Article Text

Abstract
Hypertension is an important modifiable risk factor for cardiovascular disease in patients with diabetes. Despite established guidelines, the percentage of patients meeting the target blood pressure (BP) of <140/90 mm Hg in clinic remains suboptimal. In this project, we sought to improve BP measurement in an outpatient diabetes clinic.
Two interventions were performed: (1) Changes were made to the timing of BP measurement during patient intake and (2) An electronic medical record (EMR) alert reminded staff to repeat BP if the initial reading was above target. Baseline data were collected on 4764 patients, with 72.5% meeting their BP target. After implementation of changes to the timing of BP measurement during patient intake, 73.3% of patients met the target (no significant change). However, after implementation of the EMR alert, there was a statistically significant improvement in patients meeting the target BP at 76.8% (p<0.01). This reduction was driven by the high percentage of patients with an initially elevated BP measurement that came down into goal range on repeat measurement. Those who remained above target despite multiple readings could be referred to a new pharmacist-led hypertension clinic to ensure adequate follow-up and medication adjustment.
It is important to ensure that in clinic BP measurements are taken correctly and adhere to best practices. Use of a single in-clinic BP measurement may result in overtreatment of hypertension. While timing of BP measurement during patient intake was not important, repeating high BP measurements did improve the number of patients in an outpatient diabetes clinic meeting their BP target.
- continuous quality improvement
- quality improvement
- performance measures
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Blood pressure (BP) is an important modifiable risk factor for serious cardiac morbidity and mortality. The 2017 Healthcare Effectiveness Data and Information Set (HEDIS) quality measure from the National Committee for Quality Assurance defines a BP target of <140/90 in patients 18–85 with diabetes and a diagnosis of hypertension.1 The percentage of patients meeting their target nationally remains suboptimal with rates in 2017 ranging from 54.5% to 72.0% for commercial Preferred Provider Organization (PPO) insurance and Medicare Health Maintenance Organization (HMO), respectively.1
The Michigan Medicine Metabolism, Endocrinology and Diabetes (MEND) clinic is a large university affiliated endocrinology clinic which includes approximately 30 board certified endocrinologists as well as eight endocrine fellows. An initial data review using BP measurements performed by our clinic during calendar year 2016 found that only 72.6% of patient with diabetes had a BP <140/90 mm Hg at their most recent visit.
During the planning phase for this project existing workflows for BP measurement and management were reviewed. We identified three specific, actionable areas for improvement with the current processes:
Problem #1: BP measurements were being performed in intake bays on arrival. This has led some patients to report that their readings were erroneously high due to the stress of getting to the appointment, exertion walking in from the parking lot to the clinic, and the anxiety of having a finger stick haemoglobin A1c (HbA1C). These measurements were not in accordance with existing guidelines which recommend a period of rest prior to taking BP measurement.
Problem #2: Single in clinic BP measurements were being taken rather multiple measurements. While BPs could be repeated at the discretion of the performing medical assistant (MA) or the physician, this was only happening in a small minority of cases. Previous studies have called into question the reproducibility of in clinic BP measurement,2 and current guidelines recommend that when in clinic measurements are used multiple measurements are taken to ensure accuracy.3 4
Problem #3: For patients with a high BP measurement in clinic, follow-up was often inadequate. Diabetes follow-up visits are typically scheduled for 3-month intervals so if treatment intensification was recommended by the physician, patients were not being seen back in a timely manner to confirm that the medication adjustments were adequate.
This project aimed to increase the percentage of patients with type 1 or type 2 diabetes who have a BP of <140/90 mm Hg at their most recent MEND clinic visit to 75%. This goal was selected based on the HEDIS 90th percentile and also aligns with our own institutional ambulatory care benchmarks. The project included all patients seen in the Michigan Medicine adult endocrinology clinic during the specified time interval. The intervention was limited to the primary clinical site and satellite clinic locations were excluded. While all patients seen in the clinic were impacted by the changes to clinic workflow, only patients age 18–85 with a diagnosis of type 1 or type 2 diabetes were used for the final data analysis and primary outcome measure.
