Article Text

Abstract
Obstetric triage has become one of the most crucial innovations in the field of perinatal care in the past 15 years. In lower- middle- income countries (LMICs), the pregnant patients are seen in a conventional way based on the time of their arrival; this divergent, unbalanced and inequitable approach results in delayed initial evaluation, prolonged length of stay (LOS) and affected clinical outcomes.
This project aimed at implementing an effective and efficient obstetric triage system with improved throughput and care processes within six months to facilitate timely decision making according to the individualized needs of pregnant patients.
A pre-implementation audit was completed for the core evaluation of existing obstetric triage services, followed by a fishbone analysis. Following the Donabedian model for quality care, a quality improvement project was initiated to redesign the obstetric triage system. The project strategy was implemented as part of six PDSA (Plan- Do -Study- Act) cycles to optimize the structure, processes, and obstetric triage outcomes. The triage paradigm moved from time-based care delivery to priority care, and processes were improved based on Angelini’s recommendations of best practices in obstetric triage. During the initial phase of improvement, the identified outcome measures were waiting time of 5 minutes from arrival to initial assessment, LOS of 120 minutes, and acuity-based care for at least 50% of patients. A post-implementation audit was conducted to assess improvements. The results showed that the LOS at triage reduced from 240 min (4 hours) to 60 min (1 hour) within 6 months. Furthermore, wait times for triage decreased significantly to 5 min in 65% of patients, compared with 6% in traditional triage practice.
The results indicate that the traditional triage model of the ‘order of arrival’ process is inefficient in providing adequate obstetric care. This quality initiative facilitated the successful incorporation of the Donabedian model and best practice triage practices and helped achieve desired outcomes of improved LOS and reduced waiting time with acuity-based care. Therefore, the design of an efficient,and the appropriate obstetric triage system can be adopted by other healthcare institutions in a local setting that can facilitate patient centric care.
- The Donabedian model
- Length of stay
- Angelini obstetric triage best practices
- Triage Acuity Tool: Fishbone Analysis: PDSA cycles
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- The Donabedian model
- Length of stay
- Angelini obstetric triage best practices
- Triage Acuity Tool: Fishbone Analysis: PDSA cycles
Introduction
Problem
This quality initiative is conducted in the labour and delivery (L&D) triage area of a tertiary care hospital that accounts to more than 6000 deliveries per annum. With a monthly turnover of 400–500 pregnant women, triage area is staffed round the clock to meet the needs of patients visiting L&D with complaints related to pregnancy concerns, labour and birth, medical problems and maternal-fetal surveillance. Booked patients with 24 completed weeks gestation and above are assessed in L&D triage whereas unbooked pregnant women and booked patients with less than 24 weeks gestation are assessed by the emergency department.
In our healthcare setup, obstetric triage was implemented in a traditional pattern whereby the pregnant patients were seen and evaluated on the basis of their reporting time at the reception instead of the urgency of their clinical presentation. In 2018, a sentinel event happened to a pregnant woman waiting in L&D triage. The patient presented with labour pains and per vaginal leaking, her assessment was delayed due to other patients waiting before her, triage turnover was slow due to non-availability of bed and busy staffing. When finally assessed, she was in active labour with grade 2 meconium-stained liquor, and cardiotocography was pathological. Her emergency caesarean was performed, however, due to delayed intervention, there was a serious jeopardy with adverse neonatal outcome results.
This sentinel occurrence triggered an urgent need to examine existing obstetric triage practices and develop a more efficient and safe triage process. In addition, there has been an increase in reported cases and patient complaints with respect to timeliness of care and wait times. In order to mitigate the risk and further incidents, quality initiative team consisted of obstetric experts and lead nurses decided to conduct a quality project to bring improvement by revamping of the obstetric triage system. The primary objective was to enhance triage performance by reducing wait time and length of stay (LOS) and providing priority care. As there were no prior data available for triage system evaluation, an audit was planned to provide a baseline assessment of the triage flow process including LOS and wait time for initial assessment. The goal was to compare data prior to and after the intervention.
