Article Text

Abstract
Hospitals within the UK are paid for services provided by ‘Payment-by-Results’. In a system that rewards productivity, effective collaboration between coders and clinicians is crucial. However, clinical coding is frequently error prone and has been shown to impact negatively on departmental revenue. Our aim was to increase the median number of diagnostic codes per sickle cell inpatient admission at Guy’s Hospital by 3. Three interventions were implemented using the Plan, Do, Study, Act structure. This consisted of student doctors searching for diagnoses along with comorbidities that clinical coders had missed, distributing laminated cards with common clinical codes and implementing discharge pro formas. Through auditing, student doctors generated a total of £58 813 over 16 weeks. We observed an increase in the median number of codes by ≥2 additional codes. We improved coding accuracy where we identified errors in an average of 32.5% of admissions each month, improving the quality of patient documentation. We have demonstrated student doctor involvement in clinical coding as a potentially sustainable means of achieving accurate payment for services provided; increasing departmental revenue. We are the first to report the efficacy of student–coder collaboration in improving the accuracy of clinical coding.
- PDSA
- quality improvement
- medical education
- cost-effectiveness
- teamwork
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Hospitals within the UK are paid for services provided by ‘Payment-by-Results’. This is a system envisioned to allow for greater transparency, where clinical coding is intended to provide an accurate summary of a patient’s stay.1 Patient information is converted into diagnostic codes by clinical coders at discharge. The codes for any diagnoses, comorbidities and complications are found in the International Classification of Diseases Version 10 (ICD-10) while investigations, procedures and treatments are in the Office of Population Censuses and Surveys Classification of Interventions and Procedures Version 4.8 (OPCS 4.8). This information is then used to assign a patient’s healthcare resource group (HRG) code, which determines the tariff the hospital receives for services provided. These nationally set tariffs are allocated on a cost-per-case basis and provide a clear financial and managerial incentive to code accurately.2–4
The haematology department within Guy’s and St Thomas’ NHS Foundation Trust (GSTT) was identified as having poor coding of inpatient admissions. Clinical coders at GSTT use electronic discharge letters (EDL) along with electronic clinical notes (software: e-Noting and electronic patient record (EPR)) to generate HRG codes for each patient. EPR is used to list diagnoses which informs healthcare professionals of important conditions, comorbidities and previous surgeries. On the other hand, e-Noting acts as a clinical diary of a patient’s stay where a clinical log is made every time a healthcare professional makes contact with the patient.
Previous studies have shown that discharge summaries used in tandem with clinical notes and effective clinician–coder collaboration improve the accuracy of clinical coding and departmental renumeration significantly.5 6 However, clinical coders highlighted the practice of only using EDLs and electronic clinical notes as a contributory factor to the poor quality of coding. This is because patients with sickle cell disease often have long patient stays and reading each entry can be excessively time consuming.
The interaction between coders and doctors is crucial to ensuring effective coding. Coders rely on accurately completed EDLs with all relevant diagnoses listed, particularly as they are not allowed to interpret results or vague notes. On the other side, the completion of comprehensive discharge summaries is time intensive and doctors are often unfamiliar with how to write summaries that ensure accurate payments for services provided.
This quality improvement project (QIP) was undertaken by student doctors liaising with clinical coders and clinicians at the haematology department of a large tertiary hospital—Guy’s Hospital, GSTT. The aim was to increase the median number of diagnostic codes per sickle cell inpatient admission by 3 and increase the departmental revenue by £10 000 per month.
Background
Discharge summaries are vital for an accurate transfer of information between healthcare professionals from tertiary to primary care settings. However, inconsistencies in the comprehensiveness of EDLs are a well-reported issue, where the degree of omission of important patient information varies between hospital trusts and specialties.7 Inaccuracies and inadequate transfer of information have been shown to contribute significantly to preventable adverse events in patients after discharge.8 This compromises the provision of care and prevents accurate coding.9
Our project sought to achieve improvement in three areas—accuracy of clinical coding, EDLs and departmental revenue. Studies have shown that clinician involvement in identifying missing diagnostic codes improves the accuracy of coding, demonstrating a significant positive financial impact.6 10 11 However, there has been a focus on coder–coder and clinician–coder auditing, with some arguing that collaborative efforts should be led by senior clinicians as opposed to junior doctors.6 We sought to establish whether medical student-led auditing could improve the accuracy of coding, thereby improving discharge summaries and generating income for the trust.
