Article Text

Abstract
Epidurals are a useful perioperative procedure for effective analgesia that allow early mobilisation after major surgery and help to minimise postoperative pulmonary, cardiovascular and thromboembolic complications. However, there are potential rare but life-changing complications such as an epidural haematoma. These require a high standard of post-epidural care for prompt recognition and prevention of permanent paralysis. Following a local critical incident of delayed diagnosis of an epidural haematoma in a patient after epidural catheter removal, a multidisciplinary team undertook a Quality Improvement (QI) project to improve epidural safety. To achieve this aim, it is essential that healthcare staff are aware of the early signs of neurological complications during and after epidurals and of what action to take in the event of a developing complication. The application of robust QI methodology has contributed to a sustained improvement in the healthcare staff competence (as measured using a pulse survey) at managing patients who have received perioperative epidurals. This increased from a baseline mean survey score of 38% on three surgical step down wards (general surgery, vascular and gynaecology) to 68% (averaged over the most recent 3 months of the project time frame). Educational interventions alone rarely lead to meaningful and lasting impact for all healthcare staff, due to high turnover of staff and shift working patterns. However, with multiple plan, do, study, act cycles, and a robust QI approach, there was also sustained improvement in process measures, including the occurrence of written handover from high dependency to the step down wards (baseline 33%–71%), ensuring the application of yellow epidural alert wristbands to make these patients readily identifiable (56%–86%), and early signs in improvement in reliability of motor block checks for 24 hours’ post-catheter removal (47%–69%).
- adverse events
- epidemiology and detection
- patient safety
- anaesthesia
- surgery
- critical care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Epidurals have advantages in providing effective analgesia and minimising post-operative pulmonary, cardiovascular and thromboembolic complications.1 ,2 ,3 The serious complications of an epidural are rare but life-changing, and rely on prompt recognition to prevent permanent paralysis.4–7 The incidence of epidural haematoma is more frequent than previously thought in the target population of perioperative non-obstetric patients,5–9 and it may be as high as 1 in ~9000. This risk may be increased due to peri-operative anti-platelet and anti-coagulation medications, and the potential for deviation from safety guidelines in their administration timing.7 A local hospital critical incident of delay to diagnosis of an epidural haematoma in a patient after epidural catheter removal has led to this Quality Improvement (QI) project to improve epidural safety. It is important for healthcare staff to be able to readily identify which patients have received epidurals and understand the significance of the onset of specific new symptoms in the context of a recent epidural catheter. An epidural haematoma typically presents with back pain, progressive lower limb sensorimotor deficit and sphincter dysfunction. The most reliable sign of a developing haematoma is motor block, because other factors, such as bladder catheterisation and high incidence of postoperative constipation, mean it is difficult to assess sphincter dysfunction.4 The symptom onset is usually 24 hours following either epidural insertion or removal, but this can also be delayed.6 7 10 11 Therefore, the same high standard of epidural care needs to continue from insertion, to removal, through to the patient’s discharge. This allows the early identification of epidural complications and prompt interventions to prevent paralysis.
The project aim was to improve the standard of care for patients who had received perioperative non-obstetric epidural analgesia during their hospital admission. It focused on their care after they had been stepped down to any one of three main surgical wards. It is the hospital policy that the epidural infusions are discontinued when the patient goes to the level 0 surgical wards from high dependency or intensive care. The catheters can still be present but in most instances are removed from the patient, often immediately prior to step down. When the catheter is still present, it is often due to deranged coagulation preventing its removal. In practical terms, the authors determined that the following baseline knowledge is necessary in order for the multidisciplinary (MDT) ward teams to safely look after these patients:
Which patients in their care had epidural catheters in situ or recently removed.
That a time interval must be observed between epidural catheter removal and the delivery of anticoagulation.
Motor block checks should be performed every 4 hours for the first 24 hours after epidural catheter removal.
The significance of a patient developing inappropriately weak leg(s), or other neurological sequelae, in the context of a patient having had a perioperative epidural.
To have an awareness of the immediate escalation policy of concerns to the on-call pain service or anaesthetics on-call team.
The target was to create a sustained improvement in the healthcare staff competence at managing patients who had received perioperative epidurals from the baseline of 38% to greater than 60% in 6 months across three surgical wards.
Background
An epidural haematoma is a rare but potentially devastating complication of neuraxial procedures. The authors of the third National Audit Project5 attribute the failure to identify and understand the relevance of inappropriately weak legs after central neuraxial blockade as leading to avoidable harm. It is difficult to collect evidence for rare complications on which to base UK-wide recommendations for practice, however, it is emerging that epidural haematomas and other complications are far more frequent in non-obstetric perioperative epidurals.5–9 Most studies correlate better neurological recovery in those patients with a shorter interval from symptom onset to surgical management.6 10–12 Symptom onset is most commonly 24 hours around removal of the epidural,3 but it can also occur around insertion, or the onset can be delayed.7 10 11 Immediate recognition and escalation of this complication to prevent permanent harm relies on interpreting these new symptoms in the context of a recent epidural. This requires MDT staff being able to readily identify those patients who have received an epidural and for them to have appropriate training surrounding epidural care even on the downstream wards when the epidural catheter has potentially already been removed. Staff need to understand what signs and symptoms to look out for, and what actions to take in the event of a developing complication. National surveys of neuraxial procedures in the UK support vigilance for complications of epidurals in the period following removal. There is support for inexpensive measures such as 24 hours of motor block checks every 4 hours after catheter removal,4 which were already local hospital policy.