Available knowledge
Obstetric triage has emerged as one of the most significant perinatal service innovations in the last 15 years.1 Due to physiological, social, and emotional changes, pregnant patients are considered as one of the most vulnerable populations in the healthcare spectrum. Assessment in triage not only affects the initial evaluation of labouring or non-labouring patient, but also determines the direction and timing of further obstetric care. The Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) describes obstetric triage as ‘the brief, thorough and systematic, maternal and fetal assessment performed when a pregnant woman presents for care, to determine priority for full evaluation’.2
It is vital for hospitals and healthcare facilities to provide the best individual care for this population and to prevent adverse events and complications. Obstetric triage, as observed in high resource countries, enabled better triage utilisation with improved maternal and fetal assessment.3 However, in a systematic review addressing critical care in lower- middle- income countries (LMICs), Baker4 highlighted emergency care provision and triage as the weakest components of the health system and emphasised that improvement in these areas can be lifesaving and costeffective. In commonly practised obstetric triaging in LMICs, patients are seen on the first come first serve basis.5 This may result in leaving patients without initial evaluation and delayed delivery of necessary care to the one who need it on priority.6 The most significant problems associated with traditional triage are patient dissatisfaction, extended wait times, and increased morbidity and mortality.7
For efficient triage, wait times for initial assessment, LOS and priority care are identified as performance measures.8 Unfortunately, there are currently no defined benchmarks available for these obstetric triage times. According to the obstetric triage system implemented in the United Kingdom(UK), assessment by a midwife should occur within 15 min of patient arrival followed by the assignment of acuity level9 whereas AWHONN recommends that initial assessment should be done in 10 min.2 Some studies reported a time interval of 5 to 6 min between arrival and initial assessment.10 11 Similarly, for LOS variable times have been reported.9
For priority care, acuity determination is essential to facilitate standardised care, increase patient satisfaction, and improve system efficiency. American College of Obstetricians & Gynecologists (ACOG) and American Academy of Pediatrics (AAP)guidelines for perinatal care also endorse timely assessment of women who present in the labour and delivery area.12 Currently, four and five tiered obstetric triage acuity tools are available in different countries like obstetrical triage acuity scale (OTAS) in Canada, Maternal Fetal Triage Index (MFTI) and Florida Hospital Obstetric Triage Acuity Tools in United States (USA), Birmingham Symptom Specific Obstetric Triage System (BSOTS) inUK and Swiss Emergency Triage Scale (SETS) in Europe.13–15 Some of these acuity tools are validated and allows standardised assessment based on the presenting complaints, key clinical indicators (vital signs and fetal heart rate) and the parameters based on initial evaluation are used to define levels of urgency and subsequent assessment and care plan.9 15 Forshaw et al16 highlighted the lack of specific and validated obstetric triage acuity tools for low-resource areas despite the need to improve quality of care. Only a few studies have reported the use of acuity tools in healthcare facilities of LMICs.17 18
There is still a lack of consensus on how to devise a single standardised tool or a defined system for effective obstetric triaging.15 19 Angelini and Howard in a systematic review of the past fifteen years for obstetric triage shared seven key categories and the concept of ‘best practice triage model’.3 Angelini emphasised that specific obstetric risk stratification tool was just one component and other components required were the standardisation of assessment, adequate staffing, development of clinical protocols, professional provider mix model, identification of pitfalls including hands-off, ongoing team training and quality improvement. This reflects the fact that the paradigm of obstetric triage is a complex process and is influenced by factors such as the environment, workforce, care pathways and communication.
To ensure best practice triage model, there is need to have a standardised, quality based obstetric triage system where the performance outcomes could be monitored. The well-established Donabedian model of quality care, first described in 1966, is unique as this can be used to conceptualise quality improvement and to evaluate quality assurance.20 This framework of structure, process, and outcome essentially has a linear relationship, where structure affects process, and process affects outcomes. A structure in the model refers to the way care is delivered, including facilities, equipment, and human resources. The process involves the care provided and includes the care processes, guidelines, treatments, interactions between patients and providers, and education. Whereas the outcome implies the impact of the healthcare structure and process, including service quality, performance, satisfaction, security and awareness. Within this quality framework, the Plan-Do-Study-Act (PDSA) cycle can be used to implement changes in specific areas and help to assess improvements at each step.21 Therefore, this widely used Donabedian model is highly necessary in obstetric triage, from which obstetric care begins. This was also emphasised by Rashidi Fakari et al,22 from Iran who elaborated that the index of obstetric triage quality is affected by quality of process, structure, and outcomes for obstetric triage. Furthermore, Rashidi-Fakari et al 23 reported that the similar framework can be used for standardisation and quality assurance of the obstetric triage process.
