Article Text

Abstract
Medical records are crucial facet of a patient’s journey. These provide the clinician with a permanent record of the patient’s illness and ongoing medical care, thus enabling informed clinical decisions. In many hospitals, patient medical records are written on paper. However, written notes are liable to misinterpretation due to illegibility and misplacement. This can affect the patient’s medical care and has medico-legal implications. Electronic patient records (EPR) have been gradually introduced to replace patient’s paper notes with the aim of providing a more reliable record-keeping system. It is perceived that EPR improve the quality and efficiency of patient care. The paediatric department at Queen’s Hospital Burton uses a mix of paper notes and computerised medical records. Clinicians primarily use paper notes for admission clerking, ward rounds, ward reviews and outpatient clinic consultations. Laboratory tests, imaging results and prescription requests are executed via the EPR system. Documentation by nurses is also carried out electronically. We aimed to improve and standardise clinical documentation of paediatric admissions and ward round notes by developing electronic proforma for initial paediatric clerking, ward rounds and patient reviews. This quality improvement project improved clinical documentation on the paediatric wards and enhanced patient record-keeping, boosted clinical information-sharing and streamlined patient journey. It fulfilled various generic multidisciplinary record keeping audit tool standards endorsed by the Royal College of Physicians by 100%. We undertook a staff survey to investigate the opinion before and after implementing the electronic health record. Doctors, nurses and healthcare support workers overwhelmingly supported the quality, usefulness, completeness of specified fields and practicality of the electronic records.
- electronic health records
- paediatrics
- continuous quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The National Health Service (NHS) in the UK is considered as one of the most developed healthcare systems across the globe. Over the years, the NHS has aspired to have fully integrated electronic health records (EHR) across the UK, first recorded in its information management and technology strategy in 1998.1 Various attempts at implementation have been met with hurdles, particularly budgetary constraints. Moreover, various providers in primary and second healthcare have implemented a variety of EHR solutions with limited or no provision of integration across various tools for seamless access by all healthcare professionals from any health facility in the UK.
Prior to 2019, doctors’ clinical records in the paediatric department at Queen’s Hospital Burton were made using pen and paper as a medium. This renders the clinical records susceptible to medical errors due to inaccuracies, misinterpretation, misplacement and physical loss. On the other hand, nursing staff and other healthcare professionals in the department ubiquitously use EHR for their record-keeping. This creates a dissociation between the medium of documentation within the same department, further risking miscommunication. Early local audits have also shown that paper records are insufficient in meeting national standards of documentation.
Queen’s Hospital Burton uses MEDITECH’s integrated EHR solution, which supports clinical documentation, computerised provider order entry, laboratory reporting and electronic prescribing.
The Specific, Measurable, Achievable, Realistic and Timely (SMART) aim of this project was to improve the paediatric clinical documentation standards to ≥90% in each domain according to Royal College of Physicians (RCP) standards described later, within a year of each implemented change. This required educational drives and EHR implementation, ensuring a robust, portable and accessible set of health records.
Background
Clinical documentation is the process of generating a structured record of a patient’s medical care. This record of medical information assists in optimising patient care, enables communication between health professionals involved in the patient’s care, supplies data for audits and research as well as serves as potential evidence for medico-legal cases.