There is an increase in neuraxial bleeding complications with the concurrent administration of low-molecular-weight heparins for thromboprophylaxis.13 14 This has led to the recommendation that a time interval of 4–6 hours is observed after catheter removal before heparin administration for thromboprophylaxis.13 14 It is integral to the postoperative care of epidurals that medical and nursing staff are aware they need to alter the timing of medications for routine thromboprophylaxis after epidural removal.
Measurement
Data were collected on randomly selected days, two times per month on three surgical wards between November 2018 and May 2019 in a large tertiary referral centre in Edinburgh, South East Scotland, by three separate investigators. Data collection comprised a pulse survey of MDT ward staff who were available at the time of data collection (including doctors-in-training at all levels and nursing staff at multiple bands) review of all patient notes who had been stepped down to these wards having received perioperative epidural analgesia, and direct observation of these patients. The three surgical wards (general surgery, vascular and gynaecology) receive the majority of step-down patients from high dependency or intensive care who have received perioperative epidurals during their hospital admission. Inclusions were all inpatients on data collection days on all three surgical wards, who had non-obstetric perioperative epidurals during this hospital admission.
The outcome measure was competence of the healthcare staff at managing patients who have received epidurals, measured using a pulse survey with a maximum score of 5. Prior to commencement of data collection, the investigating team established the minimum responses required for a score of 1 to each question, and the results were moderated by all three investigators independently reviewing the results of each individual survey.
Are you looking after a patient today who has had an epidural at any point during their hospital stay? (If correctly answered no, score 1. If correctly answered yes, move onto question 2.)
If yes to above, who? (If patient(s) correctly identified, score 1.)
Are there any specific actions to take when looking after a patient who has had an epidural recently removed? (Score 1 for stating motor block checks OR delay to anticoagulation administration, score 2 for both.)
Are there are complications that you would look out for in a patient who has had an epidural? (Score 1 for leg weakness, urinary retention, back pain, local swelling, redness or other signs/symptoms of epidural complication.)
What would you do if you were worried about a patient who had had an epidural? (Score 1 for correct escalation policy.)
The number of staff surveyed during each data collection day varied according to staff availability at the time of data collection, from n=2 to n=14. Results from each data collection episode were aggregated and are presented as a percentage score.
There were three process measures:
First, whether the patient had a yellow epidural alert wristband in place on step down to the surgical wards. This would readily allow the identification of patients who had received an epidural during their hospital admission. It also had the bleep number for the acute pain service and anaesthetics team on-call. It included the date and time of the insertion and removal of the epidural catheter. These data were collected by direct observation of all patients within the ward areas who had received perioperative epidurals, which varied according to the surgical workload in the time preceding each data collection episode. Data are presented as a percentage compliance for each collection episode.
Second, presence of appropriate documentation of handover of information regarding the patient’s perioperative epidural. This was measured by investigator assessment of all electronic and paper documentation for every patient who had received an elective perioperative epidural during their hospital admission and was present on the target ward during each data collection episode. ‘Appropriate’ documentation was deemed as written information of the date and time of epidural catheter removal and is presented as a percentage aggregate for each data collection episode.
Third, whether there was appropriate documentation of an assessment of motor strength being performed every 4 hours for 24 hours’ post-removal of the epidural catheter as required by the local hospital policy.
Baseline data
A large initial baseline data set of 42 pulse surveys of staff and observation and notes review of 18 patients who had received perioperative epidurals was collected in November 2018 prior to instituting any interventions. The outcome measure survey data were collected during six separate data collection episodes. These were used to set the median line of the run chart for outcome measure. The initial baseline process measures data were collected over two separate data collection episodes. Due to having aggregated these data into two data points, the process measure run charts show a median line calculated from all data presented.
These baseline data showed that the aggregated mean pulse survey score, testing knowledge required for competence in managing patients who have received perioperative epidurals, was 38%. An epidural alert wristband was present in 56% of instances, a handover that contained appropriate information relating to the patients’ epidural was present in 33% and mean compliance with gold standard motor block checks was 47%. The investigators felt that there was room for improvement in all of these key areas.
Following this initial data collection, informal interviews were conducted with key stakeholders, including the hospital acute pain management service and multidisciplinary ward leaders on the target wards and the data were presented at local anaesthesia departmental meeting. These discussions helped to raise the profile of the QI project, clarify the aims and expectations with those teams involved, and guided the QI investigators as to which tests of change might be most impactful.
There was no patient or public involvement because it was not feasible to involve them in the design of the project.
Design
The project was registered with and had approval from the local QI lead.
The project team consisted of anaesthetic trainees and consultants who worked with MDTs including the Acute Pain Team, the South East Scotland Quality Improvement and Audit and Research Network, Anaesthetics, Critical Care and MDT ward teams across the three main surgical wards. These three wards received all step-down patients with a perioperative epidural during the data collection period.
The baseline data collected in November 2018 supported the need for the following interventions:
Education via informal micro-teaching about the care of patients with epidurals. This was delivered throughout the 6-month project time frame, in addition to formal teaching on the topic delivered to doctors-in-training at their weekly mandatory lunchtime teaching sessions. Anyone who completed a survey as part of the data collection also had the opportunity to ask questions at the end of the survey and receive a session of micro-teaching. This bundle of educational interventions assisted in bridging the knowledge gap in the multidisciplinary healthcare staff regarding epidurals.