Baseline measurement
A 2-month baseline was undertaken. The number of ICD-10 and OPCS 4.8 diagnostic codes of all sickle cell inpatient admissions was counted using the coding database and a median calculated. Our inclusion criteria were all inpatient lengths of stay of ≥1 day with sickle cell anaemia with or without crisis (ICD-10 codes: D750 and D751). We excluded short-stay and outpatient admissions on the basis that they are subject to different tariff algorithms. This was carried out at the haematology department at Guy’s Hospital in London. The results showed that the median diagnostic depth for inpatient admissions in July and August 2018 were six codes. This outcome measure was used in subsequent audits after each Plan, Study, Do, Act (PDSA) cycle.
Design
Our aim was to increase the number of diagnostic codes recorded per inpatient admission by three additional codes over the baseline by February 2019 to a median of nine codes. This target was set after analysing the number of diagnostic codes each patient was allocated within our baseline measurement. The distribution showed that nine was a specific, measurable, achievable, realistic and timely goal. By improving the accuracy of clinical coding, we predicted our interventions would increase departmental revenue by £10 000 per month. This was the minimum expected based on a previous consultant-led initiative which increased remuneration in haemato-oncology patients within the haematology department at Guy’s Hospital; we used these data to inform our predictions.
The team consisted of medical students in MBBS Year 4 completing their QIP module, clinicians from the haematology department (grades: Foundation Year 2 to consultant), physician’s associates and a lead clinical coder from the GSTT coding department. This large collaborative team allowed us to identify salient issues that were impacting the quality of coding of patients with sickle cell and develop sustainable strategies to combat this.
The baseline measurement, data collection and analysis were carried out by student doctors and a clinical coder. The inclusion and exclusion criteria were set by the clinical coder. The results were presented back to the team at the end of each month. This facilitated further discussion on our strategy for the next intervention.
The project design was informed by our baseline measurement and discussions with the multidisciplinary team. We recognised that time constraints for both clinical coders and doctors were a significant factor. Writing comprehensive EDLs is often difficult for doctors on busy shifts. Clinical coders have strict deadlines and cannot search through electronic notes to find all diagnostic codes that have been omitted from EDLs. Moreover, there was a lack of awareness among doctors of the diagnostic codes that impact tariff, presenting educational opportunities.
Three interventions were devised and implemented; our first intervention centred on alleviating the burden on clinicians and coders while the rest were to raise awareness and improve the quality of EDLs. Each intervention lasted a minimum of 4 weeks with a focus on ensuring a sustainable, cost-effective impact.
Strategy
PDSA cycle 1 - 1 September 2018 (1.9.18)
Plan: This cycle aimed to improve the accuracy of clinical coding, where student doctors searched for diagnoses and comorbidities that had not initially been coded due to omission from EDLs. The codes and tariffs were correct at the time of coding.
Do: Using inclusion and exclusion criteria set by the clinical coder, we audited the inpatient stays of all patients with sickle cell anaemia during September and October 2018. For each inpatient stay, we analysed the electronic patient notes (EPR and e-Noting) to identify code descriptions that were omitted from the EDLs including: primary and secondary diagnoses, comorbidities, body mass index, allergies, blood test results, imaging and treatment (medication, physiotherapy, mental health, spiritual care, occupational therapy). To reduce variability in data collection, student doctors devised and systematically followed a checklist to find missing terms. Random crosschecks were performed. The clinical coder validated the data, ensured its accuracy and converted the descriptions into classification codes, thereby generating further income for the trust.
Study: From this intervention, we generated £13 722 in September and £30 581 in October. The median number of diagnostic codes consistently exceeded the baseline by ≥2 codes. We reached our goal four times. The results provided us with an insight into the diagnostic codes that were commonly missed from EDLs (figure 1), and we used this to design our second intervention. Due to the efficacy of this intervention, we completed this process after each PDSA cycle to establish whether it was a sustainable measure.

