Article Text

Abstract
Background Cardiac resynchronisation therapy (CRT) requires intensive, complex and multidisciplinary care to maximize the clinical benefit. In current practice this is typically a task for highly specialised physicians. We report on a novel multidisciplinary, standardised CRT care pathway (CRT-CPW). Experienced clinicians developed a CPW with simple and broadly applicable aids based on clinical evidence and identified shortcomings in the current CRT care. The resulting CPW was implemented at the Maastricht University Medical Center, aiming at a transfer from heterogeneous physician-led care to standardized nurse-led care.
Methods Two CRT patient cohorts were compared in this analysis. The benchmarked usual care cohort (2012–2014, 122 patients) was compared with the CRT-CPW cohort (2015–2017, 115 patients). The primary outcomes were process-related: number of physician consultations, nurse consultations, length of stay (LOS) at implantation and total hospitalisation days during 1-year follow-up, and referral-to-treatment time. Clinical outcomes were assessed to adress non-inferiority of quality of care.
Results Patients in the CRT-CPW cohort consulted nurses and technicians significantly more often than patients in the usual care cohort (2.4±1.5 vs 1.7±2.0, p<0.0001 and 4.3±2.5 vs 3.7±1.5, p=0.063, respectively). Patients with CRT-CPW consulted physicians significantly less often (1.7±1.4 vs 2.6±2.1, p<0.001). Referral to treatment time was significantly reduced in the CRT-CPW group (23.6±18.4 vs 37.0±26.3 days, p=0.002). LOS at implantation and total hospitalisation days were significantly reduced in the CRT-CPW group (1.1±1.2 vs 1.5±0.7 days, p<0.0001 and 2.4±4.8 vs 4.8±9.3, p<0.0001, respectively). Clinical outcome analyses showed no significant difference in 12-month all-cause mortality and heart failure hospitalisations.
Conclusion The introduction of a novel CRT-CPW resulted in a successful transition of physician-led to nurse-led care, with a significantly reduced resource use and equal clinical outcomes. Future evaluations will focus on impact on outcomes versus costs, to evaluate cost-effectiveness of the CRT-CPW.
- efficiency
- organizational
- healthcare quality improvement
- length of stay
- nurses
- time-to-treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cardiac resynchronisation therapy (CRT) is one of the most successful heart failure (HF) therapies that have emerged over the last few decades. Several randomised clinical trials have shown that CRT reduces symptoms of HF, improves exercise capacity and quality of life and reduces hospitalisations and mortality.1–4 Clinical guidelines of the European Society of Cardiology and the American College of Cardiology Foundation/American Heart Association endorse these results and recommend utilisation of CRT in selected patients with HF.3 5–7
Despite guidelines and experts’ consensus, variability in patient selection, implantation techniques, in-hospital management and follow-up is observed in clinical practice.8–10 A recent multicentre registry revealed significant heterogeneity in both definition of response and non-response to CRT, and consequential optimisation of therapy. Overall the rate of suboptimal benefit from CRT remained as high as 30%.11 In order to overcome suboptimal benefit from CRT, care for these patients requires thorough selection for treatment, skilled implanting physicians and a comprehensive follow-up treatment and comorbidity management. Few studies have introduced CRT care programmes, including resource intensive, specialised follow-up, personalised therapy delivery and frequent visits of patients after CRT implantation. These studies generally show a positive effect on outcomes.12–14 The extensive and comprehensive nature of these optimisation programmes however limits the widespread implementation in clinical practice.
In general HF care, the transition from physician-led to nurse-led care has been well accepted, as studies show that nurse-led multidisciplinary HF programmes result in a reduced risk of HF hospitalisation. These programmes have been broadly adapted in clinical practice.15–19 Moreover, studies have shown that structured aids in HF care programmes can lead to improved adherence to guidelines.14 20 21 These developments in general HF care, however, have not been introduced into CRT care programmes yet.
The present study describes the development and implementation of a CRT care pathway (CRT-CPW), a blueprint for CRT care transition from physician-led to a standardised, nurse-led care programme, which aims to reduce healthcare and patient burden at equal or better quality of care, with help of structured aids and advanced planning.