Background
Hypertension is an important risk factor for stroke, myocardial infarction, heart failure, vascular disease and is one of the leading causes of cardiovascular mortality.3 Hypertension is common among patients with diabetes and it is recommended by the American Diabetes Association that BP be checked at every routine clinical visit.5 While the ideal BP target for patients with diabetes has been debated in recent years, it is clear that a target of at least <140/90 for patients with diabetes is beneficial in terms of prevention of cardiovascular events and microvascular complications.5 6
In order to accurately identify patients with elevated BP, correct measurement technique must be used. Guidelines from the American College of Cardiology (ACC) and the American Heart Association (AHA) recommend that patients sit calmly for at least 5 min and avoid caffeine, exercise and smoking for at least 30 min prior to measurement. The BP device must be calibrated and appropriate cuff size should be used. Repeat measurements should be separated by 1–2 min. The average of at least two measurements performed on two or more separate days is used to diagnose hypertension.3 Although a seemingly straightforward procedure, in the busy outpatient clinic strict adherence to these guidelines can be challenging to achieve. Discrepancies between recommended technique and usual care can have a significant impact on BP measurements and may result in patients being inappropriately classified as above goal.7
Barriers to adequate BP measurement in the outpatient setting include improper patient preparation, lack of appropriate training and knowledge by the staff performing these measurements, accuracy of selected BP measurement device (cuff size, automated vs manual), and workflow constraints such as perceived lack of time due to multitasking and need for multiple measurements.8–11 Clinic measurements may be significantly different from home BP readings or ambulatory BP monitoring (with home measurements typically lower than office measurements) making appropriate diagnosis and management of hypertension more challenging.10 12–14 Self-monitoring BP at home has some advantages compared with measuring BP in clinic including ability to get multiple measurements, vary the frequency of measurements and detect white coat/masked hypertension.14 15 However, it still requires appropriate equipment, technique, and a willingness from the patient to perform and document measurements. Despite concerns about the accuracy and limitations of in-clinic BP measurements, there are very few studies that address quality improvement strategies to effectively improve in-clinic BP measurements in the real-world setting.
Measurement
There were 4764 unique patients with type 1 or type 2 diabetes seen in the Michigan Medicine endocrinology clinic during the baseline period, which was defined as the 1-year period prior to the implementation of the intervention in Plan-Do-Study-Act (PDSA) cycle #1. See table 1 for baseline characteristics for this population.
Baseline demographics (n=4764)
BP measurements in clinic are performed by MAs who receive training on appropriate measurement technique. All BP readings were performed using a Device for Indirect Non-invasive Mean Arterial Pressure (DINAMAP). All BP cuffs are monitored and maintained for calibration by a centralised, biomedical engineering department. MAs used Epic EMR software to enter BP readings into the medical record after the initial and repeat measurement, if applicable. Results of all BP readings were extracted from the EMR via the Epic Clarity database in addition to the University of Michigan’s internal datamart. All extractions via queries were validated by the University of Michigan’s Quality Analytics group. BP readings were associated using unique visit encounter identification numbers. These encounters were then queried to pertinent patient level characteristics and provider information of the population. All data sources were merged into datasets using structured query language.
Please see table 2 for baseline measurements. If a patient was seen in clinic more than once during the selected time period only data from the most recent visit was used. During the baseline period, 70.6% of patients had a BP of <140/90 mm Hg on initial check in clinic. Of those patients with an elevated initial reading, 13.1% were rechecked by either the MA or the physician. When a patient had multiple readings taken at a single visit, our institution quality metric for BP captures the most recent BP reading. We, therefore, found that 72.5% of patients had their most recent BP at goal (ie, they only had one measurement taken and it was at goal or if they had multiple measurements the more recent measurement was at goal).
Percentage of clinic patients meeting blood pressure target
Design
A quality improvement project team consisting of three physicians, the MEND Clinic Manager, and a Project Manager from the Department of Internal Medicine Quality & Innovation Programme was formed to address BP measurement protocols. Additional stakeholders that were involved in the design and implementation of the PDSA cycles included pharmacy, MAs and nursing. The University of Michigan’s Quality Analytics group provided statistical support so that results could be analysed after each intervention cycle. The quality improvement project team met regularly during the course of the project. Updates were provided to physician faculty during division faculty meetings to alert them to changes in workflow and elicit feedback after each PDSA cycle. The QI project manager and clinic leadership educated MAs on new BP measurement protocols and during implementation provided weekly feedback on adherence to workflow. An assessment was done on current clinic volume and additional DINAMAP vital signs monitors had to be purchased in order to accommodate changes in workflow without delaying the rooming process.
Strategy
Interventions were performed across two PDSA cycles.
PDSA cycle #1
A new BP measurement workflow was implemented to better align clinic BP measurements with ACC/AHA recommended technique. Previously, BP was taken in the intake bays at the start of the rooming process at the same time as the HbA1C measurement. With the new workflow BP was moved to the end of the rooming process and patients would be seated/resting for 5 min prior to measurement being taken. We predicted that the new workflow would result in more patients meeting the BP target on initial measurement.