The most frequently missed diagnoses and comorbidities in electronic discharge letters (EDL) in September and October from medical student involvement (Plan, Do, Study, Act; PDSA 1). Abnormal blood tests included the following codes: hyperkalaemia, deranged liver function tests, transaminitis, abnormal white cell count, disordered phosphates and hypocalcaemia. CRP, C-reactive protein.
Act: From PDSA 1 we confirmed that diagnostic codes were being missed and quantified the impact this had. Building on this learning, we developed our change idea for PDSA 2.
PDSA cycle 2 - 17 December 2018 (17.12.18)
Plan: We designed laminated cards to raise awareness into the diagnostic codes that were frequently missed from EDLs (online supplementary figure 1). We used data from our first PDSA cycle to inform the design, where the lead clinical coder provided us with the diagnostic terms that were added after student auditing in September and October. We hypothesised that the cards would act as an aide-memoire helping clinicians remember to include these diagnostic terms in EDLs, and hence be more readily coded by clinical coders.
Supplemental material
Do: The laminated cards were distributed among the whole haematology department and were attached to clinicians’ lanyards.
Study: They were well received and adopted by all doctors working within the haematology department. However, there was no improvement in the coding of frequently missed diagnostic terms.
Act: Building on PDSA 2, we recognised that although we had increased awareness, we needed to put this into practice and thus designed our final cycle.
PDSA cycle 3 - 11 January 2019 (11.1.19)
Plan: Having received positive feedback on PDSA 2 from clinicians, this cycle served as an adjunct to the laminated cards. We designed a discharge letter pro forma to improve the quality of EDLs (online supplementary figure 2). The template served to ensure that the structure and content of discharge summaries were consistent, providing a comprehensive summary of the patient’s stay. We reasoned that this would make it easier for clinicians to document all relevant information, including the frequently missed terms, therefore improving the quality of coding.