Methods
CRT-CPW design
In 2013 three expert centres (Maastricht University Medical Center (MUMC+), the Netherlands; Liverpool Heart and Chest Hospital, England; and Rigshospitalet Copenhagen, Denmark) took the initiative to collectively design a CRT-CPW. Consensus meetings were conducted to evaluate and discuss currently available evidence and local experiences in patient evaluation and selection, device implantation, follow-up care and process-related factors. CRT-CPW design was deepened into an operational CRT-CPW for the MUMC+, detailing actions and resources needed, as shown in figure 1. Checklists were created to be applied during specific contact moments with the patient (online supplemental figures 1-4). The final consensus CPW consisted of four important elements aiming to maintain or improve quality with effective resource use: (1) structured involvement of both heart failure and electrophysiological expertise in the process steps, (2) transition of tasks from physicians to specialised nurses and technicians, (3) ensuring to check and control variables contributing to optimal CRT care by means of checklists at each process step and (4) structured planning of patient visits (including hospitalisation for implantation) for each process step, with one-stop-shop visits, to reduce unnecessary resource use and patient burden (figures 1–3).
Supplemental material

Operational CRT-CPW; referral review and pre-assessment. An overview of the referral review and pre-assessment parts of the implemented operational CRT-CPW. Steps a patient goes through in the care pathway are indicated with content of the assessments and structured AIDS available for the assessment. CRT, cardiac resynchronisation therapy; CRT-CPW, CRT care pathway; HF, heart failure; ICD/PM nurse, implantable cardioverter-defibrillator/pacemaker nurse; QoL questionnaire, Quality of Life questionnaire. *The referral review and pre-assessment checklists are available in the online supplemental material.
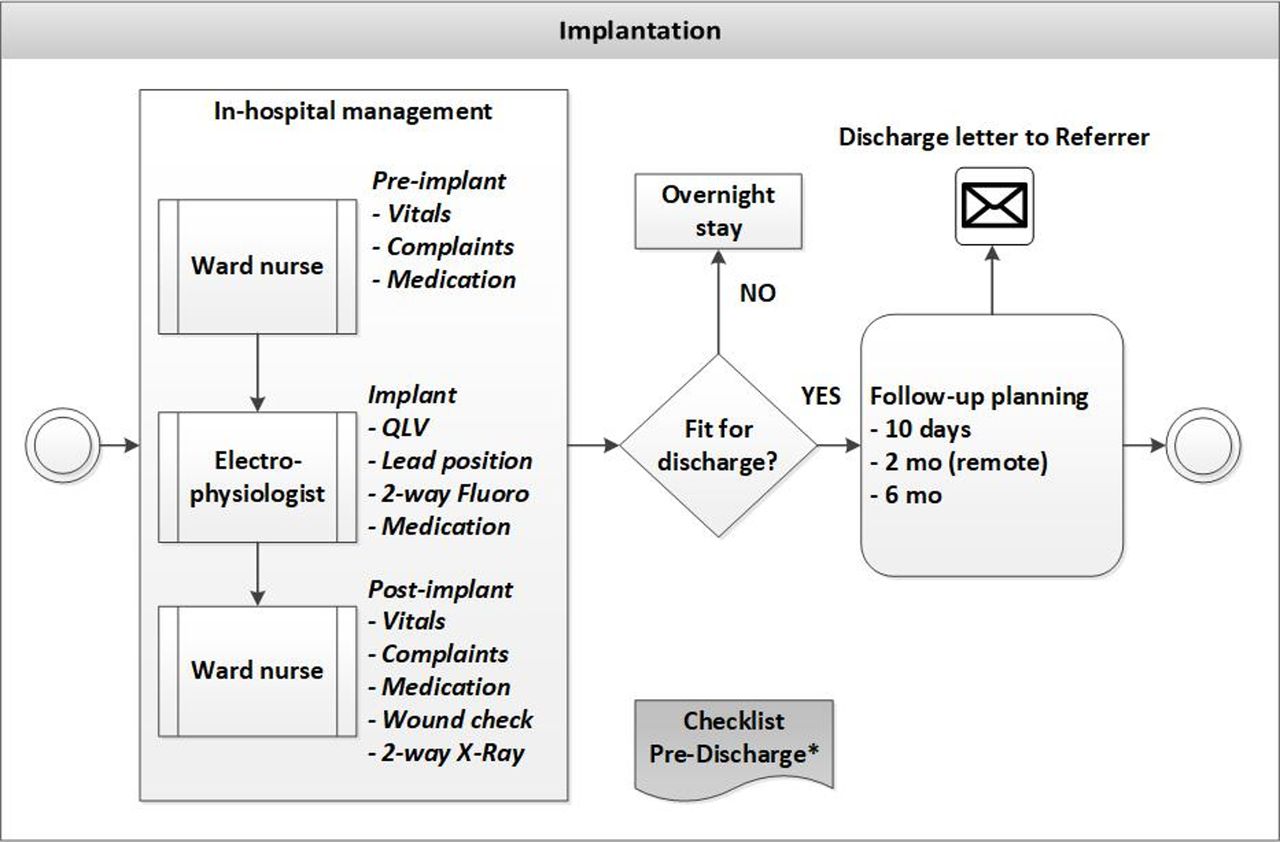