The introduction of electronic written nurse-led discharges from high dependency and epidural care awareness campaign. It was predicted that this would improve communication between high dependency and level 0 wards, and help to standardise the location of written information regarding epidurals. This would enable ward staff to more easily know which patients had received an epidural during this hospital admission, as well as salient information surrounding timings of epidural removal.
Increase the compliance with yellow epidural alert wristbands to make these patients readily identifiable. This was done with an epidural care awareness campaign that included posters in all relevant areas (for example, main recovery, gynaecology recovery, high dependency and intensive care), communication to the relevant team leaders and presentation at departmental meeting.
The trial of a motor block sticker to encourage staff to perform motor block checks on the surgical wards at appropriate intervals in the immediate 24 hours following removal of the epidural catheter.
Strategy
Throughout the project timeline, there was formal and informal education to ward staff regarding epidurals. Informal micro-teaching was delivered several times a month to ensure uptake by a good proportion of the ward teams. The project used three PDSA (plan, do, study, act) cycles, each of which contained a bundle of interventions aimed at each of the three process measures.
During PDSA cycle 1 January–February 2019, the aim was predominantly to improve compliance with appropriate written handover information. This included the introduction of electronic, standardised, nurse-led discharge from high dependency to step-down wards. During this cycle, formal teaching sessions were delivered to doctors in training at mandatory teaching sessions.
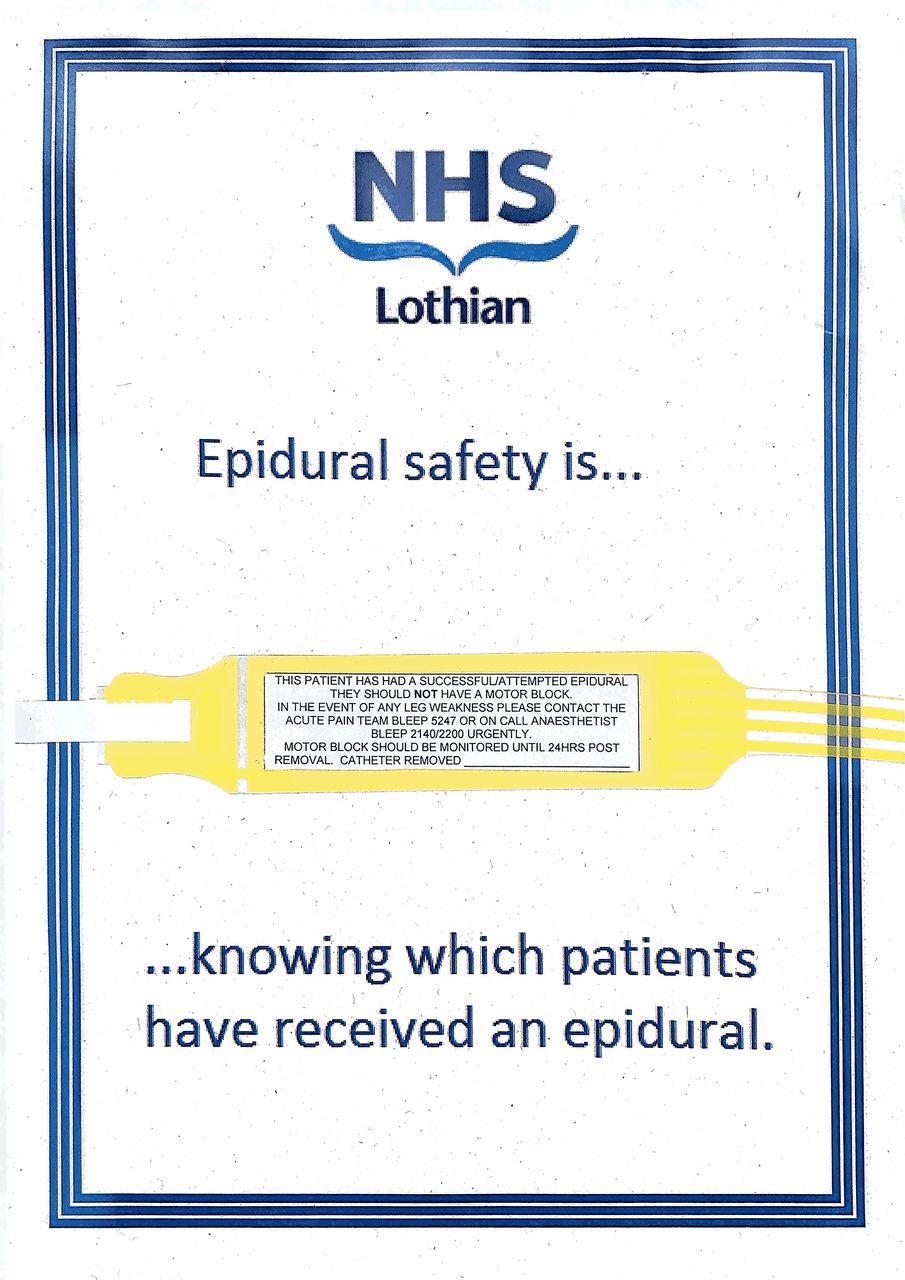
During PDSA cycle 2 February–March 2019, the goal was predominantly to improve compliance in patients wearing epidural alert wristbands. The investigators instituted a widespread epidural safety awareness campaign. This included posters to promote the use of epidural alert wristbands in main recovery, gynaecology recovery, high dependency and intensive care (figure 1). Verbal and email communications with team leads allowed this information to be included in local daily ward morning safety huddles, and the investigators ensure spare wristbands were available in every clinical area in case of inadvertent removal.

