Article Text

Abstract
We report our experience in using virtual technology in our emergency department (ED) to meet communication needs of our patients who have limited English proficiency (LEP) during the COVID-19 pandemic. Our project aim was to improve communication between our ED staff and patients who have LEP. Specifically, our primary aim was to eliminate the use of healthcare staff as ad hoc interpreters by 50% in our ED by using virtual medical interpreters within 2 months. To achieve our goal, several strategies were employed. First, we assessed the need for interpreters in our ED by tracking the number of times our nursing staff is pulled away from their nursing role to help other staff as an ad hoc interpreter. Second, a patient survey was conducted to understand their thoughts and needs for interpretation in the ED. Third, we developed strategies in improving access to interpreters in our ED. During the COVID-19 pandemic, we conducted a trial of using ‘Interpreter on Wheels’ (IOW) in our ED. In a 2-month period, we had 477 virtual interpretation encounters totaling 4123 interpretation minutes of IOW usage. We found that it satisfied not only our communication needs but also reduced some of our potential infection control risks during the pandemic.
- quality improvement
- emergency department
- health equity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Our hospital setting is a university-affiliated community teaching hospital located in Richmond, British Columbia, Canada. It has annual emergency visits of approximately 60 000. We serve a culturally diverse population—76% belong to a visible minority group with more than half speaking Mandarin or Cantonese.1 Furthermore, our hospital is the nearest hospital to an international airport serving over 25 million passengers from over 100 countries annually.2 As a result, we frequently encounter patients who have limited English proficiency (LEP) with interpretation needs.
Our lack of a dedicated emergency department (ED) interpreter causes communication gaps between healthcare providers and patients resulting in unnecessary increases in length of stay or poor clinical outcomes. Occasionally, patients bring their family members or friends to the hospital for interpretation. This arrangement is often unreliable in terms of accuracy of the interpretation and also not ideal for sensitive discussions or privacy. Frequently, we resort to using other staff in our hospital for interpretation, taking them away from their clinical duties, thus wasting valuable healthcare personnel resources.
The original plan was to hire an on-site interpreter, dedicated to the ED, who speaks Mandarin and Cantonese for our needs. However, during the COVID-19 pandemic, the plan of using an on-site interpreter was rejected and the feasibility of continuing with patients’ family members or staff was diminished due to infection control concerns.
Background
It is well documented that language barriers impact healthcare in the ED setting. Patients who have LEP often have difficulty communicating with healthcare providers which can lead to poorer health outcomes. Patients who have LEP often have longer lengths of stay in the ED, undergo more tests due to diagnostic uncertainty and have higher rates of admission.3 In one study from 2016, patients who have LEP were 24% more likely to have an unplanned ED revisit within 72 hours suggesting challenges in ED quality of care.4
Ad hoc interpreters are often used when a professional interpreter is not readily available. Family members or friends who accompany patients who have LEP often act as interpreters. This is not ideal because family members and friends may not have the expertise to accurately translate medical terms and diagnoses. Furthermore, conversations are often sensitive and confidential in nature and thus make family members and friends not the ideal person to be the interpreter. ED nursing staff with proficiency in a second language are frequently asked to provide interpretation. This takes them away from their assigned tasks, increases workload and reduces efficiency and flow in the ED. There can also be missed or misinterpreted information with subsequent perceived clinical risk.5
It is widely accepted that the use of professional interpreters for communication with patients who have LEP in the healthcare setting provides many benefits. These benefits include an improvement in patient comprehension, improved clinical outcomes and increased satisfaction with care.6 Professional interpreters are also associated with more accurate discharge communication leading to improved safety and outcomes particularly for paediatric patients who have LEP and were discharged from the ED.7 Furthermore, the use of professional interpreters results in significantly lower likelihood of errors than ad hoc or no interpreters.8
Various solutions currently exist to provide professional interpreters in the healthcare setting. Interpreters may be accessible remotely by telephone, or video, or live in-person. While these modalities have various advantages and disadvantages, the best modality may differ depending on the clinical setting, population served and available resources. Access to multiple interpretation options are often necessary to provide proper and culturally competent care for patients.9 In most healthcare settings, the modality used is dependent on what is most easily accessible to clinicians.