Operational CRT-CPW; implantation. An overview of the implantation part of the implemented operational CRT-CPW with steps a patient goes through in the care pathway are indicated with content of the assessments and structured AIDS available for the assessment. CRT, cardiac resynchronisation therapy; CRT-CPW, CRT care pathway; mo, months. *The pre-discharge checklist is available in the online supplemental material.
{kind=link}
{kind=link}
{kind=link}
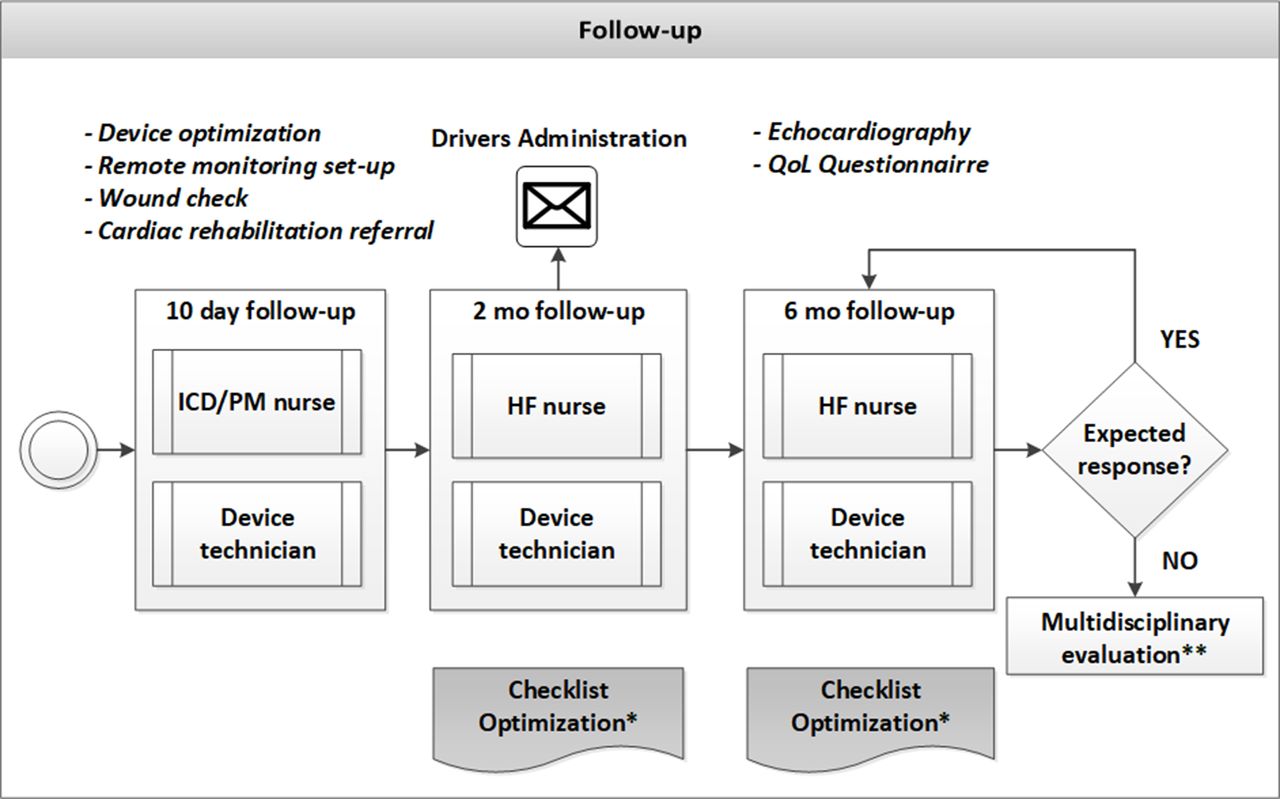
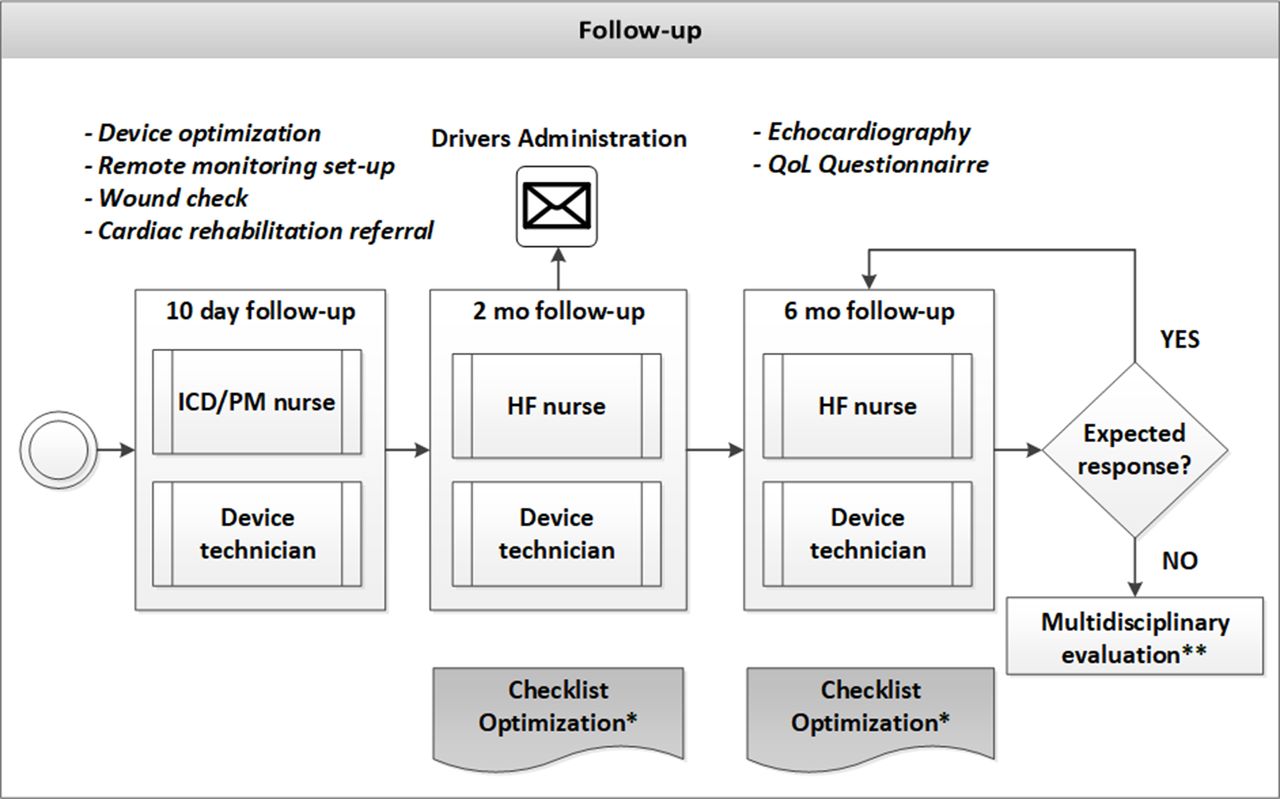
Operational CRT-CPW; follow-up. An overview of the follow-up part of the implemented operational CRT-CPW with steps a patient goes through in the care pathway are indicated with content of the assessments and structured AIDS available for the assessment. CRT, cardiac resynchronisation therapy; CRT-CPW, CRT care pathway; HF, heart failure; ICD/PM nurse, implantable cardioverter-defibrillator/pacemaker nurse; mo, months; QoL questionnaire, Quality of Life questionnaire. *The optimisation checklist is available in the online supplemental material. **The multidisciplinary evaluation is the same as the referral review multidisciplinary evaluation.