Poster to improve epidural safety by promoting the epidural alert wristbands and ease of patient identification.
During PDSA cycle 3 March–April 2019, the aim was to improve compliance with motor block checks. The investigators introduced motor block check stickers. These were designed to encourage block checks at the correct time intervals and for the correct period of time in total. These factors had been identified as a weakness in the initial data collection, and during the informal project discussions with key stakeholders at ward level.
Results
Following introduction of the first test of change, throughout the 6 months of QI work presented here, the survey testing, the outcome measure was undertaken on 46 occasions. Twenty-five patients and their notes were objectively examined by the investigating team. Two patients were notably excluded from the data presented, for reasons of patient safety that support the rationale behind the project. One patient was stepped down to the ward with their epidural catheter in situ due to deranged coagulation. The ward staff did not know that the epidural catheter was in situ due to a lack of handover and the patient was not wearing an epidural alert wristband. Furthermore, the ward staff had already administered low-molecular-weight heparin thromboprophylaxis that evening. The patient did not know the catheter was still in place due to their delirium in high dependency. The project team alerted the ward staff, placed an epidural alert wristband on the patient and ensured that there was an appropriate electronic handover documented. Another patient was excluded because their epidural catheter was removed before the correct time interval had elapsed after low-molecular-weight heparin had been administered. This patient was highlighted, a critical incident form completed and the patient monitored closely. Neither of these instances lead to the patient coming to harm.
The outcome measure run chart of overall survey score shows a sustained trend in improvement from a mean aggregated pulse survey score of staff from baseline 1.9 to 3.4 (68%) averaged over the last 3 months of the project time frame (figure 2). It demonstrates the cumulative impact of each PDSA cycle.
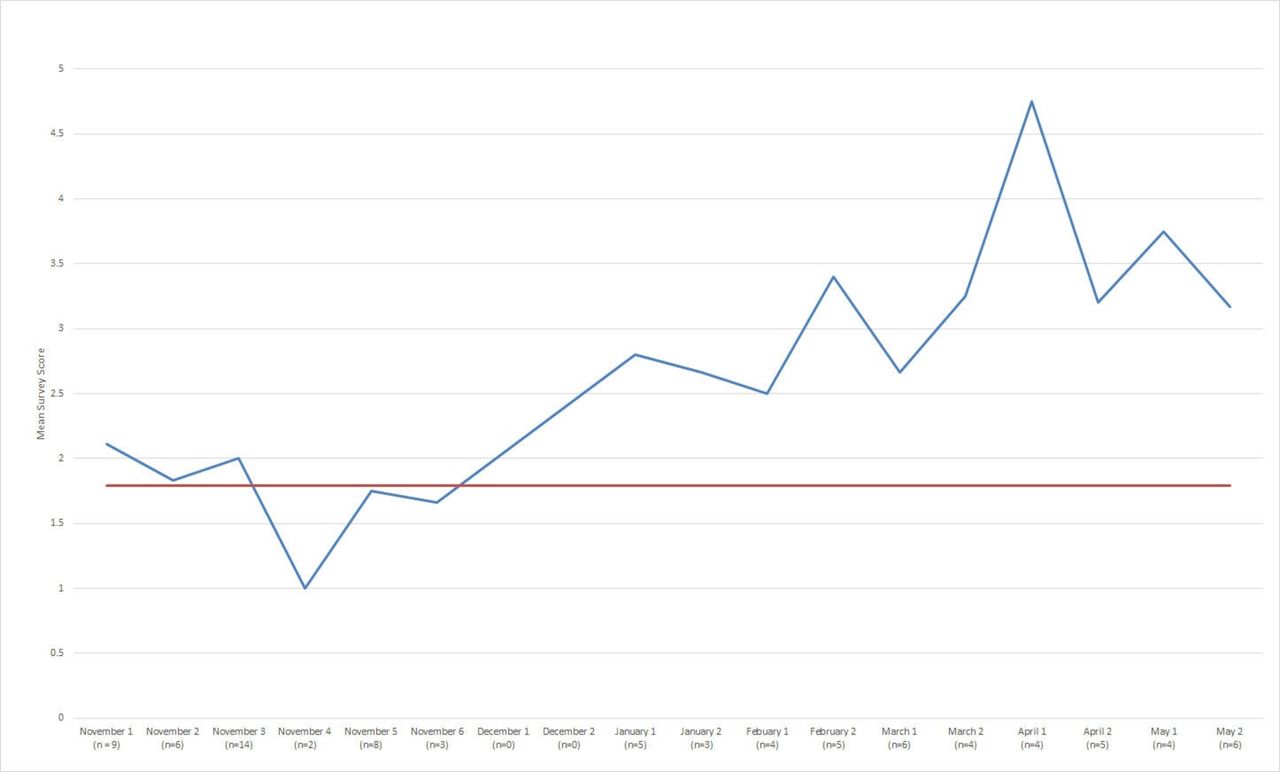
Aggregated mean pulse survey score for managing patients who have had a perioperative epidural.