Based on these observations, in a health organisation a quality based triage system can be devised by integration of Angelini’s key strategies within Donabedian framework using PDSA cycles to achieve ‘Best Triage Model’. Ultimate improvement in triage system can lead to efficient and safe patient care with a reduction in LOS, improved patient satisfaction and reduced morbidity. A standardised triage system is not used in healthcare facilities in Pakistan. This project will also provide a pathway for other care providers in LMICs to consider adapting these strategies in their institutions.
Rationale
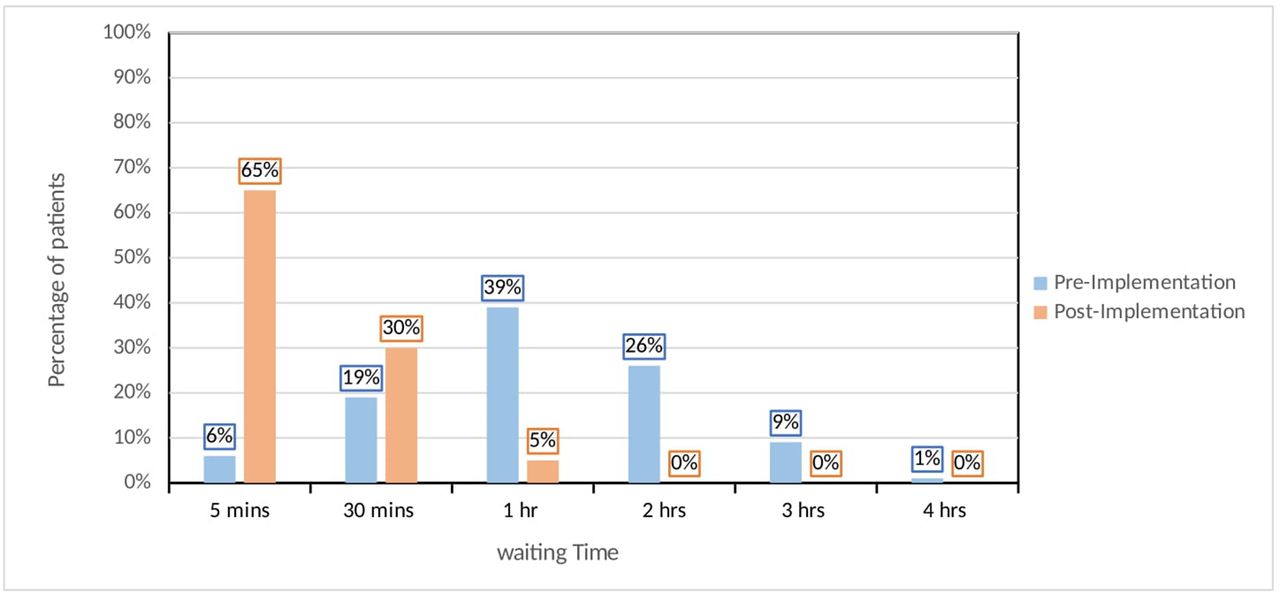
After recognising a substantial problem with obstetric triage, a project team was established to assess the issues, identify causes, and focus on the problem as a priority. A baseline audit of L&D triage was conducted to evaluate triage throughput, including waiting time (arrival to initial assessment) and LOS during the first quarter of the year in 2018. The data were collected over a month, using a structured survey to get an ‘idea’ of the problem. The audit results showed triage waiting time ranged widely between five to 240 min and a 5 min target wait time was achieved in only 6% patients (figure 1). Whereas LOS in L&D triage extended up to 3 to 4 hours, irrespective of the patient’s clinical presentations and in 16% of cases LOS was not documented (figure 2).

Triage waiting time from arrival to initial assessment.
