Article Text

Abstract
The COVID-19 pandemic has infected tens of millions of people worldwide causing many deaths. Healthcare systems have been stretched caring for the most seriously ill and lockdown measures to interrupt COVID-19 transmission have had adverse economic and societal impacts. Large-scale population vaccination is seen as the solution.
In the UK, a network of sites to deploy vaccines comprised National Health Service hospitals, primary care and new mass vaccination centres. Due to the pace at which mass vaccination centres were established and the scale of vaccine deployment, some sites experienced problems with queues and waiting times. To address this, one site used the Lean systematic improvement approach to make rapid operational improvements to reduce process times and improve flow.
The case example identifies obstacles to flow experienced by a mass vaccination centre and how they were addressed using Lean concepts and techniques. Process cycle times were used as a proxy metric for efficiency and flow. Based on daily demand volume and open hours, takt time was calculated to give a process completion rate to achieve flow through the vaccination centre.
The mass vaccination centre achieved its aim of reducing process times and improving flow. Administrative and clinical cycle times were reduced sufficiently to increase throughput and the number of queues and queueing time were reduced improving client experience.
The design and operational management of vaccination centre processes contribute to client experience, efficiency and throughput. Lean provides a systematic approach that can improve operational processes and facilitate client flow through mass vaccination centres.
- lean management
- COVID-19
- vaccination
- continuous quality improvement
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The COVID-19 pandemic has infected tens of millions of people worldwide.1 Healthcare systems have experienced extreme pressure caring for the most seriously ill and globally, at the time of writing, over four million people have died following infection.1 2 Furthermore, social distancing and lockdown measures adopted to interrupt transmission of the virus have had significant economic and societal impact.3 As vaccines become available, large-scale population vaccination is seen as the solution.4 5
Mass population vaccination is logistically complex.4 In addition to behavioural resistance and vaccine hesitancy,4 6 production supply chains, international distribution and the capacity of healthcare systems for local dispensing have been identified as requiring attention and planning.4 6 7 For rapid deployment, improvised mass vaccination centres may be required—at least in the short term.6
In the UK, the Department of Health’s COVID-19 Vaccines Delivery Plan established a network of sites to deploy vaccines comprising hospital hubs, local primary care sites and mass vaccination centres.8 By end March 2021, almost 1700 sites were reported as operating—of which, 158 were mass vaccination centres.9
However, due to the pace at which mass vaccination centres were established, and the rapid increase in scale of vaccine deployment, some sites experienced problems with queues and waiting times.10–13 One site in Northern England used the Lean systematic improvement approach to make rapid operational improvements to reduce processing times and improve flow at a National Health Service (NHS) mass vaccination centre.
Background
Mass vaccination centres are large-scale venues in communities, such as sports stadiums, repurposed to vaccinate large numbers of the local population.8 They complement other vaccination sites such as hospital hubs and primary care sites. Hospital hubs have utilised NHS trust facilities and focused on vaccinating health and care staff as well as initial roll-out of vaccines to ensure any clinical and safety issues are identified and managed. Local primary care sites mobilised general practices and community pharmacies to focus on the highest risk individuals and those unable to attend vaccination sites. Mass vaccination centres are a new approach in the NHS that offer a high-volume alternative to hospital and primary care services. They provide convenient locations and extended hours with appointment slots that can be booked via the National Booking Service (NBS). Mass vaccination centres are part of the UK Government’s strategy to roll-out COVID-19 vaccination to the entire population at pace.8
Mass vaccination centres operate to national protocols.14 15 As vaccines are prescription-only medicines, there are specific legal mechanisms under which they can be administered—that is, signed prescriptions; patient-specific directions; patient group directions; and national protocols. National protocols are new legal instruments that support vaccination campaigns (influenza and COVID-19) by allowing a broader range of staff to safely administer authorised vaccines, including those who are not registered healthcare professionals.14 Such protocols provide flexibility to split the vaccination process into its component parts across multidisciplinary teams (comprised of various clinical and non-clinical professionals from various seniority levels)16 setting out the competency and professional registration requirements of each stage (eg, clinical assessment and consent, vaccine administration).14 15
Initially, seven mass vaccination centres were established.8 As new mass vaccination centres opened, some experienced overbooking due to a malfunction with the NBS that has been reported widely in national and local press.10–13 The case study presented here was one such site.