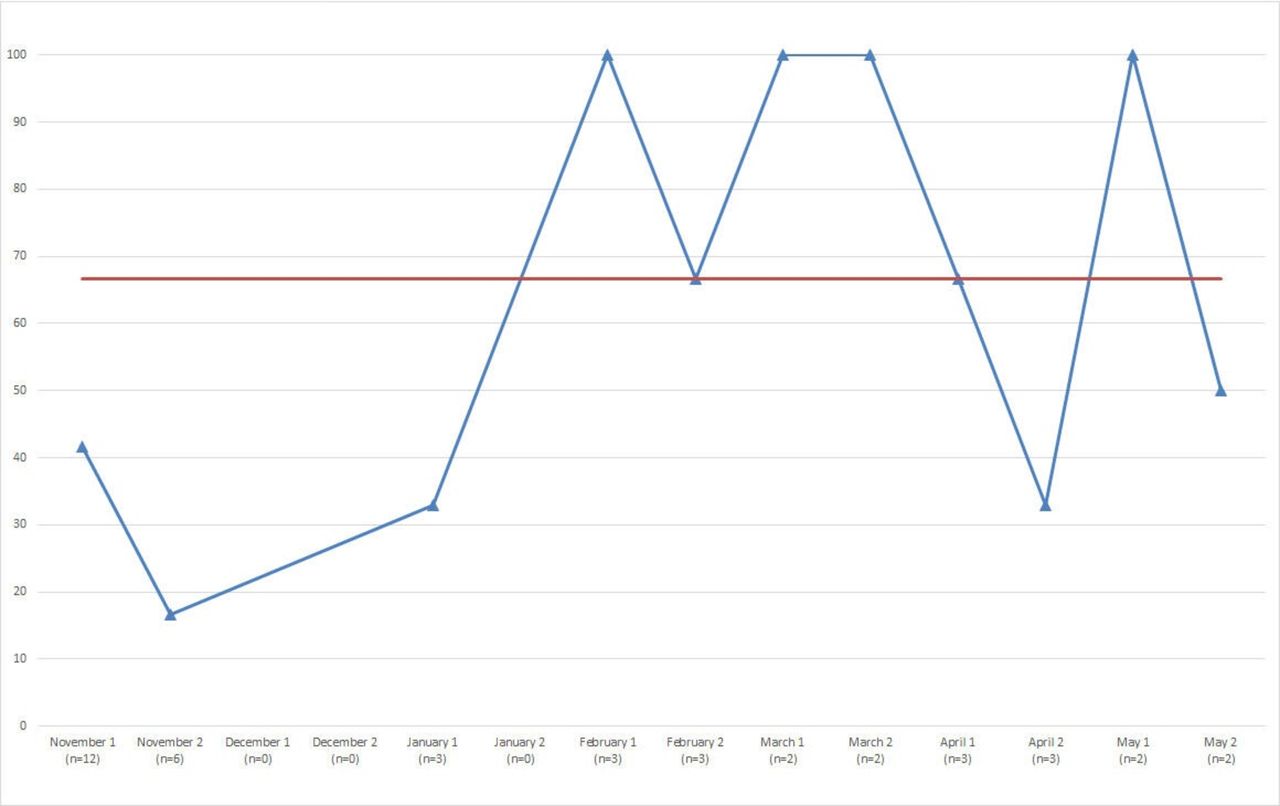
The run chart for whether the patient handover contained information about the patient having received an epidural showed a trend in improvement from PDSA cycle 1 in January 2019 (figure 3). The introduction of electronic nurse-led discharges from high dependency contributed to this improvement from January 2019 onwards. The mean baseline of 33% increased to an average of 71% over the last 3 months of the project time frame. This was essential to patient safety because without knowing which patients have received epidurals, the ward staff would not be able to interpret the onset of early neurological signs in the correct context and escalate promptly. Furthermore, they would not know how to perform focused neurological assessments (eg, motor block checks) for the 24 hours every 4 hours as per hospital policy.
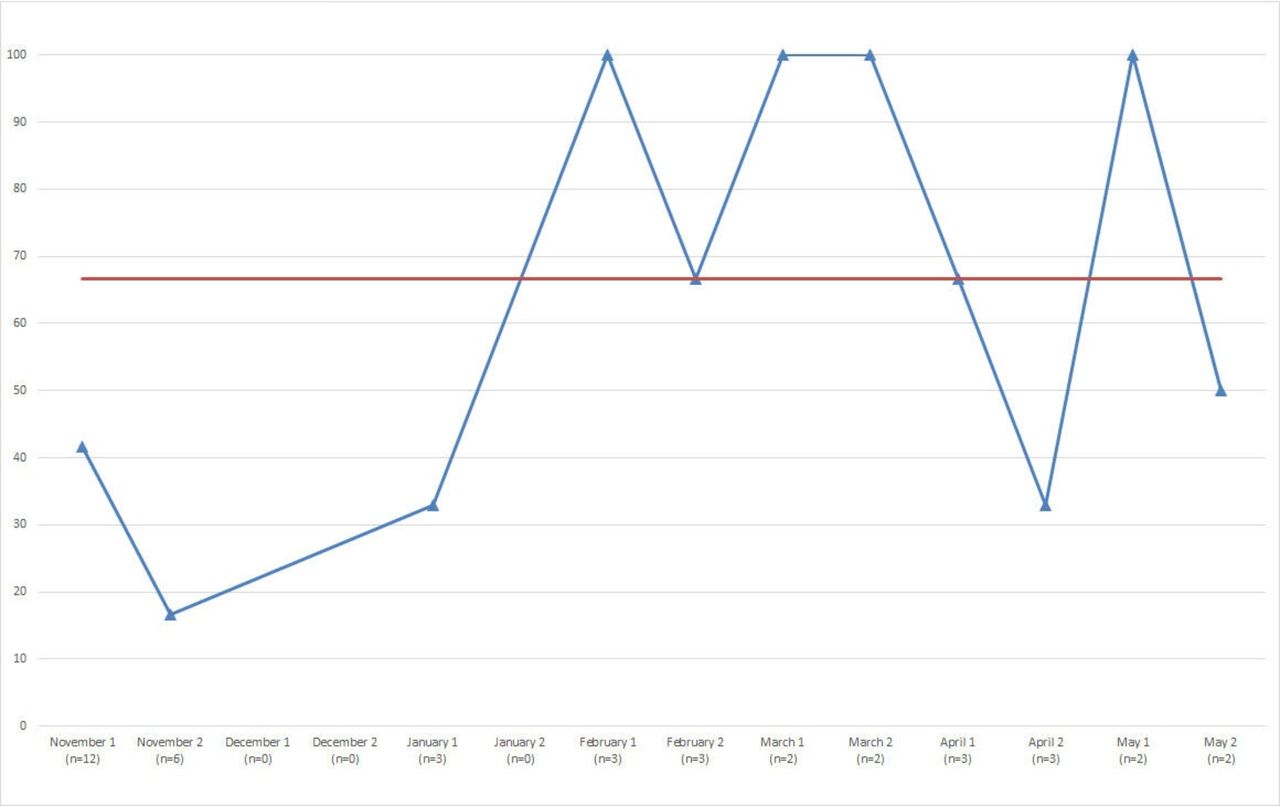
Process measure run chart: compliance with written handover.