The General Medical Council originally defined a framework for Good Medical Practice (1995), recommending ‘clear, accurate and contemporaneous patient records’.2 This has been largely unchanged in the latest edition of Good Medical Practice (2013, updated 2019).3 The Professional Record Standards Body, endorsed by the RCP, has published standards for the clinical structure and content of electronic health records, reflecting best practice.4
Much of clinical documentation is still handwritten, rendering it susceptible to errors in record-keeping. Commonly touted examples include poorly legible handwriting, inaccurate patient identification, inaccurate timestamping, lack of signature and lost records.5 6 These, by themselves or in combination, may contribute to medical errors and compromise patient safety.7
EHRs have been proposed as a solution to enable healthcare professionals to generate good clinical records. The EHR is operationally defined by the US National Institute of Standards and Technology as ‘a longitudinal collection of patient-centric healthcare information available across providers, care settings and time’.8 By maintaining an accurate record of patient’s clinical data, EHRs aim to optimise and streamline a clinician’s workflow. This in theory not only establishes a more robust set of health records but also has the advantage of increased accessibility, portability, security and searchability.9 The UK government has devised the National Health Service Long Term Plan which aims to digitalise all health records by 2024.10
The evidence for benefit of EHR is largely favourable. A number of studies have shown an improvement in record-keeping quality and efficiency11 12 as well as measurable clinical outcomes.13 14 However, other studies have shown no significant benefit in clinical outcomes after the implementation of EHR or worse, an increased risk.15 16 It is thus debatable that EHRs are only able to better achieve quality metrics rather than actually improving clinical outcomes. Hence, any EHR implementation should carefully consider the benefits as well as the risks.9 17
This quality improvement (QI) project broadly sets out to answer two key questions.
By implementing EHR, is there an improvement in documentation completeness and quality?
Does the EHR fit the users’ needs?
This, while not necessarily generalisable to other organisations, can result in a highly efficient fit-for-purpose local tool.9 18
Measurement
Initial data collection was carried out using the RCP generic multidisciplinary record keeping audit tool (2011).19 Standards 1, 7, 9, 10, 11 and 12 were not measured as these were either not applicable or difficult to measure retrospectively. It covered the Children’s Wards which consists of 20 inpatient beds.
The inclusion criteria reflected in the Audit Tool was
Admission duration of >24 hours and <30 days.
Review of all recorded entries between admission and discharge.
The baseline audit was carried out in May 2017, involving 10 patients and 72 pages of health records. A sample of 10 patients was selected as set out in the RCP generic multidisciplinary record keeping audit tool (2011).19 A single patient’s clinical records during the admission was audited for up to 14 days. This audit found that the record-keeping standards were severely lacking in documenting patient identifiers (<50%), printed name of entry writer (49%) and printed grade of entry writer (51%). The utilisation of the admission clerking proforma was surprisingly low at 60% despite easy access and free availability on the wards (table 1).
Baseline data of record-keeping standards (in %)
Disappointing results from May 2017 audit steered us to develop this QI project. During this project, in order to improve local clinical documentation standards, we used the same audit tool to measure the outcomes after every intervention using a phased improvement project. The expected standard for documentation was a compliance rate of ≥90%.
Design
A structured paper admission clerking proforma was developed and implemented in the 1990s in order to improve inpatient admission documentation, and has been used since. Following the May 2017 audit, educational drives were taken in the form of departmental presentations. This served as a reminder to the junior doctors to complete the clerking proforma as well as sign and timestamp their entries. Later, these educational sessions were integrated into the departmental inductions to ensure consistent training during staff changeover. Each new member of the paediatric department necessarily participated in a departmental induction. Despite these measures, RCP generic multidisciplinary record keeping audit identified poor clinical documentation standards. This led to developing and implementing EHR within the paediatric department. The QI team consisted of a paediatric consultant, a junior paediatric doctor and MEDITECH support staff. Three separate EHR documents were designed which included an admission clerking proforma, an inpatient review note and a ward round note. After a pilot run, these electronic documents were built on the existing departmental EHR framework at Queen’s Hospital Burton. We ran induction sessions to train doctors to use newly implemented EHR.
Key features of the EHR were as follows:
Completion of mandatory fields before submission/final sign off
Clerking proforma which pulled data from previous admissions (where applicable)
Automatic referencing of patient’s details
Streamlining of admission care plans into the discharge letter
Documentation of designated bleep number to improve identification.
A user survey was carried out before and after the implementation of the EHR. This was to gather users’ opinion, gauge their satisfaction and address any concerns they had regarding the EHR. This was to ensure the end product was not only fit for purpose but also satisfied users’ needs.