The case took place at a mass vaccination centre in northern England situated within a community of c150 000 people. As the vaccination centre went live, problems with the NBS led to long waiting times and queues with clients expressing their dissatisfaction directly to staff at time of attendance and indirectly via social media. While the site team made operational changes on the day (such as creating additional, socially distanced queuing space), the experience alerted them to how easily queues could build due to imbalances in the centre’s processes (see measurement section below). A project was established to reduce queuing time and improve throughput at the centre.
As the project was being established, a member of the mass vaccination centre team was invited to join a national online programme, Lean Fundamentals, which introduced foundational improvement concepts from the Lean approach.17 Lean has its origins in Japan’s automotive industry. It is a systematic quality improvement approach based on two core values—to make client value flow and respect for people.18 Lean achieves this by conceptualising work as processes that can be continuously improved.19 In healthcare, this emphasises the centrality of clients (usually patients) to all activities and aims to reduce or eliminate processing time that does not add value to the client.20 In practice, this is achieved through the application of Lean’s five operational principles: defining client value; mapping the client journey (value-stream); making the client journey (or value-stream) flow; designing processes that ‘pull’ value towards clients as needed; and pursuing perfection through ongoing continuous improvement.19 21 Developed by NHS England and NHS Improvement’s (NHSE&I’s) Improvement Capability and Delivery (ICBD) team, Lean Fundamentals is a technology enhanced learning programme to support operational managers to implement process improvements using Lean.17 A highly practical programme, it comprises six, 1-hour content modules available 24/7 over an 8-week period to support operational managers to make rapid process improvements.17 The Lean Fundamentals online programme was adopted to support the mass vaccination centre’s project and improvement aims.
Measurement
Kollberg’s framework provides a set of proposed metrics for measuring Lean improvement initiatives in healthcare. The framework aligns metrics with the Lean principles to measure aspects of value, value-streams, flow, pull and perfection. Proposed metrics include: volume of demand; client satisfaction; process times; number of queues; and staff improvement suggestions.22
Due to the initial problem with the NBS allowing overbooking, the vaccination centre had an urgent need to improve flow through the vaccination process. Lean aims to improve process flow by analysing the steps in a client pathway (value-stream) and then reducing and balancing processing time across the cycles in the pathway.22 23 By reorganising processes in this way, non-value adding time can be eliminated and tasks redistributed to create more efficient, flowing processes.21 Therefore, baseline measurement captured process cycle time data for a sample of clients at each process step in the vaccination centre—security and bag check, administration, clinical assessment and vaccination.
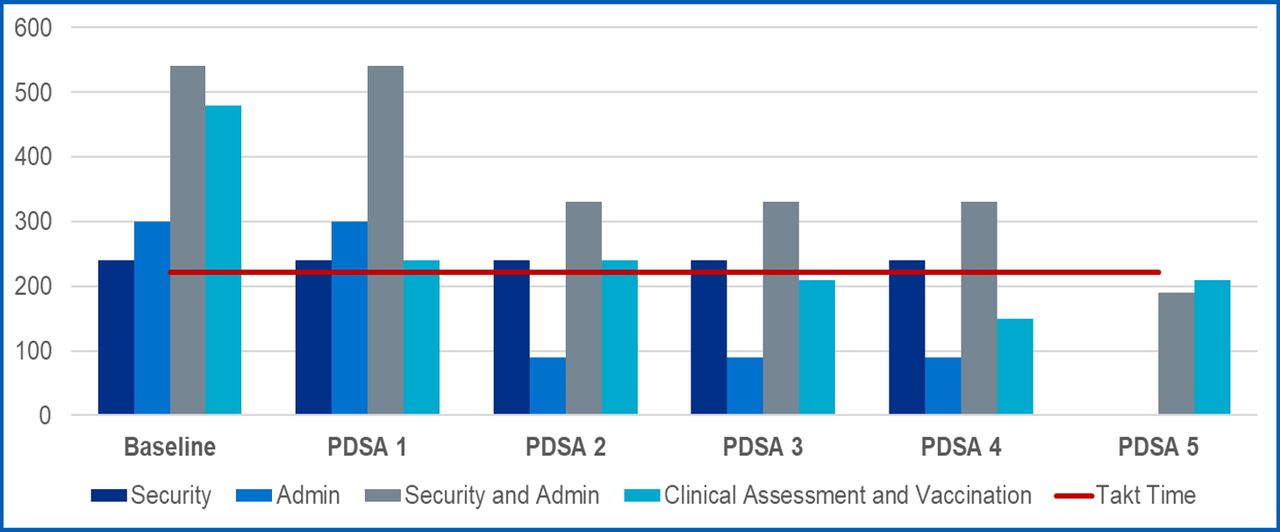
The daily demand at the vaccination centre on opening was for 1560 injections (560 more than the 1000 the centre was expected to deliver). With the centre’s opening hours of 08:00 am to 20:00 pm, this implied a completion rate for vaccinations of one every 28 s. With eight vaccination lanes available, each lane required a completion rate of one every 222 s (roughly one every 3 and half minutes). Figure 1 shows the baseline measurement for each process cycle compared with the required completion rate for each vaccination lane—shown as the red horizontal line and typically referred to as ‘takt time’ in the Lean lexicon.24

Baseline condition of vaccination centre process cycle times (seconds).