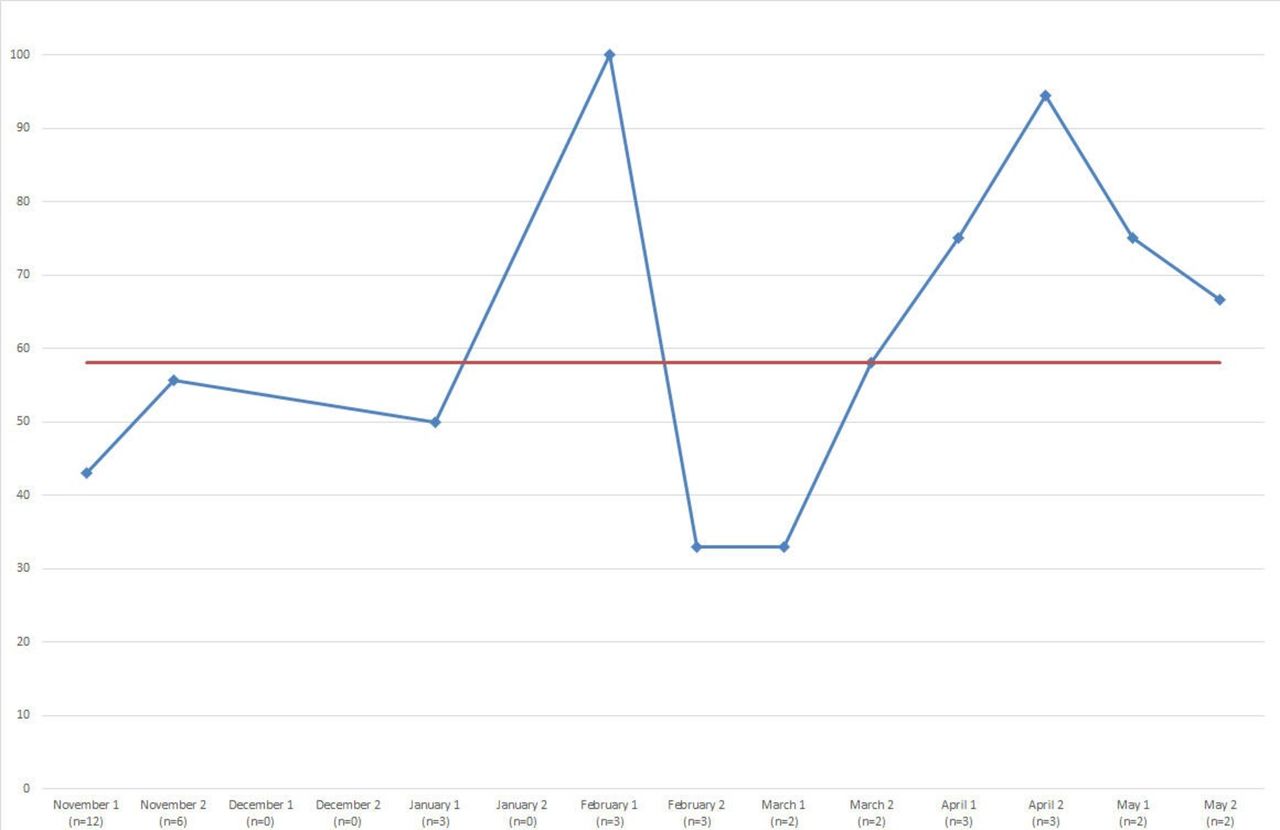
The run chart for the application of yellow epidural alert wristbands shows an increase from the start of the PDSA cycle 2 in February 2019 (figure 4). This included the epidural awareness campaign with posters promoting the application of the yellow epidural alert wristbands, and reminders to staff of the importance of these alert wristbands in morning daily handover huddles.