Strategy
Phased improvement cycle 1 (December 2017)
Following the baseline data collection in May 2017, educational sessions were carried out to improve the awareness and understanding of the clinical documentation. A re-audit was completed in December 2017 using the same audit tool with encouraging results. Even though, documentation structure (standard 3) and chronological note sequences (standard 4) improved to 100%, shortcomings persisted in standards 2, 5, 6 and 8 (table 1).
Phased improvement cycle 2 (May 2018)
A re-audit in May 2018 demonstrated a decline in some record-keeping standards such as accurate date and timestamping a written entry. The audit also showed a failure to accomplish the expected standard of documentation, such as patient name and ID documentation (standard 2) being 56% and 46%, respectively (table 1). These results were postulated to be secondary to regular turnover of staff, prompting an action plan to integrate regular clinical documentation training into the departmental induction.
Phased improvement cycle 3 (April 2019)
Further re-audit in April 2019 showed marginal improvement in some record-keeping standards (table 1). However, a significant number of standards were still unmet particularly those involving patient identification (standard 2), timestamping entries, signing entries, recording grade (standard 6) and most senior clinician recording (standard 8). This led us to develop and implement the EHRs in the paediatric department as EHRs have the advantage of trivialising these sections of the record.
Phased improvement cycle 4 (July 2019)
The final cycle assessed the documentation standards after implementation of EHR. A re-audit in July 2019 was carried out with the same cohort of staff (as in April 2019) which demonstrated a universal improvement (100%) in all standards (table 1).
Results