The patient population in Richmond, British Columbia, is unique due to the large number of non-English native speakers in our community. Only 33% of residents based on the 2016 census reported their mother tongue as English.1 The majority of patients who have LEP require Mandarin or Cantonese interpretation. At our ED, interpretation has traditionally been provided by ad hoc interpreters such as family members, friends or ED staff. Remote telephone interpretation has had limited uptake due to inconvenience of use and poor sound quality, while access to an in-person professional Mandarin and Cantonese interpreter is limited.
The COVID-19 pandemic added another challenge to providing care for patients who have LEP. As with other jurisdictions, our health authority restricted all visitors to essential visits only, meaning only in cases of compassionate care such as end of life or critical illness. Patients who usually would have family or friend accompanying them to help interpret were no longer present to provide this service. As well, to mitigate risk of infectious contamination, contact between patients, live in-person interpreters and other healthcare personnel who would otherwise assist with interpretation was kept to a minimum. These additional restrictions limited our ability to provide in-person professional or ad hoc interpretation.
The ‘Interpreter on Wheels’ (IOW), a mobile device providing access to voice and video translation in over 200 languages, was a practical solution in this unique situation. This project provided an opportunity to trial a new technology to provide professional interpreter services 24/7 in an ED servicing a high number of patients who have LEP while adhering to infection control precautions.
Measurement
The goal of this quality improvement project is to improve communication between our staff and patients who have LEP by having a dedicated interpretation service in our ED. Specifically, our primary aim was to eliminate the use of healthcare staff as ad hoc interpreters by 50% in our ED by the introduction of virtual medical interpreters within 2 months.
Before the COVID-19 pandemic, we were able to collect baseline data on the number of times nursing staff was pulled away from nursing duty to provide interpretation for other staff members. Furthermore, we conducted a patient survey to understand their needs for interpretation service in our department.
During the trial of using ‘IOW’ in our ED, patients and staff had the option of rating their experience on the device electronically. Data were also collected on the number of interpretation encounters and the number of interpretation minutes.
Baseline measurement
Misuse of personnel resources
Baseline data were collected to understand the experiences of bilingual nurses as ad hoc interpreters in our ED. Between 18 July and 11 August 2019, we asked four emergency registered nurses (RN) who speak Mandarin and Cantonese to record the start and end time of when they were pulled away from their nursing role to provide interpretation for other colleagues. During the 25 days period, there were 49 times when they were pulled away in 18 RN shifts with an average of 12.8 min per encounter. This represents 34.8 min per shift per RN when there is misuse of healthcare personnel resources.
Patient survey
A patient survey was conducted to understand the needs of patients using interpreting services. Seventeen native Chinese (either Cantonese or Mandarin) speaking patients were interviewed in the ED. Overall, 76% of the patients understood less than half of the medical content discussed. Overall, 94% of patients would choose to use interpretation services if available.
Design
Our primary aim was to eliminate the use of healthcare staff as ad hoc interpreters by 50% in our ED by the introduction of virtual medical interpreters within 2 months. This project used a collaborative approach to design our quality improvement (QI) intervention. It was supported by a physician-led quality improvement team and a team-based quality improvement committee at our health authority. It went through A pRoject Ethics Community Consensus Initiative and was reviewed by our health authority privacy review committee.
After obtaining baseline measurements to understand patient and staff needs and requirements, our first intervention was to increase awareness of the project idea in order to improve the experience of patients who have LEP and improve the satisfaction of our staff. The results obtained from our baseline work and patient survey results were disseminated and shared at staff meetings of our ED. Our improvement idea was also discussed and shared at the hospital quality council meetings attended by frontline and administration staff to further increase awareness and support of the project.
Our original plan was to compare different modes of professional healthcare interpretation in their ability to achieve our primary aim. We wanted to evaluate whether virtual interpretation and/or in-person interpretation could eliminate the need for staff to provide ad hoc interpretation. We intended to repeat misuse of personnel resources measurements. Furthermore, we intended to conduct patient and staff surveys to study other benefits and counterbalances of the two interpretation modalities. Our trial was to start on 31 March 2020. However, because of the COVID-19 pandemic, our health authority forbade the introduction of our live in-person interpreter to our ED due to infection risk. In addition, all survey collection and data gathering were prohibited.
Despite our inability to introduce in-person interpreter or actively collect data, we felt there was benefit to conduct a limited trial of virtual interpretation in our ED during the COVID-19 pandemic. We modified our project by only introducing virtual interpretation and collect only passive data from the virtual device. This modification received approval from hospital administration. Funding was provided through our hospital health authority, our provincial physician association and the hospital foundation.