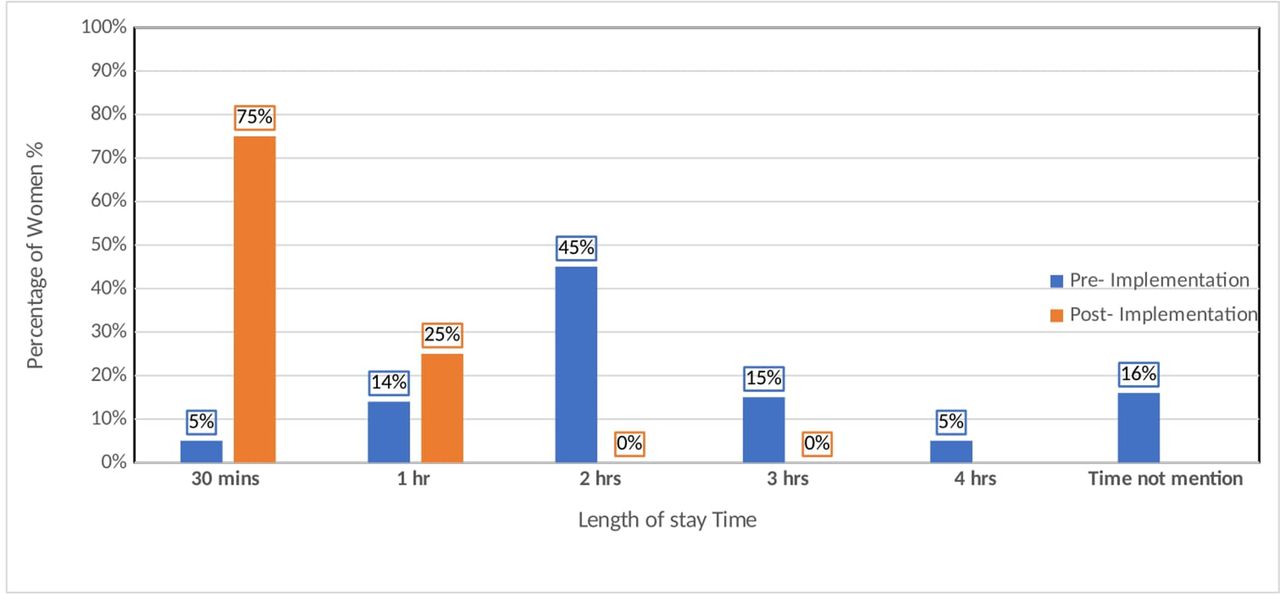
Length of stay.
Based on the results of the audit, the team determined that delays in the initial assessment and further assessment resulted in an increase in LOS and wait times. The project team decided on cause-and-effect analysis using fishbone diagram24 (online supplemental file 1 Fishbone Diagram). The in-depth analysis of the problem identified issues in different steps of the routine triage flow process. Patients presenting at triage initially reporting to the unit receptionist, had to complete the check-in process before a registered nurse was notified of the patient’s arrival. The assigned nurse, engaged in other patients’ assessments in the triage room, was sometimes unaware of patient’s arrival for a significant period. Similarly, issues were identified for timely involvement of the physicians. Initial nursing evaluation and obstetric assessment by physicians were performed in a single, three bedded triage room. Factors like occupancy of triage beds for unpredictable times, delay in patient assessment irrespective of clinical presentation and compromised communication among healthcare providers were contributing to prolonged waiting times and delay in the initial assessment.
Supplemental material
The existing triage policy focused mainly on priority 1 category for acute emergency cases. Triage Severity Index (prioritisation criteria) was not in use to determine appropriate treatment needs. In the absence of a clearly defined system, patients with less severe symptoms received care earlier than those with emergency and semi-emergency needs. The time frame between the report and the decision was 120 min, but it was not achievable most of the time. Similarly, there was no defined process for the disposition of patients from triage to other clinical areas. The report findings revealed that issues in a flow process with increasing patient volumes, physical space inhibition and staffing limitations were impeding smooth care delivery in triage.
The team concluded that there was a lack of standardised approach without a clear definition of process-time targets, priority-based acuity tool, defined roles, and responsibilities. Additionally, there was compromised communication, knowledge deficit and lack of information retrieval due to improper documentation. In addition, space and personnel constraints also make things difficult.
Based on these observations, the team hypothesised that triage throughput will improve by revamping of structure,change in triage flow process and shifting of care paradigm from the order in which patient arrive ‘to’ the provision of priority based care according to pregnant patient’s needs.