Over each phased improvement cycle, a general improvement in clinical record-keeping was achieved in some of the standards. Educational drives were found to be efficacious but did not meet our recommended standards (≥90%) globally. Implementation of the EHR allowed us to achieve these standards. A post-implementation survey was carried out to gauge user satisfaction and further refine the EHR to suit the end-user’s needs. The user survey demonstrated a generally positive attitude toward the EHR.
Assessing quality of documentation in accordance to national standards
The first question to be answered was whether the interventions had any measurable effect in clinical documentation standards. On the administration of educational methods, the expected documentation standards of ≥90% were achieved in improved dating of entries (87%–96% at phased improvement cycle 1), correct completion of the proforma (80%–100% at phased improvement cycle 2) and uptake of clerking proforma (60%–90% at phased improvement cycle 3). Compliance towards including a signature also improved from 49% to 87% after phased improvement cycle 3. Critically, documentation of patient’s name (49%–58%), patient identification (42%–51%), recording of clinician’s grade (51%–76%) and recording of most senior clinician (75%–37%) remained well below required standards of ≥90% at phased improvement cycle 3. Following the implementation of the EHR, all standards were met at 100%.
Assessing doctors’ opinion in using the EHR
General sentiment and overall satisfaction
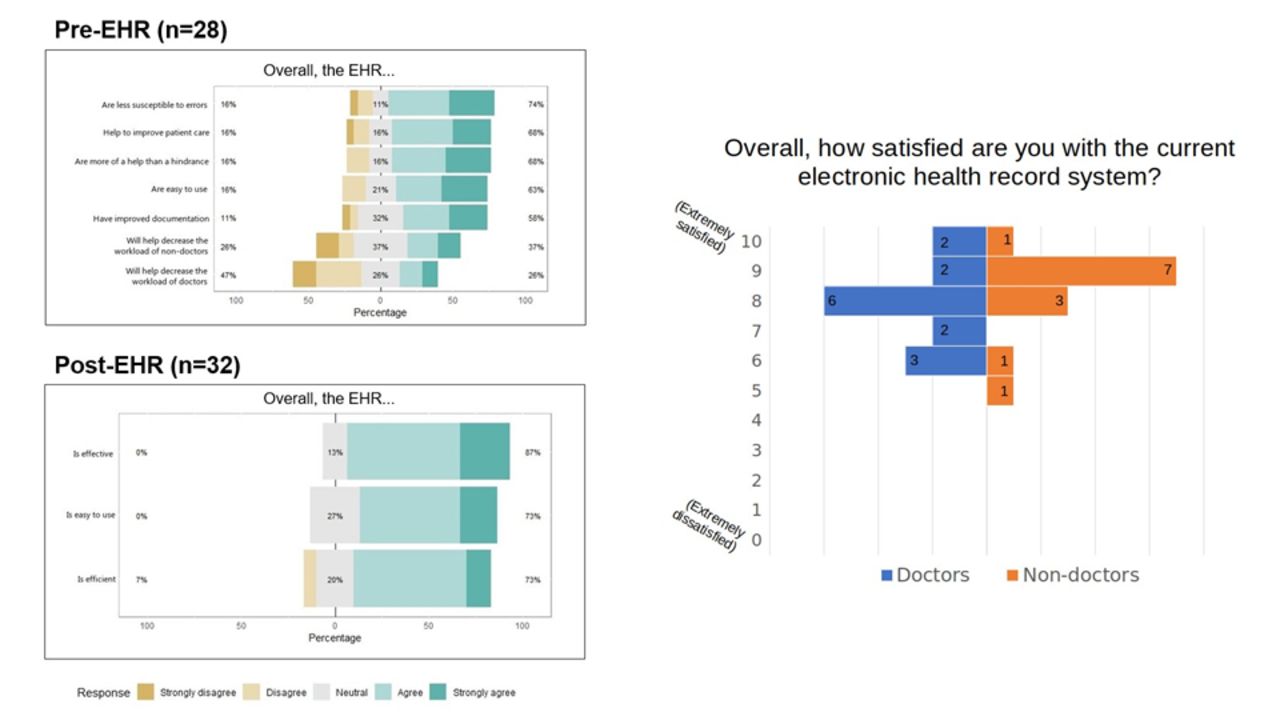
There were similar numbers of respondents in both surveys, with 28 respondents in the pre-EHR survey (15 doctors, 13 non-doctors) and 32 respondents in the post-EHR survey (19 doctors, 13 non-doctors). During the pre-EHR survey (figure 1), respondents generally answered favourably towards the