We used ‘IOW’ through the LanguageLine InSight Audio and Video Interpreting Service (figure 1). IOW comes in the form an electronic tablet mounted on an adjustable rolling stand within a secure audio amplification system. Interpretation is initiated through a touch screen app. Interpretation service is available 24/7 with access to over 200 languages through video or audio form.
Interpreter on Wheels.
Strategy and results
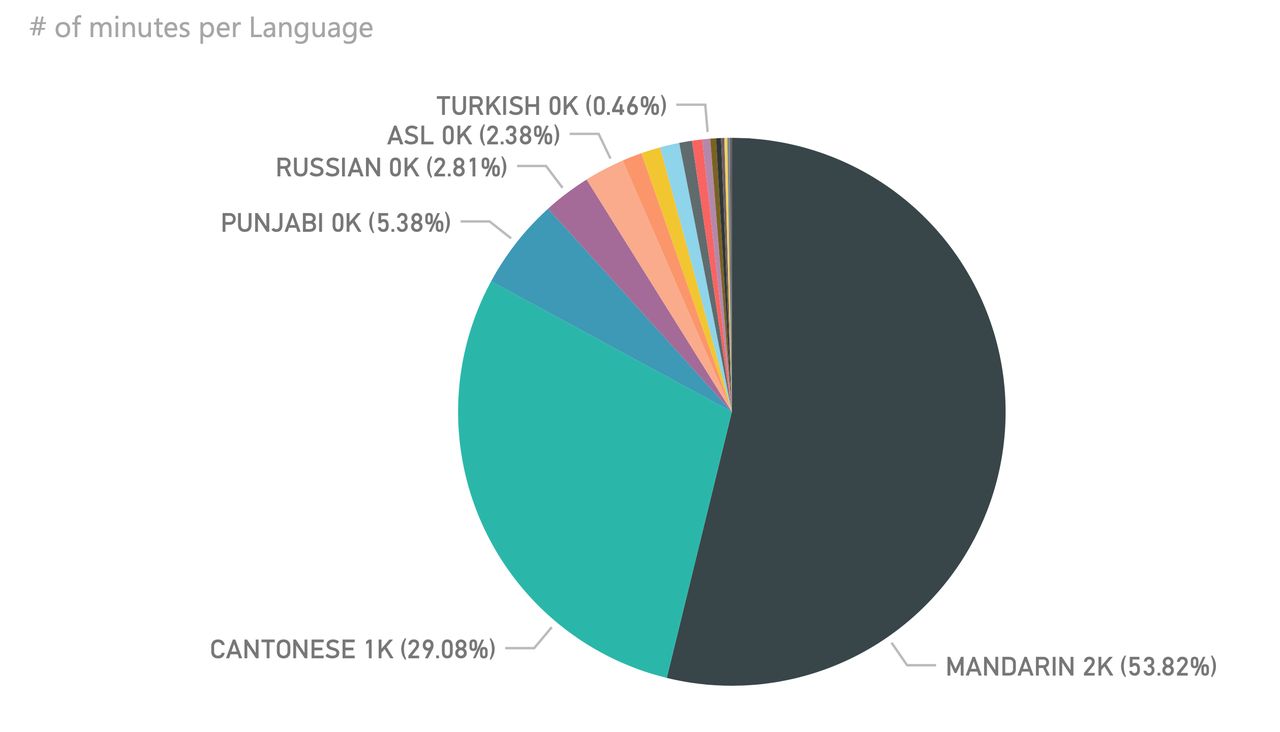
Between 30 March and 31 May 2020, we had 477 virtual interpretation encounters totaling 4123 interpretation minutes (2835 audio minutes and 1288 video minutes) of IOW usage. The majority of the interpretation needs were for Mandarin or Cantonese (figure 2). The feedback was extremely positive both from the staff and the patients. A composite score of 4.43/5 was received from 169 on-device ratings. Anecdotally, it was deemed that the IOW provided a safe and reliable interpretation resource for our ED. Especially during the COVID-19 pandemic, we found that it was safer from an infection control perspective to interpret electronically to meet demands of physical distancing and isolation. Stories of IOW usefulness include:
A deaf gentleman presented with hip pain. He had his note pad and pen ready to write notes to the staff. He was pleasantly surprised that we were able to access an American Sign Language video interpreter within seconds. We were able to take an accurate history, guide him through focused physical exam, provide discharge instructions and answer his questions. It was very easy and efficient, and we were confident that we were able to help address his medical concerns.