Do: The discharge letter pro forma was used by the physician’s associate and clinicians. Study: We repeated our first PDSA cycle to ensure diagnostic terms had not been missed. We measured the number of diagnostic codes.
Act: The discharge pro forma showed no clear effect and was abandoned.
Results
Our main outcome measure was the median number of diagnostic codes per patient, which was collected from the coding database. To assess normal variation, we established the preintervention baseline from the median diagnostic depth of all inpatient admissions in July and August 2018. This equated to a median of six codes per patient. We set a goal of increasing this to nine codes. Data were thereafter collected over a 16-week period to generate a run chart (figure 2).
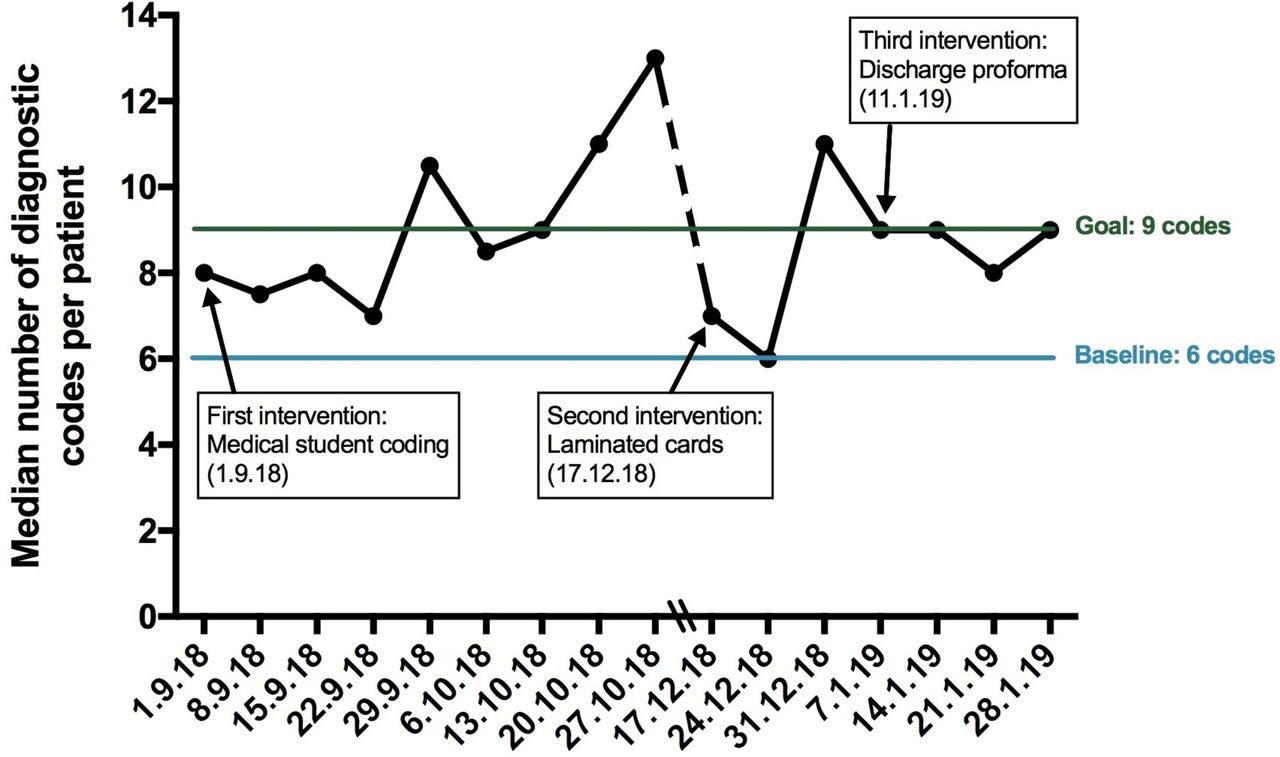
Run chart showing the median number of diagnostic codes per patient over a period of 16 weeks. The baseline measurement was calculated using the median number of diagnostic codes in July and August 2018, which equated to six codes. Our aim was to increase this by three additional codes to nine codes.
Following the implementation of the first intervention, we reached our goal of a median of nine codes per patient on eight occasions. However, this was only maintained over 3 consecutive weeks. Despite this, results show an overall improvement in the coding of patients with sickle cell where we observed an increase in the median number of codes by ≥2 additional codes. This occurred on 12 occasions and moreover persisted over 5 consecutive weeks.
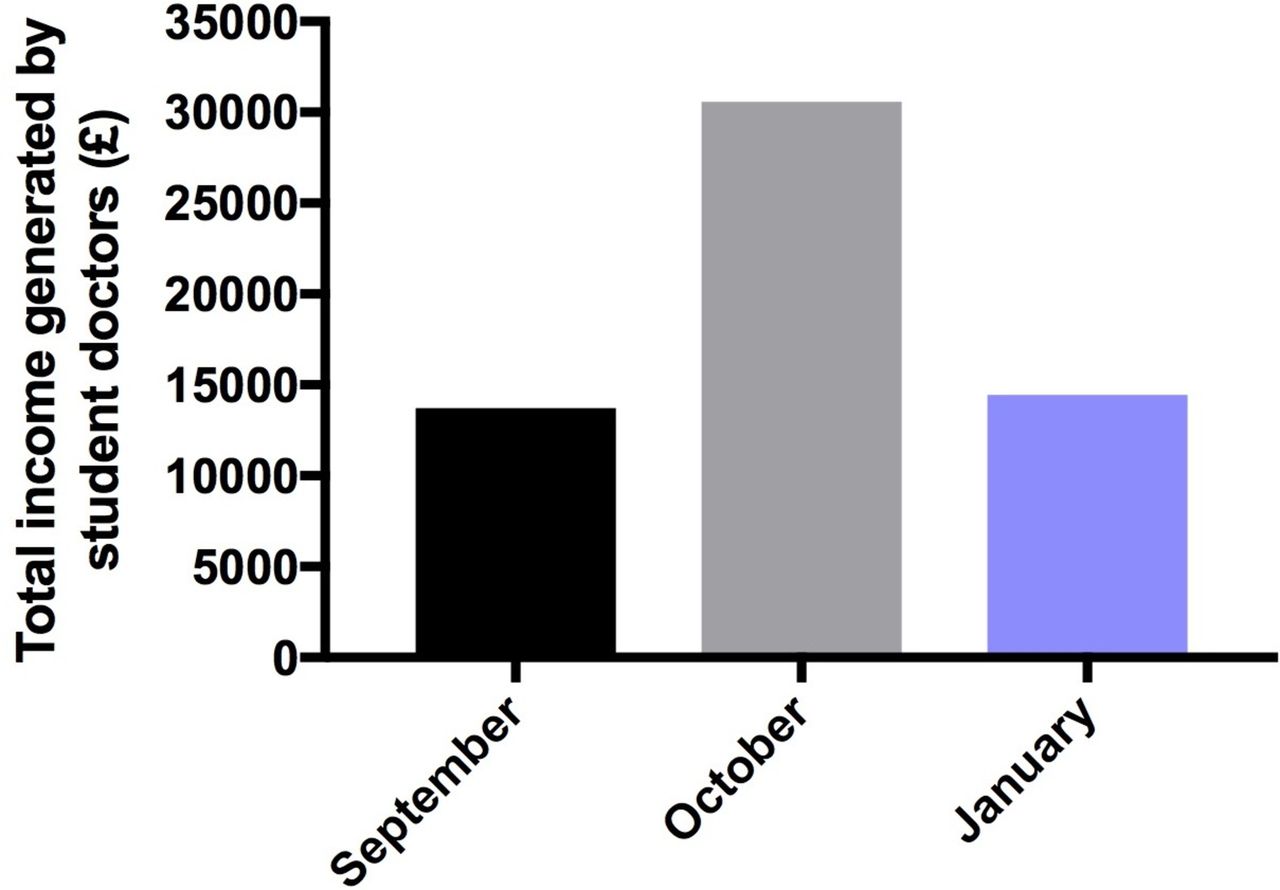
Results have shown that medical involvement increased the total departmental revenue, which was sustained throughout the project (figure 3). We generated a total of £58 813 over 16 weeks; September (£13 722), October (£30 581), December (£81) and January (£14 429).

{kind=link}
{kind=link}
{kind=link}
Total income generated by medical students for the haematology department from identifying missed diagnostic codes.
The introduction of our second and third interventions showed no clear effect. Medical students remained able to identify missing diagnoses and comorbidities (online supplementary figure 3), generating income consistent with previous revenue (£13 722 in September vs £14 429 in January). Furthermore, we identified that the error rate for coding remained consistent during the project at an average of 32.5% of total admissions per month. In total, 60 patients were recoded out of a sample size of 158.