benefits of EHRs, agreeing that EHRs will be less susceptible to errors (74%), would help to improve patient care (68%), would be easy to use (63%) and will improve documentation (58%). However, only 47% of respondents felt that it would decrease their workload. In the post-EHR survey (figure 1), respondents had far greater affirmative response towards EHR with an overwhelmingly larger proportion of them agreeing that the EHR had positive impact. They felt that EHR was effective (87%), easy to use (73%) and efficient (73%) with small number of respondents disagreeing (7%).
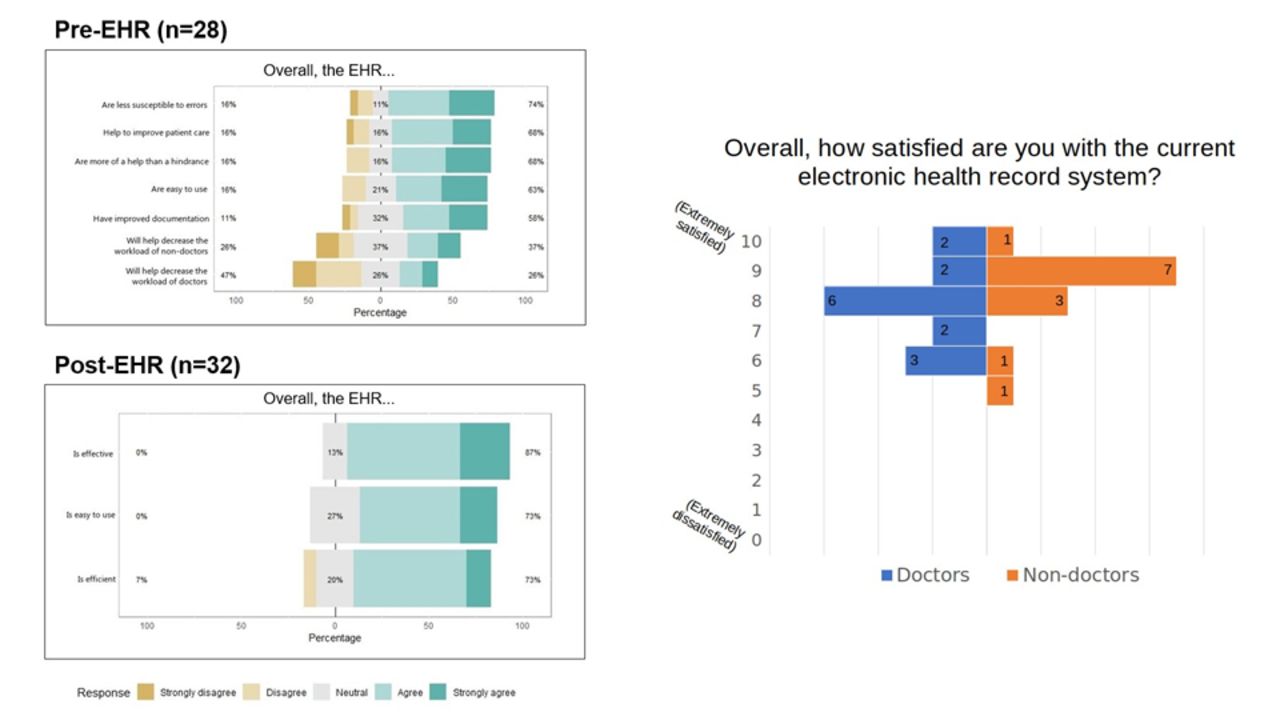
Overall responses towards EHRs in general, before and after EHR implementation. EHR, electronic health records.
Use of clerking proforma and ward round notes
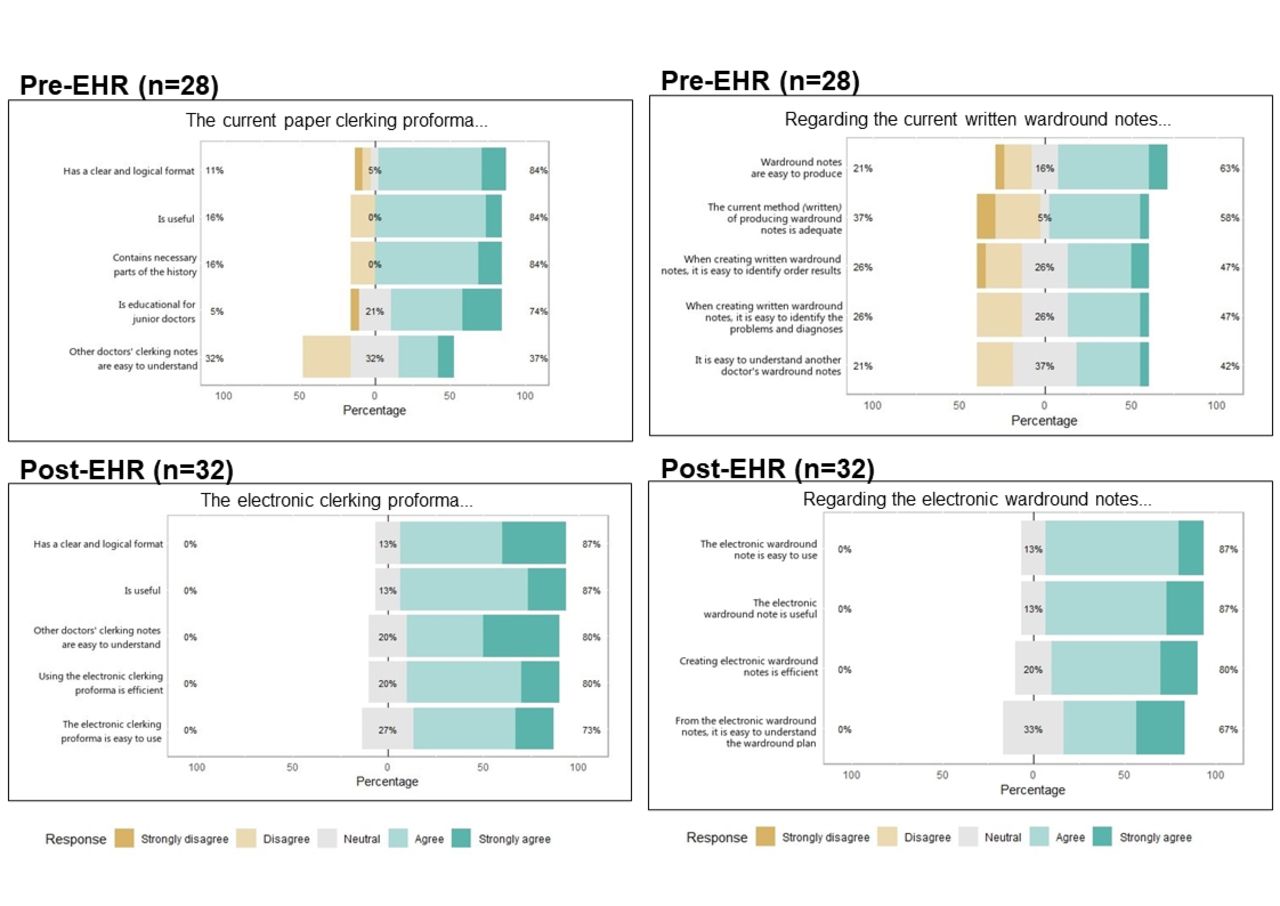
During the pre-EHR survey (figure 2), majority of the responders supported the use of the existing paper clerking proforma noting its logical formatting (84%), general utility (84%), comprehensiveness (84%) and educational utility (74%). More than 2/3 responders disagreed or remained neutral when asked whether other doctors’ clerking notes were easy to understand. Post-EHR survey showed an overwhelmingly positive response with agreement rates of 73%–87% for all the questions (no disagreements at all). Most notably, the reports of difficulty in understanding other doctors’ clerking notes had vanished after the implementation of the electronic clerking proforma.
{kind=link}
{kind=link}
Responses towards the electronic clerking proforma and electronic ward round notes before and after EHR implementation. EHR, electronic health records.
During the pre-EHR survey, only 42%–63% of the doctors felt paper ward round notes to be adequate, easy to produce and found it easy to understand ward round notes made by other doctors (figure 2). In the post-EHR survey, the responses were overwhelmingly positive in favour of the electronic ward round notes (67%–87%) with no disagreement at all.