Specific aims
The team aimed to achieve the desired results of efficient, and effective triage with improved throughput and care processes within 6 months by using the Donabedian framework. In the initial phase of improvement, three baseline performance metrics were decided to include: wait time from arrival to initial assessment, LOS, and acuity-based care. To evaluate the effectiveness of the quality initiative processes, improvement was desirable for at least 50% of patients.
Methods
Context
The quality improvement team, comprised of key stakeholders including physicians, nurses, quality and patient safety unit representatives and other staff, initiated the improvement project. An in-depth literature search was conducted to review existing triage systems, and expert feedback was gathered at the departmental and institutional levels. The intention was to look for evidence-based improvement plan for highlighted issues in the existing triage system. As improvement was needed at all levels in the obstetric triage, the project team contemplated concepts of the Donabedian framework to establish an efficient and effective system.
The quality team pondered that within this quality framework, improvements in structure, manpower and equipment facilities were likely to upgrade triage inputs, and modification of processes by integrating Angelini’s best triage practices in local perspective will help to improve the outcome measures (figure 3). With the evolution of processes and practices, it was expected that efficiency, satisfaction, and performance measures would improve. The team expected that a regular assessment of the structure, processes and outcomes of continuous quality improvement would also be possible under this quality model.
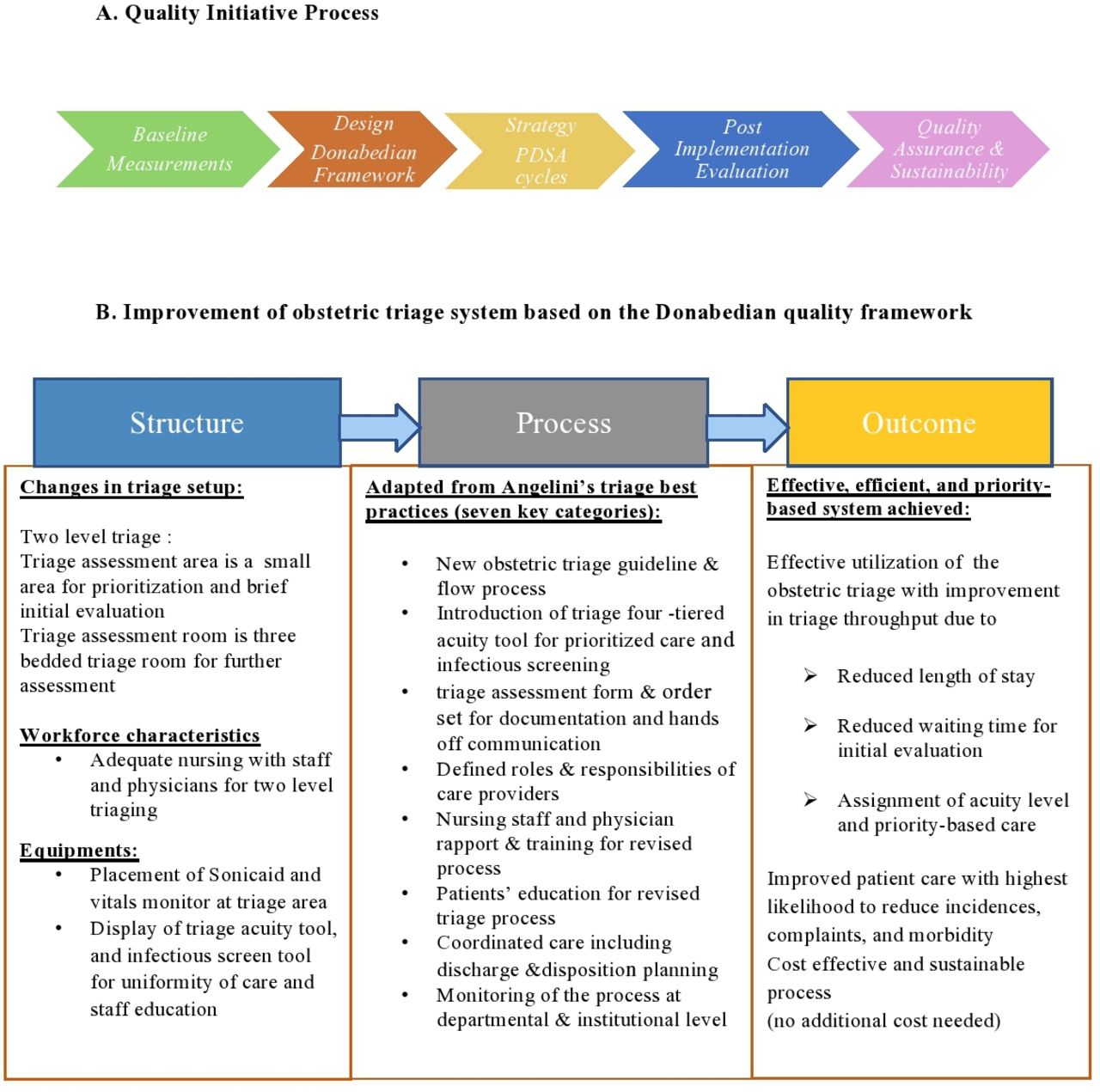
A-Quality Initiative Process & B-Improvement of obstetric triage system based on the Donabedian quality framework.