We observed special cause variation from 17 December to 31 December, coinciding with the holiday season. The number of admissions and lengths of stay was significantly reduced compared with other months. This is further supported by the overview of the financial income the haematology department receives for patients with sickle cell on a monthly basis (online supplementary figure 4), where the departmental revenue in December is considerably lower.
Lessons and limitations
We recognised that a simple intervention of student doctors thoroughly checking clinical records improved the accuracy of coding, amounting to a significant positive financial impact. The average error rate for the clinical coding of patients with sickle cell was 32.5% each month. This is notably higher than the national average of 15.3% for inpatient admissions.12 We determined that this was mainly due to EDLs not being comprehensive. This consequently leads to clinical coders meticulously searching EPR and e-Noting for diagnostic codes—both inefficient and time consuming. This pressure is compounded by strict deadlines that must be met every calendar month.
Based on our learning from PDSA 1 we attempted to improve the documentation of codes in EDLs through implementing laminated cards and discharge pro formas. However, they produced no clear improvement in the quality of clinical coding . Impact on departmental renumeration is more challenging to elucidate. The revenue is based on a complicated algorithm and several factors can affect the tariff. This includes, but is not limited to, a patient’s age, length of stay and their comorbidities. For this reason, we cannot detail how commonly missed codes impact the HRG. In some patients, adding a particular code may increase the tariff, and in other cases the tariff may remain the same.
Student doctor–coder collaboration consistently led to the addition of diagnostic codes throughout the project (online supplementary figure 3). This was the only intervention out of the three PDSA cycles that was successful and was adopted by the department.
