 Furthermore, a large randomised controlled trial, the LIFE study, showed that a structured exercise programme of moderate intensity carried out with supervision and at home was superior to a health education strategy in improving physical health for longer-term benefits.45 Thus, direct information sharing lacked significant physical health benefits for the older adults. That said, equipping participants with knowledge is a component in the COM-B model. Similar to other established behaviour change models, the COM-B model uses motivational interviewing to empower participants with self-reflection strategies.30 46 According to Copeland et al, motivational interviewing achieved behaviour change through the development of components such as improved self-efficacy, self-control, motivation and planning. Furthermore, trained users of motivational interviewing could have a direct influence on health outcomes.46
Health ambassadors played a pivotal role in engaging the older adults for behaviour change in our project. Similarly, a recent health behaviour change programme used ambassadors to drive physical activity and dietary habits to achieve desired behaviour change.47 This was possible because the ambassadors had more communication time with the participants in our study. A society rich in communication technology usage such as social media access with mobile communication devices could strengthen health message communication.48
The benefits of group exercises extend beyond physical health gains, which included psychosocial aspects of health. The social opportunity for the older adults to interact allowed the development of friendship, reducing loneliness and formation of interest groups. In a recent systematic review, the availability of social support increased physical activity participation.49 The importance of social opportunity among older adults was best reflected in a recent meta-analysis, which pooled studies of older adults who lived in isolation and especially those who lived alone were at increased risk of early death.50 Although the endpoint of the project was to achieve increased exercise participation, future projects could explore health outcomes of the participants. Exercise participants should live longer and healthier lives, thus achieving the national vision of healthy and active ageing.
Despite the success of the project, it had a few limitations. Successful engagement of older adults requires manpower. A drop in the number of attendees was noticed on the days when the programme coordinator was unavailable to support the programme. Further, we could not continuously monitor the motivational interviewing conducted by the health ambassadors after the initial training phases. In future, a surrogate measure through monthly review of participant drop-out or regression in the stages of change could help to assess the efficacy of motivational interviewing by the health ambassadors. Finally, this programme was not designed for a pandemic which did not allow ongoing follow-up.
Conclusion
The implemented interventions with the use of the COM-B model for effective behaviour change had achieved an improvement in participation rate from 20% to 60% at the end of 4 weeks, which was sustained 6 months postintervention implementation. Although the planning phases of the project required substantial manpower resources, once implemented, the cost to sustain the initiative was relatively low. Hence, the success of the project could be replicated by other SACs looking at improving the engagement of older adults with social and physical activities with a view to improving their quality of life and delaying onset of frailty.
Acknowledgments
We would like to thank Ms Chen Liyun (Occupational Therapist), Ms Su Sandi Aung (Physiotherapy Associate/Programme Coordinator) and Ms Jolin Teo (Administration Assistant) for their contribution towards the project planning and execution. In addition, we would like to thank Ms Su Sandi Aung for her role in data collection throughout the project phases. We extend our thanks to the project sponsor, Mr Cyril Tee (Divisional Director), for supporting the project initiative from September 2018.
References
Footnotes
Contributors BCK was principally responsible for all phases of the study design and implementation, data collection and analysis, and draughting of the manuscript. WPW provided intellectual inputs to all phases of the study design and review of the final manuscript. LR provided intellectual inputs to all phases of the study design, data analysis and review of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.