Design
The improvement process was supported by the Lean Fundamentals online programme. Lean Fundamentals provided accessible knowledge transfer on Lean techniques and a structured improvement routine through which they could be deployed.17 The structured improvement routine utilised ‘improvement kata’ drawn from the Lean improvement practices of Toyota.25 26 The improvement kata routine comprised four steps: understand the direction and challenge; grasp the current situation; establish the next target condition; and experiment towards the target condition.25 26
The first step established a clear improvement aim linked to an organisational priority.17 25 26 In this case, the organisational priority was to provide timely vaccination and, therefore, the aim was to reduce process time and improve flow.
The second step used various process analysis techniques to study the current state in detail.17 25 26 This involved the use of Lean process analysis tools, which included: a ‘waste-walk’—which is an observational study to identify obstacles to delivering client value such as bottlenecks and delays in the process; cycle time observation—which involves capturing the individual process times (cycle times) for a sample of patients at each process step; and flow process analysis—which uses cycle time data and sketching the various flows of healthcare (patients, families and carers, staff, medication, equipment, supplies and information) to create visual representations of the overall process flow.27–30
The third step articulated a series of target conditions for how processes should operate to achieve the aim and deliver client value (in this case, value being timely receipt of vaccination).17 25 26 The final step applied successive iterations of plan-do-study-act (PDSA) experiments to achieve each target condition and the overall improvement aim.17 25 26
Strategy
The intervention strategy utilised Lean. Due to the initial overbooking issues with the NBS and the consequent delays, the team operating the vaccination site considered rapid changes that could be made to speed up the process and alleviate the situation. Observation of queues and timing of process cycles were used to identify bottlenecks. This identified that the front-end administrative process was averaging 4 to 6 min per client to complete. Clients then moved to the clinical assessment process that was averaging 5 to 7 min to complete. Following clinical assessment, clients moved to the vaccination process that was averaging 2 min to complete. The process times were clearly unbalanced (as illustrated in the baseline condition in figure 1) leading to too many queues and too many people waiting for the next step in the process.
The first target condition was to reduce the number of queues and decrease processing time. The first PDSA experiment involved a rapid, real-time change to the process, which combined the clinical assessment staff with the vaccination staff to work together as a team in each point-of-dispensing (POD) area. This created several positive impacts. First, by combining the two processes, one queue was immediately eliminated. Second, having the clinical assessors and vaccinators work together as teams reduced the overall process time. Whereas in the baseline condition, clinical assessment and vaccination were averaging 6 min and 2 min, respectively, the new combined process was averaging 4 min in total (approximately half the time). Third, by combining the two processes, floor space was released, which provided more socially distanced queueing—though still insufficient to accommodate all waiting clients. As the focus cohort for vaccination at the time comprised the more elderly and vulnerable, and the winter weather was cold and inclement, the next target condition was to provide additional, sheltered but socially distanced and well ventilated queueing space. This was achieved by contacting the building owner who had donated space to the vaccination effort to request additional space be opened and reconfigured to accommodate socially distanced, queueing.
With socially distanced queueing at the front-end of the process addressed, the next target condition was to further reduce this queue. The team focused on the initial administration process. Part of the previous experiment to combine clinical assessment and vaccination roles had reallocated some administrations tasks, previously carried out by clinicians, to administrators in the administration process. While this worked to reduce the overall clinical/vaccination process times, it added time and complexity to the administration process in which clients were received. In addition to checking client bookings against the NBS, administrators also now entered data to a secondary national data collection system (Pinnacle). Through observation and discussion with the administrators, the team aimed to identify easier methods for moving between the two systems and capturing the required data. PDSA experimenting identified a ‘split screen’ approach and work sequence that was both easier and more timely to complete—reducing the new administration process, on average, to one and a half minutes. This had the desired impact of processing clients through the front-end queue more quickly.