PDSA cycle #2
A new EMR best practice alert (BPA) was implemented in clinic to encourage repeat BP measurement when the initial reading was above target. When an MA entered a BP reading into the EMR encounter that was above the target of 140/90 mm Hg the alert prompted the MA to recheck the BP again prior to the end of the encounter with at least 5 min between the two measurements. Our baseline data collection had demonstrated that a significant percentage of patients with elevated initial BP measurements had lower readings on subsequent measurements. We, therefore, predicted that an intervention increasing the recheck rate would result in a greater percentage of patients meeting their BP target.
Results
Data were collected on 3244 patients seen in the 5-month period after PDSA cycle #1 After implementation of the new BP check workflow, 72.1% of patients had a BP of <140/90 mm Hg on initial check in clinic, which was not statistically significant. Mean systolic and diastolic BP was essentially identical before and after the intervention at 132/68 vs 131/68 mm Hg. When analysis was limited to only patients with a diagnosis of hypertension (as determined by EMR problem list), we found that fewer patients were at goal, but there was still no significant difference between the two time points (59.8% vs 62.5%).
Data were then collected on 3768 patients seen in the 6 months after the implementation of PDSA Cycle #2. During PDSA cycle #2 the implementation of an EMR reminder to recheck elevated BP readings in clinic did significantly increase the BP recheck rate in our clinic from 12.9% prior to the initiation of the BPA to 35.9% after the implementation of the BPA. Of the patients who had a repeat BP measurement taken, 48.6% of the time the second BP was in the goal range.
There was no significant improvement noted in the overall percentage of patients meeting their BP target after PDSA Cycle #1 (72.5% vs 73.3%). However, after PDSA cycle #2, there was a statistically significant improvement in patients with diabetes meeting the target from 73.3% to 76.8% (p<0.01). There was also a statistically significant improvement when the population was limited to those with a diagnosis of hypertension (62.2% vs 67.9%, p<0.01) . This change was driven by the increase in BP recheck rate with many patients coming into the goal range on their second measurement.
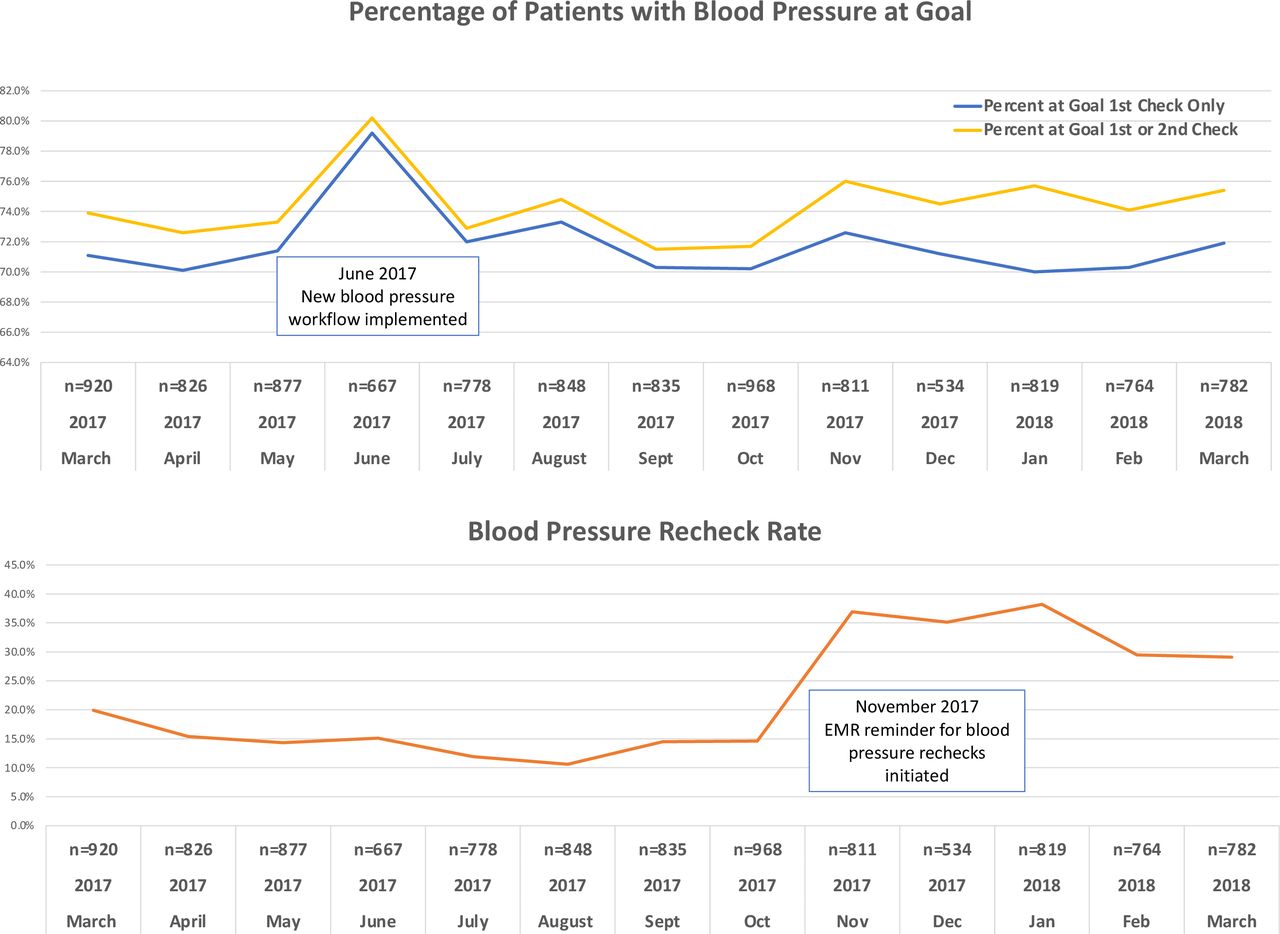
Please see figure 1 for BP results and rechecked rate on a monthly basis during the course of the project. We note there initially seemed to be improvement in the percentage of patients meeting the target BP in June when the first PDSA cycle was initiated, but these results were not sustained. The reason for the initial improvement and subsequent decline is not clear, especially as ongoing efforts from clinic leadership and the project manager confirmed continued adherence with the new protocol. The second PDSA cycle created a modest but sustained improvement over time in the BP recheck rate which in turn improved the overall number of patients at goal when both the first and second BP check are included.