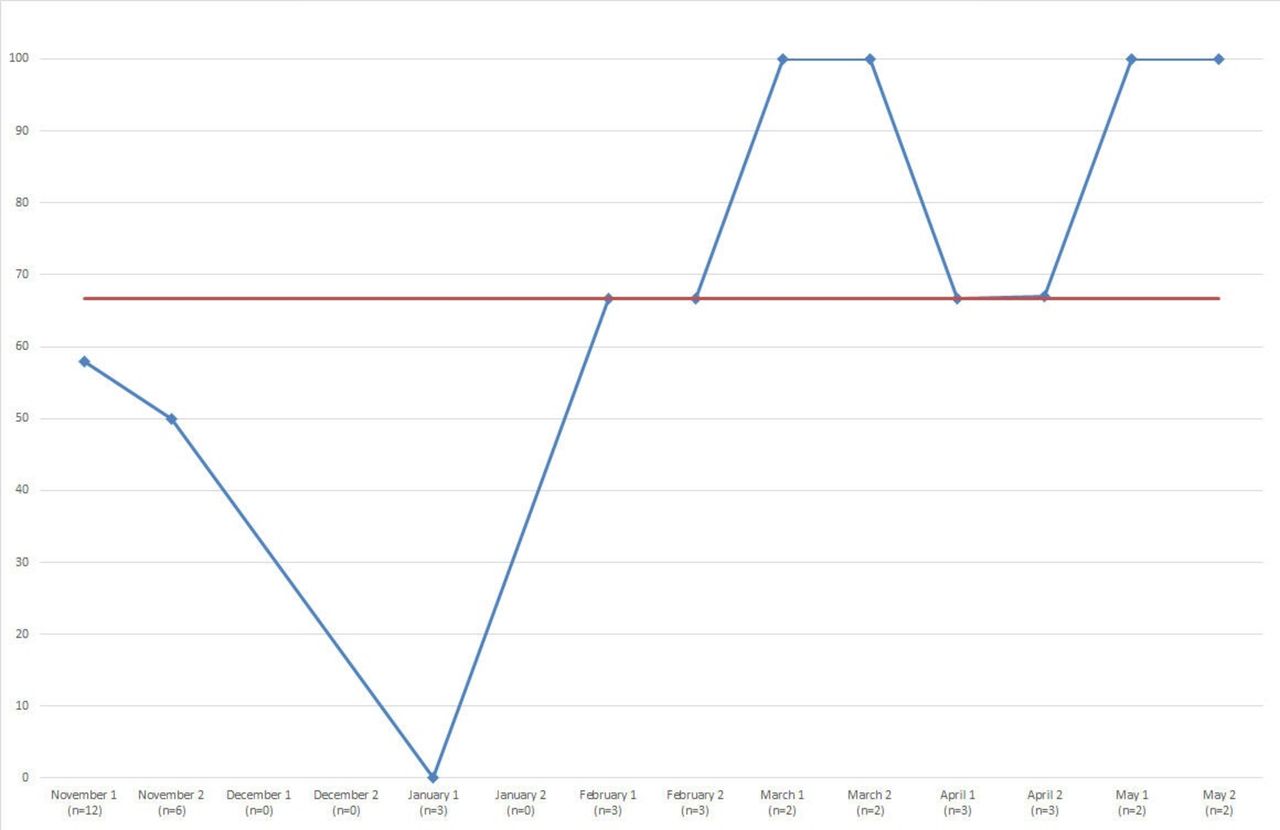
Process measure run chart: application of epidural alert wristbands.
The run chart demonstrating the percentage of motor block checks performed after the removal of the epidural catheter shows a run of 5 data points from mid-March 2019 onwards (figure 5). Healthcare staff performing motor block checks will have been encouraged by the continuous teaching sessions delivered on the wards and the interventions to make patients who have received epidurals readily identifiable including the improvement of handover to the downstream wards. PDSA cycle 3 involving the introduction of motor block stickers may have unfortunately contributed to the dip in motor block checks in May 2019 as these stickers were rarely applied. The expectation of a sticker that was not applied may conversely have worsened motor block checks. Subsequently, this intervention was abandoned. The low percentage of motor checks performed over the project time frame may in part reflect a failure of documentation. In practical terms, it is of vital importance that the MDT ward teams understand the significance of neurological or other symptoms in the context of a recently removed epidural catheter. Unfortunately, without appropriate documentation, it leaves an organisation open to medico-legal criticism.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Process measure run chart: compliance with motor block checks.
An important balancing measure was not to change or delay the step down of patients from high dependency or intensive care to any of the three surgical wards included in the project. The average length of stay in high dependency for these patients was not significantly different in the project time frame.
Lessons and limitations
The most significant learning point for our investigating team is around the data set collected during this QI project. By aggregating each data point, we have been less able to distinctly identify the impact of each individual test of change. This has also led to us being unable to set a true baseline median line on our process measure run charts, as we obtained too few data points prior to commencing tests of change. It is however reassuring to see trends crossing the median line set from all of the data points available, suggesting our interventions have led to improvement in these areas. The median line in our outcome measure run chart was created from 6 aggregated data points, all collected in November. The authors acknowledge that the periods between data collection episodes of this initial baseline audit data are not identical after the tests of change were introduced. The investigators were also unable to undertake data collection during December 2018, due to staff availability. This has been represented on our run charts as ‘n=0’, however we understand that it would have been most ideal to continue bimonthly data collection from the moment initial data collection was commenced.
The QI project has tackled the complexities of improving service delivery for patients receiving epidurals across multiple different areas. This relied on communication between many different teams and the support of multiple different key stakeholders in each area. One of the surgical wards was resistant to the project initially, due to their different priorities with finite resources. The investigating team was asked to return to provide micro-teaching at an alternate time on multiple occasions. This made their uptake of teaching far less than the other wards and the area generally performed less well in all project areas. Arguably the project may have benefited from focusing its interventions in one specific ward area. This might be considered a SMART goal. On the other hand, the frequency of patients receiving epidurals in the hospital was only a few each week, meaning that by targeting only one ward, we would have significantly limited the number of epidural patients in our data collection and the impact of our interventions.