Despite raising awareness and receiving excellent feedback from the haematology department, it is time-consuming writing comprehensive EDLs that encompasses all conditions a patient presents with. Studies have attempted to improve the quality of EDLs using a combination of a discharge pro forma alongside an automated process that inserts specific elements of patient data, such as allergies.13 For these reasons, initiatives are currently under way in improving the software at GSTT. There is a motion to introduce an easy-to-use grid interface that allows clinicians to tick off diagnostic terms during a patient’s stay, thereby improving the documentation of inpatient admissions.
It is evident that Payment-by-Results rewards efficiency and productivity where there is a clear financial incentive to code accurately. This can only be achieved through effective coder–clinician collaboration. However, clinical coding is frequently error prone14 and has been shown to impact negatively on financial income in hospitals around the UK.6 11 12 From this QIP, the results raised questions into whether other specialties at GSTT are struggling to code accurately. Our first intervention produced a significant increase in departmental revenue, generating £58 813 in a small, targeted sample of patients with sickle cell (n=158) over only 16 weeks. One can hypothesise that continued student doctor involvement over a full calendar year could generate over £150 000 for patients with sickle cell alone. There is profound financial potential and we plan on expanding our intervention to other departments.
The process of auditing clinical notes for missing diagnoses and comorbidities in patients that have already been coded, as a means of improving coding accuracy, has been reported before. Clinician–coder and coder–coder collaboration has been encouraged,6 11 with an emphasis on consultant-led involvement. We are the first to report the effectiveness of student doctor involvement in improving the quality of clinical coding.
Recruiting student doctors is cost-effective and allows for trainees to gain an appreciation of the importance of clinical coding early in their careers. We now recognise the significance of writing comprehensive EDLs, which will shape the way we practice medicine in the future. The data collection furthered our knowledge of clinical medicine as we have gained a thorough understanding of sickle cell disease, including common comorbidities and management.
Our impact on local systems led to the establishment of three initiatives to drive an improvement in clinical coding at GSTT. The haematology department has included our intervention in their business plan. Clinical coders are recruiting medical students to join the NHS staff bank at GSTT, an entity that offers approved healthcare workers temporary and part-time work opportunities. This acts as a financial incentive, allowing students to take up paid shifts on a flexible basis. Lastly, coding projects will continue to be offered as an assessed module as part of the MBBS Year 4 QIP curriculum.
Conclusion
Student doctors generated £58 813 in revenue to the trust, demonstrating that auditing clinical notes is an advantageous strategy to ensure accurate remuneration for clinical services provided. The median diagnostic depth consistently exceeded the baseline, reaching our target on various occasions. We improved coding accuracy where we identified errors in an average of 32.5% of admissions each month leading to an improvement in the quality of patient documentation.
To ensure this intervention is sustainable, we aim to offer student doctors paid jobs through the local staff bank to audit inpatient stays. Furthermore, clinical coding projects will continue to be offered as part of the assessed QIP module in MBBS Year 4 at King’s College London, allowing student doctors to develop skills in project design, teamwork and sustainability in quality improvement. This comes with the additional benefit of raising awareness into the importance of clinical coding early on in a student’s career and further their understanding of clinical medicine through the auditing process. To further improve the quality of clinical coding, future efforts should focus on collaborative work between clinicians and clinical coders to create a user-friendly, easily operable interface to expedite the recording of clinical information in electronic note systems.
Acknowledgments
We are grateful to the haematology department at Guy’s Hospital for their unwavering support and cooperation. Special thanks to Dr Jo Howard for her kind support and guidance. To Dr Paula Busuulwa for kindly reviewing the manuscript and for helpful discussions. To Dr Matthew Streetly, Dr Caroline Spencer and Miss Deborah Sealy for their insight and helpful discussions.
Footnotes
SA, NS and KW contributed equally.
Contributors SA, NS and KW devised the project and collected and analysed the data after every intervention. MO assisted with data collection at some timepoints. CH, the lead clinical coder, revalidated all of the coding data and made substantial contributions to the design and methodology of this project. SA, NS and KW designed and implemented the laminated cards. SA, NS and LRH designed and implemented the discharge pro forma. GCS, the clinical lead of quality improvement (QI), oversaw the project. SA, NS and KW wrote the manuscript. SA and GCS contributed significantly to the revision of this manuscript. All authors reviewed and commented on the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.