To attain more efficient system, team decided for 5 min target for initial wait time based on the available evidence, and 120 min were considered as benchmark for LOS (the defined hospital indicator for triage) with acuity-based care for at least 50% of patients.
The frequency of meetings of the project team was about once every month during the cycles to monitor the implementation and to assess improvement with performance outcome measures.
Intervention
To implement the quality plan, six PDSA cycles were completed to achieve the desired results. These PDSA cycles focused on change in structure, risk stratification with obstetric triage acuity tool and infectious screening, implementation of triage guidelines and flow process, hands-off communication with triage initial assessment form and order set, adequate staffing, process awareness and training sessions for physicians and nursing staff. Each cycle was comprised of four phases of planning, implementation, analysis, and evaluation.
PDSA cycle 1
Our initial intervention was to create a designated area for rapid assessment and prioritisation of pregnant patients presenting in L&D triage. Despite a space constraint, the team decided to make more efficient use of the available area. This was achieved by introducing relevant changes in the existing structure of L&D, a smaller area was created next to the unit receptionist counter called labour triage area for the initial brief assessment and priority evaluation. For a more detailed assessment of pregnant women, three beds were used in the existing labour triage room. These areas were equipped accordingly. Subsequently, pamphlets for the triage prioritisation tool were also posted in the triage area. This structural change allowed patients to be evaluated in two stages and improved triage fluidity. Due to high patients’ census, a work plan was also proposed for expansion of the L&D area for further improvement.
PDSA cycle 2
To develop and enhance our reminder model, an evidence-based obstetric triage acuity tool was indispensable for prioritised patient care. Based on the literature review a paper-based four-tiered acuity tool validated in similar context was adapted.25 This adapted tool was synchronous to our clinical services and obstetric patients’ needs. We preferred four-tiered tool due to simplicity of use, relevance, and practicality. Four levels of acuity were defined based on the urgency of the assessment, the level of the caregiver, the area of assessment, the reassessment and the disposition process (online supplemental file 2 Obstetric Acuity Tool). The acuity assessment was based on the presenting complaint and key clinical indicators including vital signs and fetal heart rate. The tool included obstetrical and non-obstetrical complaints comprising contractions, rupture of membranes, vaginal bleeding, reduced fetal movements, hypertensive disorder, neurological symptoms, abdominal pain, infection, chest pain and/or breathing problems, urinary and gastrointestinal symptoms during pregnancy. For vital signs cut-off levels adapted to the physiological changes of pregnancy. If two different acuity levels emerged after chief complaint and vital signs, the patient was allocated to the higher level. This initial evaluation was to be completed within 5 min prior to further assessment.
Supplemental material
The four tiers were highlighted with colours as red level 1: immediate assessment within 15 min, amber level 2: emergent assessment within 30 min, green level 3: urgent assessment within 60 min and white level 4: non-urgent assessment to be done within 120 min. In available literature review, the timelines for non-urgent cases ranged from 120 min to 240 min for different available acuity tools. We opted for 120 min for acuity level 4 to improve processing time and triage use. This was also in accordance with the hospital recommended benchmark for triage LOS.
The acuity tool was reviewed by senior obstetricians and nurse instructor. Since there was no such model or tool that formally existed in Pakistan, this method proved to be most appropriate in the setting. We decided with implementation of this, we will also establish whether this tool may be applicable in our context. Furthermore, these four acuity levels were supported by a standardised algorithm. Early feedback from nurses indicated that it was frustrating to recall each level of acuity and caused difficulties in the workforce process. This concern was addressed with further PDSA cycles.