In terms of study design, the assessment of competence through pulse survey questioning does expose our results to interassessor variation. To minimise this variation, all three assessors discussed potential interpretations of questions and agreed on standardised minimum responses to achieve a score of 1. However, this could have been improved on by having a single assessor for all surveys. In addition to this, the investigating team recognise that collection of qualitative data would have been hugely valuable, to thematically analyse specific areas where knowledge or confidence gaps in managing these patients existed, thus providing clear targets for further PDSA cycles.
The nursing ward staff have huge demands already on their time and a balancing measure of the project was not to impose any significant additional workload on the ward teams. It was observed that they usually complied with motor block checks only when they could be done in combination with their routine patient observations. This meant that unless a patient was on four hourly observations for another reason then they did not get all of their four hourly motor block checks performed for 24 hours after epidural catheter removal. When electronic observations are brought into our hospital, it would be useful ‘forcing function’ to tie these motor block checks into the e-observations system that have an electronic prompt.
It is important that the low percentage of motor block checks performed even in the intervention months of the project may reflect documentation. It would be a reasonable expectation that if a patient suddenly develops weak leg(s) that the patient would alert the ward staff. A caveat is that patients cannot be wholly relied on as evidenced by one of the patients excluded in the project data. This patient had been confused in high dependency and did not know that their epidural catheter was still in situ on the step-down surgical wards. A potential improvement for the future would be focusing on patient education and empowerment regarding the symptoms of an epidural haematoma. Nevertheless, the project priorities were staff communication and knowledge. This would ensure that the ward staff members were able to identify which patients had recently had an epidural catheter removed or one in situ. Furthermore, that the staff were adequately trained to understand the significance of a presentation of lower limb weakness, back pain or sphincter dysfunction in this context. The healthcare staff would then be able to escalate appropriately.
The introduction of nurse-led discharges from high dependency was excellent in ensuring that the ward staff received a standardised handover, which improved communication in general. However, this handover still sometimes did not have any mention of the epidural. Unfortunately, within the project time frame it was not possible to negotiate the addition of appropriate epidural information to the electronic performance with the area leads, and the information technology team. We plan to institute and measure this test of change as soon as possible.
The yellow epidural alert wristbands were applied in both theatre recovery areas, high dependency and intensive care wards, and were intended to remain on the patient for the duration of their hospital stay. There is a strong argument that these wristbands could be applied at the time of epidural insertion by the anaesthetic team in theatre to avoid being missed in recovery. However, it was not possible at the time of the project to get support and to change the practice of a large body of anaesthetic consultants. The authors intend to discuss whether this would be possible to change, with some key stakeholders within the anaesthetic department.
QI methodology is now being used in all areas of medicine and surgery to continuously improve patient care and healthcare processes. There are a number of QI techniques in use which could have been applied to this project (depending on whether we are looking at the whole process or focusing on one particular area for intervention). Lean theory for example looks at processes from beginning to end and tries to establish how flow could be improved. We have touched on this in our project by introducing changes at various different stages in the patient journey (eg, the wrist band which should be applied when the epidural is inserted, the handover from high dependency unit to the ward and the training of surgical ward staff in post-epidural care), although formally addressing the five elements of lean theory would be beneficial ((1) identify value, (2) identify the value stream, (3) create flow, (4) create systems that pull and (5) strive for perfection). By comparison, six sigma methodology usually focuses on refining and standardising a single step in the process. This is arguably a more simple methodology which can be used effectively in a project such as ours to improve individual steps in the process.
Finally, it is important to note that this is an ongoing project with many threads to be followed up on. The aims of this QI project extend long beyond the time constraints of this piece of written work. We endeavour to continue to make adjustments and measure both their short-term and long-term impacts, until excellent post-epidural care is embedded in the work culture of our surgical wards.
Conclusion
The application of robust QI methodology contributed to a sustained improvement in the competence of healthcare staff at managing step-down patients who have received perioperative epidurals during their hospital admission, over a period of 6 months. Educational interventions alone are difficult to sustain, given the high turnover of staff, shift working patterns in these areas and level of input required by those individuals delivering teaching sessions. Therefore, we have promoted sustainable improvement by also focusing on system changes to make these patients readily identifiable. This was done by improving the quality of handover from high dependency to the step-down wards, and ensuring the application of yellow epidural alert wristbands. It is hoped that the combination of methods, ongoing plans for interventions and involvement of the local pain team will achieve the culture of change required. The relative infrequency of epidural haematoma and abscess as a complication2 4 means that expensive additions to current practice are not practical. However, for the individual this complication is life-changing, and there is good support for simple inexpensive measures such as having these patients immediately identifiable, performing and documenting motor block checks for 24 hours’ post-removal of epidural catheters, as well as a widely held staff understanding of the signs and symptoms of developing complications, and how to escalate these concerns appropriately.4
References
Footnotes
Twitter @deetssleeps
Contributors The authors would like to thank the SQuARES Network (South East Scotland School of Anaesthesia Quality Improvement, Audit and Research Network), the Acute Pain Team as well as staff across recovery, high dependency, intensive care units, vascular, general surgery and gynaecology who all contributed to improving patient care.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.