Operational CRT-CPW
For patients referred for CRT implantation a weekly multidisciplinary meeting with HF cardiologists and electrophysiologists was set up to assess eligibility. (figures 1–3) Baseline parameters possibly affecting patient outcomes are checked following the ‘referral review’ checklist (online supplemental figures 1–4). In case additional workup is needed for a patient, the referring physician is contacted and the patient is re-evaluated after completion of diagnostic evaluations and/or optimisation of general HF therapy. After approval for CRT, the implantation is scheduled; a one-stop-shop outpatient visit planned for preoperative assessment, including education and informed consent of the patient. This consultation is conducted by the implanting physician and a dedicated nurse, guided by a ‘pre-assessment’ checklist (online supplemental figure 2). The operational elements of the referral review and pre-assessment are displayed in figure 1.
CRT-CPW changes related to implantation procedure focused on the structural collection of patient-related and implantation-related information, in order to be able to facilitate same-day discharge and availability of implantation-related information needed during follow-up. Hospital discharge was supported by a ‘pre-discharge’ checklist (online supplemental figure 3) which is introduced to verify the absence of implantation-related complications, medication verification, patient education and follow-up management planning. The operational CRT-CPW implantation phase is summarised in figure 2.
The CRT-CPW follow-up management consists of pre-planned visits from hospital discharge onwards, up to follow-up consultation at 6 months after implantation including echocardiographic evaluation. One-stop-shop consultations with pacemaker nurse/implantable cardioverter-defibrillator nurse and device technician at 1 to 2 weeks, and thereafter HF nurse and technician at 2 months and 6 months take place. The CRT-CPW did not include structured remote monitoring as an intervention, however this was offered as an option to patients in both usual care and CRT-CPW group. The device technician checks and if applicable changes device programming and reports on device HF diagnostics. The dedicated HF nurses act on device information, optimise HF medical regimen taking into account comorbidity affecting treatment and support the patient with medication compliance and lifestyle changes. All post implant consultations are guided by an ‘optimisation’ checklist (online supplemental figure 4). Whenever optimal conditions are not met, consequent actions are taken. In case specialist intervention is considered (eg, atrial fibrillation or His ablation), this is discussed in the multidisciplinary meeting. At 6 months the one-stop-shop consultation includes echocardiographic evaluation, and benefit from CRT is assessed accordingly. The CRT-CPW thus provides structured optimisation for every patient, instead of only those that do not respond to therapy as expected (so called ‘non-response’). Whenever a patient is thought to have improved too little from CRT, despite the structured optimisation, the patient is evaluated in the multidisciplinary meeting. The CRT-CPW allows for planning extra consultations if needed from a device or HF perspective with respective specialists and/or nurses. The operational CRT-CPW follow-up phase is displayed in figure 3.
CRT-CPW implementation
The CRT-CPW has been implemented at the MUMC+. A phased implementation strategy was used to introduce the CRT-CPW in functional parts of the care process; being the patient referral and pre-assessment, the implantation procedure and finally the follow-up management, as different stakeholders are involved in these steps. Between January and September 2014 all stakeholders were trained on the CRT-CPW, using the checklists provided and introducing logistical and IT (information technology) support changes to improve planning of consultations for the patients.
Patient and public involvement
This research was done without patient and public involvement.
Data collection and analysis
The study was performed according to the Declaration of Helsinki. Baseline characteristics and process metrics from all patients, from 6 months before the device intervention until 1 year after device implant were collected by extracting data from the MUMC+ (electronic) Hospital Information System. All patients that received care in the MUMC+ before and after the intervention, and had an elective ‘de novo’ CRT device implantation or upgrade to CRT were eligible for the study. Patients treated before the implementation of the CRT-CPW (January 2012 up to December 2014; usual care) were compared with patients treated after the implementation of the CRT-CPW (January 2015 up to December 2017).