However, with clients now entering the system more quickly, pressure started to build again on the clinical assessment and vaccination PODs. The next target condition was to improve the flow between administration and clinical assessment/vaccination. PDSA experiments looked at changes to the POD process. Trials included clinicians carrying out the assessment questions with clients and vaccinators supporting them by capturing the required responses in the computer system ready for clinical checking and sign-off before giving the vaccine. The impact of these trials was to reduce the average clinical assessment/vaccination process time to under three and a half minutes. While the improvement reduced clinical assessment and vaccination time to a rate sufficient to deliver 1500 vaccines per day through eight PODs over a 12-hour shift, it still left a queue to be managed between administration and clinical POD. The next target condition was to create the best flow between the two processes.
The next PDSA experiment involved moving the administration process as close as possible to the clinical POD. However, within only 30 min, it was clear this was adversely affecting the flow and causing stagnation and queue build up. The next experiment then did the opposite and moved the administration process away from the clinical POD to accommodate a socially distanced, first-in-first-out (FIFO) queue for clients completing administration. As the clinical PODs were now the constraint that set the flow rate for the vaccination centre, the FIFO queue acted as a buffer to keep the clinical PODs operating at full capacity and so maximise the number of clients that could be processed. Therefore, the next target condition considered how to add value to clients in the prevaccination FIFO queue. This involved experimenting with provision of information about the clinical assessment and vaccination process. This took the form of both printed media, such as posters, and staff (clinical and non-clinical marshals) who could address any questions clients may ask. As any questions clients may have had were already answered and addressed in the FIFO queue, the impact was to further reduce the clinical assessment and vaccination processing time to an average of two and half minutes.
As initial improvements had focused on the administrative and clinical processes, the security check process on arrival had become the bottleneck. Therefore, security became the focus for the next target condition. The team noticed that clients were required to effectively check-in twice—once at security and then again at administration to verify their NBS booking. A PDSA experiment tested combining aspects of the security and administration processes. This involved bringing forward the NBS booking verification to run concurrently with security and bag checks. Additional data required for entry to the Pinnacle system was moved into the clinical PODs. As Pinnacle was already used in the PODs as part of clinical assessment and vaccination, and because processing time had already been much reduced, it was possible to accommodate this task within the required takt time. The outcome of the test was a two-step process for administrative check-in and security (averaging just over 3 min) and clinical assessment and vaccination (averaging three and a half minutes).
Following each round of PDSA experimenting, proposed changes were confirmed with clinical system vaccination operation centre leads for compliance with the centre’s protocol before implementation.
Results
The mass vaccination centre achieved its aim of reducing process times and improving flow. Across five cycles of PDSA experimentation, total processing time was reduced by more than half. Table 1 below summarises average process cycle times for the baseline condition and following each round of PDSA experimentation.
Process cycle times for baseline condition and post PDSA experimentation (seconds)
The number of queues and queueing time were reduced. By combining the clinical assessment and vaccination processes as one multidisciplinary team process within the clinical PODs and combining the security and administrative check-in process, two queues were eliminated from the process flow. Combining the processes and redesigning the distribution of tasks between administrators, clinical assessors and vaccinators both reduced the processing time (thus speeding up client flow) and created a more even balance of work across processes (thus creating a smoother flow with shorter wait times in the remaining queues).
Furthermore, administrative and clinical cycle times were reduced sufficiently to meet a takt time that could deliver 1500 vaccinations per day over a 12-hour shift (see figure 2 below). Alternatively, the centre could deliver its target number of vaccines in a shorter working day or with fewer open lanes. This gave the centre a level of flexibility to plan for clients returning for second doses of vaccine—including a viable option to dedicate some lanes to first and some to second doses while maintaining required levels of throughput (dependent of course on availability of vaccine supplies).
{kind=link}
{kind=link}
Process cycle times for baseline condition and post PDSA experimentation compared with required process completion rate/takt time (seconds). Security and administration, shown as the grey column, represents the sum of the separate security (dark blue) and administration (mid blue) columns for the baseline position and post PDSAs 1 to 4. In PDSA 5, security and administration were combined into a single process. Therefore, only the grey column is shown. PDSA, plan do study act.