{kind=link}
The blue line indicates the percentage of patients who met the blood pressure target when only the first blood pressure measurement is considered. The yellow line indicates the combined per cent of patients who met the blood pressure target on the first check plus those who did not initially meet the target but came down into the goal range on repeat measurement (second check). The per cent of patients with two or more blood pressure measurements recorded during their clinic visit (ie, blood pressure recheck rate) is shown in orange.
In order to ensure that patients with multiple high BP readings had close follow-up a pharmacist-led hypertension clinic was also created. Entry of an elevated BP measurement into the EMR queued an order set for the 2–4 weeks follow-up appointment with a clinical pharmacist that the physician could sign if appropriate. The clinical pharmacist is a PharmD who can review home BP measurements, educate patients on correct home BP measurement technique, assess adherence to therapy, address adverse effect or cost concerns, counsel on various lifestyle modification strategies to improve BP, make BP medication adjustments via protocol, and follow-up on electrolytes and other labs related to medication changes. The clinical pharmacist communicates recommendations with the physician after the patient visit. Clinical pharmacy appointments for hypertension, type 2 diabetes or hyperlipidaemia management and polypharmacy are available within all primary care offices across our institution, but were not previously an option for patients being seeing in the endocrinology specialty clinic. From January 2018 to June 2018, there were 42 patients seen in the PharmD clinic. However, this reflects only a fraction of the patients who were potentially eligible for referral suggesting this resource was underused.
Lessons and limitations
Reliable BP measurement is essential to appropriate hypertension management. In our first PDSA cycle, we adjusted the timing of BP measurement during the patient intake and rooming process such to allow the patient adequate rest time prior to BP measurement in accordance with ACC/AHA guidelines. This did not result in any significant change in the percentage of patients meeting their BP target, nor was there a change in the mean BP.
During our second PDSA cycle, we noted a large percentage (48.6%) of patients who had an initially elevated clinic BP reading came down to target when the measurement was repeated. Previous studies have indicated that a single clinic BP measurement is inadequate for assessing control due to significant within-patient variability.16 Our results similarly highlight the importance of having multiple BP readings in order to assess whether patients have their hypertension adequately controlled.