Study outcomes
Process Key Performance Indicators were used as primary outcome measures. Process metrics were calculated for the period of 6 months prior to implantation of the CRT device, up to 12 months after the implantation of the CRT device.
Successful transition of care was measured by the number of physician and nurse and/or technician consultations, with specification of the specialism of the physician consulted. Resource utilisation was evaluated by number of consultations and number of outpatient visits (defined as consultations that are not on the same day). Moreover time from referral to CRT device implantation, the length of stay (LOS) in days after implantation and the total hospitalisation days during follow-up were evaluated.
Even though clinical outcome was not the primary focus of the current analyses we have used 12-month all-cause mortality and HF hospitalisations as a secondary outcome, to address the non-inferiority of quality of care.
Statistical analysis
Results are reported with means and SD for numeric variables and counts and percentages for categorical variables. Variables are compared using Student’s t-test or Wilcoxon rank-sum test for continuous variables, Fisher’s exact test for proportions, and the Cochran-Mantel-Haenszel test for trend in ordinal variables. A p value<0.05 is considered significant.
Results
Patient characteristics
In total 837 patients received a CRT device between January 2012 and December 2017 at the MUMC+. Of these patients, 531 were referred by external physicians, with incomplete follow-up data available for analysis. Sixty-one patients were non-elective implants, and hence data on pre-implantation care was missing. Additionally, eight patients were excluded because of missing data on the primary outcomes. The study cohort comprised a total of 237 patients available for analysis.
Data collected from 122 patients referred for elective implantation of a CRT device according to usual care and data from 115 patients after introduction of the CRT-CPW were analysed. The baseline characteristics of the two cohorts were largely comparable (table 1, Baseline characteristics). CRT-CPW Patients more frequently underwent an upgrade procedure (23.5 vs 12.3%, p=0.027) and more frequently had a history of myocardial infarction (47.8 vs 33.6%, p=0.034).
Baseline characteristics
Process metrics
Table 2 (Process metrics) summarises the process metrics for the usual care and CRT-CPW. Patients referred for a CRT device after CRT-CPW implementation had a comparable number of hospital visits to patients with usual care (10.1±4.3 vs 10.8±4.1, p=0.21). However, there were significantly more pre-implantation visits in the CRT-CPW cohort, than in the usual care cohort (1.6±1.4 vs 1.2±1.5, p=0.010). CRT-CPW visits included significantly more individual consultations than in the usual care cohort (9.9±4.2 vs 8.1±3.3, p<0.001). The number of consultations were significantly higher in the pre-implantation phase (2.1±1.8 vs 1.2±1.5, p<0.0001), and showed a trend toward significant increase in the post-implantation phase (7.8±3.7 vs 6.9±2.8, p=0.059) (table 2).
Process metrics
Patients in the CRT-CPW consulted HF nurses, pacemaker/ICD nurses and pacemaker/ICD technicians significantly more often than patients in the usual care cohort (2.4±1.5 vs 1.7±2.0, p<0.0001, 0.8±0.7 vs 0.0±0.3, p<0.0001 and 4.3±2.5 vs 3.7±1.5, p=0.063, respectively). At the same time patients with CRT-CPW consulted physicians significantly less often (1.7±1.4 vs 2.6±2.1, p<0.001) (table 2).
Time from referral to implantation of the CRT device was significantly reduced in the CRT-CPW cohort (23.6±18.4 vs 37.0±26.3 days, p=0.002). Total hospitalisation days during the observation period was significantly reduced in the patient group with CPW (2.4±4.8 vs 4.8±9.3, p<0.0001). This reduction includes a significant reduction in LOS at implantation (1.1±1.2 vs 1.5±0.7 days, p<0.0001), with a significant increase in patients with a same-day discharge and with only one night stay at implantation (28 vs 7% and 78 vs 43%, respectively, both p<0.0001) (table 2).