Following the changes, a client feedback survey was introduced. Over a 4-week period, 15 343 clients were approached for feedback and 3227 responses received (giving a response rate of 21%). Only six respondents highlighted a longer than anticipated wait (less than 0.2%).
Lessons and limitations
Several key learnings emerged from the project.
First of all, the Lean principles provided a framework for improvement and were operationalised within the vaccination centre. Value was determined through client feedback and non-value through observation of bottlenecks and queues. The value-stream (or client journey) was mapped and process cycles timed and analysed in detail. Flow was improved by reorganising work processes and reducing (and rebalancing) cycle times. Pull was implemented via the FIFO queue servicing the clinical vaccination PODs—which enabled patients to be pulled forward to the next available POD. Perfection was pursued through securing staff input to potential changes and testing via a series of iterative PDSA cycles.
Second, multidisciplinary team working was key to improving flow. Balancing process cycle times was achieved by clinicians, administrators, vaccinators and volunteer marshals working together, flexibly, to reallocate tasks to the most appropriate member of the team. Diversity in multidisciplinary teams has been observed as an enabler of successful improvement.16 In this case, the multidisciplinary teams comprised a range of clinical and non-clinical staff from a variety of backgrounds, disciplines and levels of seniority. They could, therefore, draw on a broader range of skills and experiences to solve problems—including, in the case of vaccinators and volunteer marshals, professional knowledge and experience from outside the NHS.
Third, small changes can make a big difference. Changes were made daily via rapid experimentation to meet the needs of the process. The changes were relatively simple and, individually, quite small. However, guided by the Lean principles, the cumulative impact of the changes was considerable. Not only was flow across processes improved but capacity increased (by 50%) and client experience improved.
Finally, the temporary nature of the mass vaccination centres made them more readily reconfigurable. The opportunity to redesign clinical space is infrequent and typically involves costly capital developments.31 Previous studies have observed that poorly designed layouts can ‘lock-in’ inefficiency and waste to healthcare facilities —particularly if all relevant flows have not been considered.27–30 As the mass vaccination centres repurposed a large venue in the community, the space provided was rapidly setup using portable equipment. Therefore, this could be moved readily and rapidly to create and test new layouts when seeking to improve flow—or, indeed, to respond to the changing requirements of client cohorts.
Several limitations have been identified.
First, one of the authors, IMS, worked on the design and delivery of the Lean Fundamentals online programme and one, DS, worked on the case project. Therefore, there is the potential for positivity bias. To mitigate this, authors have practiced reflexivity and sought the opinions of colleagues on earlier drafts.
Second, the client satisfaction survey was introduced after changes were made. Therefore, no baseline position is available against which to measure improvement. However, problems with long queues and wait times initiated the project and anecdotal data from social media and local press reports suggest dissatisfaction was widespread prior to the changes.
Finally, the study reports on one case example. Therefore, results are less likely to be generalisable. Nevertheless, the experiences of the project are grounded in the daily reality of operating a mass vaccination centre and may be of value to others working in similar centres. With the ongoing threat of new COVID-19 variants and the expectation of additional booster vaccinations,5 the need for efficient vaccination deployment is likely an ongoing requirement. Therefore, further reports from other vaccination centres, including hospital and primary care sites, may be of benefit to form more widely generalisable lessons.
Conclusion
The design and operational management of vaccination centre processes contribute to client experience, efficiency and throughput. Lean provides a systematic approach that can improve operational processes and facilitate client flow through mass vaccination centres.
The rapid, PDSA experiments that took place were predominantly low-tech interventions involving changes to layout and the distribution of work tasks between staff working as a multidisciplinary team. The Lean concepts and techniques used were learnt and rapidly applied through participation in NHSE&I’s Lean Fundamentals online programme. Therefore, both the changes made and the practices used may be readily transferable to other vaccination centres—both in the UK NHS and, potentially, other healthcare systems.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge Elaine Bayliss for providing feedback on earlier drafts of the paper.
Footnotes
Contributors DTLS was responsible for the planning and conducting of the work described. IMS was responsible for reporting on the work and writing the article. DTLS contributed to the writing and revision of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests We have read and understood BMJ policy on declaration of interests and declare the following interests: IMS works as an improvement and transformation professional in the NHS and led the design and delivery of the Lean Fundamentals MOOC. DTLS works as an improvement and operations manager in the NHS and worked on the case project.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.