Assessing non-doctors’ opinion in using the EHR
A similar survey was also completed by non-doctors comprising of nurses, pharmacists, healthcare support workers and the ward clerk. The responses had a pattern resembling that of the doctors in that there were more negative or equivocal responses prior to the EHR implementation which progressed into overwhelmingly positive responses. After implementation of EHR, non-doctors felt that there was an improvement in the ease of understanding of a patient’s management plan and its general utility.
Prior to EHR implementation, non-doctors routinely used the EHR for their own documentation but referred to paper record for notes made by the doctors. It is thus unsurprising that by unifying the medium of clinical documentation, greater staff satisfaction was observed.
EHR implementation: benefits and challenges
During the survey, the respondents’ opinion was also sought regarding the advantages and disadvantages of electronic notes (table 2). This qualitative data was crucial to identify potential problems early and address them in a timely fashion. For example, there were concerns regarding information excess with too many mandatory fields in the clerking proforma which were deemed clinically irrelevant. This had potential consequences with unnecessary delays and back log during a patient’s admission. This was addressed by a consensus decision to decide a minimum set of mandatory fields within the clerking proforma. Another example was the apprehension of the availability of sufficient computers when seeing patients simultaneously by the on-call doctors during the busy time period. This was addressed by budgeting and purchasing new wheelie laptops for the department.