Clinical outcomes
Table 3 (Clinical outcomes) summarises the clinical outcomes for the usual care and CRT-CPW at 12 months follow-up. Patients referred for a CRT device after CRT-CPW implementation were hospitalised for HF less often than patients referred for a CRT device before its implementation (5.2% vs 9.0%, p=0.32). Also patients 12-month mortality was (non-significantly) lower when patients were implanted with a CRT device after CRT-CPW implementation (3.5% vs 6.6%, p=0.38) (table 3).
Clinical outcomes
Discussion
Implementing a CRT-CPW using multidisciplinary care, in a structured, checklist driven patient management protocol resulted in a successful transition of physician-led usual care to nurse-led CRT patient management. Moreover it led to a significant reduction in resource use; with a reduction in hospitalisation days and physician consultations. These changes did not lead to inferior clinical outcomes, as mortality and HF hospitalisation at 12 months were non-inferior to usual care.
Mullens et al were the first to show that the use of a standardised algorithm in patients that did not derive benefit from CRT could identify factors associated with suboptimal treatment, and if corrected this was associated with improved clinical outcome.14 Importantly, these favourable effects appeared to be driven not only by appropriate device and arrhythmia management but also by improved HF care.22 These results were recently strengthened by another study comparing multidisciplinary, comprehensive CRT care to conventional CRT care.12 A communal factor in the programmes evaluated in these studies however, is that they require intensive, specialised, physician guided follow-up, with extensive resource use, which hampers widespread adoption in clinical practice.
The CRT-CPW as applied at the MUMC+ shared the aim to improve quality of care for patients with CRT by applying multidisciplinary expertise, in a structured way in order to identify any opportunity for optimisation of treatment at any moment in the care process. But at the same time, the current CPW aimed to establish a transition of care from highly specialised (physicians-led) care to protocolled, nurse-led care, with structured planning of patient visits to establish a reduction in resource use.
The current study showed that a transition was made from physician-based care to the nurse-led program. Non-dedicated physician-led care, incorporating different kind of specialised cardiologists was transferred to the CRT-CPW nurse-led care. The evaluation showed that there still were physician contributions to the HF care in the patient with CRT-CPW group. This may be explained by destabilised HF which demanded physician consultation, specialised consultation in order to target factors contributing to suboptimal treatment or simply incomplete implementation of the CRT-CPW. In addition, implementation of the new CRT-CPW may have been incomplete as simultaneous and complete training of all contributors to CRT care before the start of the practical use of the CRT-CPW was not possible. As implementation of new CPWs expands over time, especially when contributors see the added value of it, we expect the number of physician consultations to decrease further over time. However, as specialised interventions (eg, atrial fibrillation or His ablation procedures) may be required in structured optimisation, physician consultations will remain at a minimal level needed to reassure optimal CRT care.
Even though we successfully transferred care for these patients to dedicated CRT and HF nurses and technicians, the number of visits was not significantly lower in the CRT-CPW cohort. Due to the uncoordinated care in the usual care cohort, we expected this to be lower in the CRT-CPW group. Our data shows that the introduction of the one-stop-shop visits in the CRT-CPW resulted in a reduced need for repetitive visits, as the overall number of consultations significantly increased in the CRT-CPW, but patient visits to the outpatient clinic were not different. This is possible as the pathway allowed for deviations when either optimisation or stabilisation of HF required this. One explanation may therefore be that in the checklist driven CRT-CPW more possibilities for optimisation were identified, requiring extra consultations, for example, optimisation of HF medication, treatment of congestion or device reprogramming. Another explanation may be an increase in destabilised HF, however if the excess consultation would have been the result of this, we would expect to have seen a coinciding increase in HF hospitalisations and overall hospitalisation days during follow-up. Other studies introducing structured checklist into general HF care have shown that restructuring HF care, aided by checklists helped to improve guideline adherence for the outpatient and admitted HF population, respectively,20 21 therefore we believe that future evaluations will reflect this in improved patient outcomes.
Another result of the enhanced coordination and planning by the multidisciplinary team is the reduced time between referral and device implantation, with more than 35% reduction. Shorter time to any intervention generally contributes greatly to patient satisfaction with their medical treatment.23 Moreover, in patients with HF, timely intervention may prevent hospitalisation due to destabilised HF. With the use of a ‘referral’ review and ‘pre-assessment’ checklists incomplete diagnostic work-up or lack of general HF optimisation can be identified at referral and managed in a coordinated way. Moreover, the reduction in device-implantation related LOS was possible due to (1) discussion of and consent to a discharge plan with the patient at the pre-implantation one-stop-shop meeting, and (2) the introduction of a discharge checklist, available to the ward nurse to reassure absence of any complications, enabling an early discharge.