With the use of an EMR-based alert, we were able to increase the frequency of BP rechecks from 12.9% to 35.9%. However, this means that even with an EMR reminder, less than half of patients with high BP had a repeat measurement that was documented in the vitals section of the EMR. This result underscores how difficult it can be a busy outpatient practice to obtain multiple BP readings. Feedback from the MAs indicates that a common reason the repeat BP measurements were missed is that there was not time to repeat the measurement prior to the physician starting their visit, and they were hesitant to interrupt an in-progress physician encounter for repeat BP measurement. The BP could be repeated after the physician had completed their visit, but patients would often forget to stay to have the measurement retaken. Asking the physician repeat the BP measurement during the encounter could help solve this issue but would be challenging given physician time constraints. Furthermore, some physicians may have repeated the BP measurement themselves and documented it in the text of their clinic visit note, but unless it is entered into the vitals section of the EMR it is not captured by our quality improvement metrics. In order to address the continued suboptimal recheck rate the clinic is currently obtaining a BpTRU BPe monitor which takes multiple measurements automatically at intervals of 1–5 min.17 A future PDSA cycle is planned incorporating the BpTRU machine into existing workflows to see if the ability to take multiple measurements without a clinician or staff member present would increase the recheck rate without adversely affecting clinic flow.
Use of in home BP measurements or ambulatory BP measurements would address some of the limitations of in clinic BP measurements including reproducibility concerns.2 Multiple measurements could be taken without the time constraints of the busy outpatient clinic environment. This would also be useful in situations of suspected white coat hypertension. Currently, patient-reported home measurements are not included as part of the HEDIS controlling high BP performance measure and hence were not used as part of the primary outcome for this project. However, these readings could still prove useful to clinicians in our clinic for hypertension diagnosis and medication adjustment and thus could be incorporated in future quality improvement cycles. Feedback from physicians in our clinic suggest that many do encourage their patients to check home BP measurements and use this data to guide clinical decision making. Home BP measurement <140/90 mm Hg has been identified in the literature as a reason why providers many not intensify hypertension therapy despite high in clinic measurement.18
For patients with repeat high BP measurements, physicians were given the option to refer to a PharmD-led hypertension clinic. Forty-two patients were seen in this clinic from January 2018 to June 2018. This means only a fraction of eligible patients completed PharmD visits. In assessing reasons for this low rate we found that the physician signed the referral order only about ~1/3 of the time the EMR alert was triggered. There are various reasons why the order may have been dismissed by the provider. A few examples include missed doses of BP medication prior to that visit, a single elevated BP reading in a patient who has previously been well-controlled at visits or who reported in range home BP measurements, primary care follow-up already scheduled in between visits, or patient declining referral. Some patients were referred but never scheduled, and others scheduled, but later cancelled their visit. The PharmD hypertension clinic was limited to Friday afternoons based on clinic space and availability. The time slots available, living distance from the specialty clinic and lack of perceived importance may have been barriers for some patients. More patients and a longer follow-up period would be needed to determine if patients who attended PharmD clinic visits were more likely to have goal BP readings at their subsequent clinic follow-up appointments and also to address the long-term cost effectiveness of the PharmD hypertension clinic.
Conclusion
We found that increasing the BP recheck rate via an EMR alert resulted in a significant increase in the number of patients meeting their BP target in an outpatient diabetes clinic. A significant percentage of patients with an initially high BP measurement came down into goal range on repeat check suggesting that the use of a single measurement may be inaccurate and result in overtreatment. The timing of initial BP measurement during patient intake did not have a significant effect. Further work is still needed to ensure the consistency and accuracy of in clinic BP measurements and to improve follow-up of elevated in clinic readings. Our results may be of interest to other outpatients clinics and health centres seeking to improve in-clinic BP measurement.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
The project was submitted to the Institutional Review Board of the University of Michigan and was deemed non-regulated as a clinical quality assurance activity (HUM00127059).
Acknowledgments
We would like to thank the Michigan Medicine Quality Department for providing statistical support for this project.
References
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors JW initiated the project and designed the interventions used in the PDSA cycles. MJ served as project manager. He oversaw the implementation of the PDSA cycles in the clinic and worked with clinic leadership to ensure staff had appropriate training in new protocols and workflows. MJ also worked with Quality Analytics to extract the data. JJI assisted with the implementation of the PDSA cycles, communicated results of each cycle with faculty to elicit feedback and performed the data analysis. JJI also took the lead in writing the manuscript. JEF worked with the project team to initiate the follow-up hypertension clinic and served as the PharmD of the clinic. She wrote sections of the manuscript pertaining to the hypertension clinic. SK was part of the project team and assisted with the design and implementation of the PDSA cycles and wrote the background portions of the manuscript. Each of the authors has revised and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.