Benefits and challenges of electronic health records implementation
Lessons and limitations
This project reflected a progression towards improving clinical documentation, beginning with simple measures and upgrading to systemic changes. One of the key aspects of the project was iterative development to generate sustainable change. This phased improvement project spanned four cycles, each of which implemented a slightly different change to the existing practice at that time in order to address the identified problems. The first two phased improvement cycles resulted in targeted small group tutorials. However, on discovery that it was unsustainable during staff changeover, the training sessions were integrated into the departmental induction. Later, after recognising that it was primarily the robotic aspects of clinical documentation which were missed, the EHR was implemented to robustly achieve the documentation standards. This tackled the problem at a systemic level and removed human error from the equation. Building on our current iteration of the EHR, we will seek regular feedback from the users to continue to refine the EHR to suit their needs.
Another strength of this project is its user-centred and data-driven focus. Prior to implementation of the EHR, a survey was undertaken of its potential users to measure their perception of EHR and whether it would be advantageous to implement it. We used quantitative and qualitative data to identify key concerns about clinical documentation and addressed them while the EHR was in the development stage. We also explored aspects of an EHR which our users would find helpful and integrated them into our EHR design. After implementation, we again sought feedback from the users to refine the EHR to ensure it met their needs. This is crucial because it is not uncommon to bring about a new systemic change within an organisation without consulting the end users leading to increased pressure, distress and frustration among them.
When developing this project, collaborative consultations took place and opinions were gathered from members of different teams. We worked with nurses, healthcare support workers and other staff members to better understand their views on the EHR. As they have been using EHR for routine documentation for several years, we were able to use their knowledge and experience when designing and refining the EHR for doctors. This also fostered local confidence in instigating organisational change.
This project has its limitations too. Applicability of our methodology in resource-limited Trusts with primitive electronic clinical information system (CIS) will be challenging. We were privileged to already have an advanced CIS in place for electronic prescribing and viewing laboratory results, thus minimising the overheads to develop and implement the EHR. Other hospitals which do not already have a CIS will have to consider the added financial cost to their EHR implementation. We are optimistic that the user-centred strategy we adopted to design the EHR will also be used in QI interventions in secondary and tertiary care facilities across the country.
The data collected from this project had its own shortcomings. First, the audit data used the RCP generic multidisciplinary record keeping audit tool. On implementation of the EHR, almost all standards were immediately met at 100%, reaching a ceiling effect. This rendered this tool unusable for further audits of this nature. Second, this tool also uses a sample size of 10 patients per audit cycle, which we adhered to. Although this appeared to be a small sample size in patient numbers, the audit tool measures the number of pages filled which meet the criteria which is the more direct measure of compliance. Third, the survey data was primarily qualitative and exploratory. Due to the nature of this QI project, there were no quantifiable clinical outcomes. To address these problems, we recommend further steps including creating a locally defined set of documentation standards or using an evaluation instrument such as the QNOTE in order to better quantify performance metrics.20
Conclusion
Good clinical documentation is an important part of patient’s clinical care. Hence, as healthcare professionals, we need to strive for highest standards of clinical documentation. While simple methods such as educational drives can be beneficial, these are only moderately efficacious and are not sustainable. Implementation of doctors’ EHR improved the paediatric clinical documentation standards to 100% in each domain compared with pre-implementation standards in a robust and sustainable way. Based on the feedback received, we refined the EHR locally to suit the end-user’s needs. Building on this groundwork, we aim to use different outcome measures to ensure continuous improvement in our clinical documentation standards. In the years to come, every patient will eventually have fully comprehensive EHR, using a single NHS electronic database platform, so the information is readily accessible from any NHS facility in the UK.
Acknowledgments
We would like to acknowledge the contributions made by Dr David Anderson and Ms Jessica Dutton (MEDITECH staff) in enabling us to develop and implement EHR. Thanks are also due to the paediatric medical and non-medical staff who supported this project and provided invaluable feedback as without their backing, this project would not have been possible.
Footnotes
Contributors JK initiated the project, performed data collection, analysis and writing of the manuscript. MA made critical revisions and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This project was planned to improve the service for paediatric patients. Hence, it was not deemed to require ethical approval. The interventions were designed to standardise and enhance accepted good medical practice.
Provenance and peer review Not commissioned; externally peer reviewed.