The IOW was used to assist in a sensitive conversation with a patient and her family regarding code status/level of intervention. The translator was able to convey the critical nature of the clinical situation using medical and technical terms in Cantonese. We were able to clearly establish goals of care and discuss prognosis. The patient’s family was very appreciative to have a clear understanding of the situation.
A gentleman presented with anxiety and insomnia. He spoke only Mandarin. Using the IOW, we were able to have a detailed conversation to understand his concerns both physical and psychological. The complexity of the situation required multiple separate conversations using the IOW. In the end, an adequate plan was arranged for outpatient mental health follow-up.
{kind=link}
{kind=link}
Languages used between 30 March and 31 May 2020. Note: ASL=American Sign Language
Lessons and limitations
Lessons learnt within our Access to Translator (AT&T) project included navigating the balance between introducing a new IOW technology during a time when new clinical processes and procedures were being rolled out daily during the COVID-19 pandemic. The project required administrative approval to roll out and was initially delayed during the early weeks of the pandemic as more urgent matters took precedent. Within our health authority, visitor policies limited patient’s family members to essential visits only, such as end of life care and critical care decision-making. Our QI team noted this and advocated the importance of the project to move ahead. We reasoned that the IOW would provide patients and staff with effective and safe interpretation services in the absence of patient family members. Furthermore, IOW prevents misusing ED staff as ad hoc interpreters so that they can concentrate on their clinical care responsibilities. This also limits the number of unnecessary physical contact from the hospital staff doing ad hoc interpretations with patients who may have infectious concerns. The project was eventually approved in midst of the COVID-19 pandemic.
The device was immediately well received and had little negative feedback. On a few occasions, error messages would display, resulting in the need to reboot the device which resolved the issue. The device was user friendly and it brought an interpreter to the clinical assessment area promptly. We found it was used by more ED team members than previously expected, including consulting physicians, social workers, admitting clerks, respiratory therapists and pharmacy technicians completing medication reconciliations. We have received feedback asking for a second device in the department, as physicians and nurses report walking around looking for it, and finding it in use already, requiring them to wait for their turn to use the device. When patients were discharged home, pending infection tests results, the staff used the device to educate the patients how to properly isolate at home in addition to providing translated written handouts.
We also found that the cost of the device was not insignificant. There were separate fees for audio and video interpretations. The audio interpretation fee is $C0.90/min, while the video interpretation fee is $C1.60/min. While the staff were directed to choose the less costly audio option when possible, the monthly cost for the device was not insignificant. However, using the IOW eliminated the potential cost related to personal protective equipment usage from on-site professional or ad hoc interpreters. Furthermore, one has to evaluate the potential economic impact of disease spread due to physical interaction with patients with infectious concerns.
Limitations to our AT&T project included the lack of ability to collect qualitative and quantitative measurements of the multidisciplinary team’s experiences using the device, since the project was rolled out during the pandemic where resources were concentrated on other priorities and there were infection control concerns. While the metrics and numerical values of minutes used and languages accessed was tracked, there was less ability to compare the device with in-person interpreters as originally planned, which may have given some understanding of staff preference for interpretation in the ED. Despite our inability to repeat assessment of ad hoc interpretation by ED staff, the IOW was used 477 times during a 2-month period and it very likely reduced the need for personnel misuse in our ED.
Conclusions
We report our experience using virtual technology in our ED to meet communication needs of our patients who have LEP during the COVID-19 pandemic. During the COVID-19 pandemic, we conducted a trial of using ‘IOW’ in our ED. We found that it satisfied not only our communication needs but also mitigated some of the infection control concerns in our ED. We are working closely with hospital administration to provide funding for this resource long term.
Acknowledgments
The authors would like to acknowledge Vancouver Coastal Health Quality Improvement Teams (PLQI and TBQI), Vancouver Coastal Health Virtual Health Team and British Columbia Provincial Language Service for their support.
Footnotes
Twitter @kwok_matthew
Contributors MK: Overall leadership of the project and article writing and editing. RKC: Assisted in the project and article writing and editing. CH: Assisted in the project and article writing and editing. KT: Assisted in the project and article editing. HYW: Assisted in the project and article editing.
Funding The authors received funding for their work from Vancouver Coastal Health Authority, Doctors of BC and Richmond Hospital Foundation.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.