Finally, the current evaluation showed a non-significant decrease in all-cause mortality and HF hospitalisation. Even though this was not the primary aim of the current evaluation, these results express the non-inferiority of the nurse-led, checklist-guided, CRT-CPW compared with usual care with respect to clinical outcomes. As the selected cohort of patients analysed in the current paper specifically fits the primary aim of process evaluation it does not allow to show superiority on clinical outcomes. Reduced mortality and HF hospitalisations (even though non-significantly) may point to an improved clinical outcome, as reduction of HF hospitalisation is one of the main targets in HF management. Moreover, hospitalisations remain the largest expense in HF care,24 and a reduction may lead to a significant reduction in healthcare costs. Efforts are currently being made to evaluate relevant medical outcomes and costs, in order to report on cost-effectivity of the CRT-CPW.
Strengths and future: This CRT-CPW allows for adjustments to local practices and hospital care teams, while still providing quality care for patients with CRT by making use of standardised forms and algorithms. Further improvement of data collection by automatic data entry into the hospital information system combined with integration of the CRT-CPW into standard medical practice will provide a unique opportunity to standardise and continuously evaluate patient care. This potential may lead to continuous improvement of quality of care, resource use and innovation in CRT care.
Limitations: This study uses a historical control to evaluate the CRT-CPW effect on process metrics, this introduces a possible bias. Other influences on process outcomes may have been introduced over time, affecting the results. Furthermore, even though the pathway aims to be simple and adoptable to any clinical practice, it is uncertain whether the presented results will be similar in other centres. Other hospitals have started to implement the CRT-CPW, which provides opportunities for future evaluations. A limited number of patients were included in both cohorts, patients referred from other hospitals and hospitalised patients were excluded because of incomplete follow-up. Next to patient clinical outcomes, patient satisfaction with the care pathway have not been addressed in the current paper. However it may be expected that patients appreciate the reduced time to treatment, improved communication between stakeholders and the efficient care team interaction.
Conclusion
The introduction of a CRT-CPW using a protocolled, multidisciplinary approach with structured aids, led to a successful transition of physician-led care to nurse-led care, with a significant reduction in hospital resource use, and non-inferior clinical outcomes, compared with usual care.
Acknowledgments
We would like to thank Archana Rao (Cardiology Department, Liverpool Heart and Chest Hospital, Liverpool, UK, RegitzeVidebaek and Helen H Petersen (Cardiology Department, Rigshospitalet, Copenhagen, Denmark), John M Morgan (Cardiology Department, Wessex Cardiac Centre, Southampton University Hospitals, Southampton, UK), Wilfried Mullens (Cardiology Department, Ziekenhuis Oost-Limburg, Genk, Belgium) for the input and discussions resulting in the structured CRT-CPW. Luuk Debie and Josiane Boyne (MUMC+) for the implementation and completion of the patient checklists, Bart Gerritse, Richard Cornelussen and Sandra Jacobs for the data analysis (BG), comments, suggestions and edits to the manuscript (BG, RC, SJ, Medtronic plc).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AMWvS and SS are joint first authors.
Contributors AVS, WD, HP B-LR, CK, KV: contributed significantly to the concept, design of the CRT-CPW, the implementation of the CRT-CPW; the data acquisition, analysis, interpretation of data for the work and writing of the manuscript. SS: contributed to the implementation of the CRT-CPW, data acquisition, analysis, interpretation of data and writing of the manuscript.
Funding This project was funded by a research grant from Medtronic plc.
Competing interests AVS, WD, CK and KV have nothing to disclose; SS is employee of Medtronic and HP B-lR reports grants from Vifor, Novartis and Roche Diagnostics, outside the submitted work.
Patient consent for publication Not required.
Ethics approval The study was approved by the Medical Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data were made available from the Hospital Administration System for this study and are not publicly available.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.