PDSA cycle 3
The previous triage guideline was mainly focusing on category 1 and there were no defined timelines and responsibilities. For uniform and appropriate care, the team decided to revise triage guideline to make it a more comprehensive document incorporating modifications. Input from the relevant expertise and available evidence reviewed. In the new guideline, the revised flow process and acuity tool were incorporated along with defining roles, responsibilities, and care processes for all the acuity levels (online supplemental file 3 Triage Flow Process). Assessment and disposition processes were also described. Approval for the new document obtained from the department and hospital leadership. The sessions were organised to raise awareness among physicians and staff who responded positively to the revised guidance and found the document to be fairly explainable and practical. This guideline facilitated smooth running of triage and sustainability of improvement changes. We also incorporated a triage order set for standardised care, so it was easier to follow and not miss any important care aspect in a single view (online supplemental file 4 Triage Order Set).
Supplemental material
Supplemental material
PDSA cycle 4
For our fourth cycle, we deeply explored how to improve communication process at triage. We decided to integrate the acuity tool and hands-off process. We realised that the only way was to create a tool for initial assessment and acuity assessment in one document. Therefore, we developed a triage assessment form, including non-intervention elements based on the SBAR (Situation, Background, Assessment and Recommendations),infectious disease screening and the obstetric triage acuity tool (online supplemental file 5 Triage Assessment Form). This form was displayed at triage area for quick reference. It worked as an intelligent and better way of sorting patients and documenting patient results appropriately.
Supplemental material
PDSA cycle 5
The acquisition of acuity tools, guideline and structural changes is essential but inefficient without the presence of dedicated staff to ensure smooth workflow and continuous monitoring of the process. Similarly, care providers understanding and knowledge of implemented process is essential and if not trained properly, they can be the cause for delay in service provision. To ensure effective transformation, for our fifth cycle, changes were made in the existing staffing model. Dedicated nursing staff (one staff for triage area and one for triage room) and physicians were appointed in shifts for smooth running of the triage process. With additional staff arrangements, the area was staffed 24 hours a day to meet the needs of our pregnant patients.
We trained our triage care providers for improved high-quality care. On-the-job training sessions were held for nurses and obstetricians to assist with the evolution of the process. A dedicated, 8-hour workshop was conducted for obstetric triage module covering essential concepts of triage definitions, and triage system including re-triage, urgency, and triage scale, this also encompassed possible outcomes: under and over triage, correct triage decision, communication issues, and pain assessment at triage. New triage guidelines, acuity tool, flow process, documentation requirements, infectious disease screening and isolation type, were introduced and practised. For evaluation component, case-based assessments and skill sign off was done. The workshops took place once every 3 months.
To maintain quality assurance, reinforcement of the process was ensured to the nursing staff as part of daily huddles. This was further reinforced by the time-to-time assessments of nursing performance on actual patients. For its quality assurance, routine monitoring by clinical quality lead was ensured.
PDSA cycle 6
After five PDSA cycles, a new triage flow process was developed with defined timelines. The process steps were planned in the following sequence. On arrival, the patient reporting at triage, will be greeted by the nurse. The assessment of patients in the triage will take place in two stages. Within 5 min of arrival, assigned nurse will approach the patient in the L&D triage area for initial brief assessment. The area nurse will inquire for a brief history, infectious screening, fetal movements, and uterine contractions. The initial evaluation will include vital signs and fetal heart sounds assessment. The case will be prioritised in accordance with the acuity tool. These findings will be documented on the triage assessment form. This form shall be a comprehensive document consisting of obstetric acuity and infectious screening tool and hands off component. Triage area assigned nurse will hand over the patient to the assigned nurse of triage assessment room and the patient will be shifted there for further nursing and obstetric assessment by physicians. Triage room nurse will check the order set for completion of care process.
For unwell women fulfilling level 1 criteria of the obstetric acuity tool, labour room consultant will be immediately involved. After quick assessment in the triage area, patient will be directly transferred to labour room or operation theatre for further management including delivery. Pregnant patients presenting with other acuity categories will be managed according to the defined care process. To improve turnover, reassessment and disposition process will be performed according to the defined flow process in the new triage guideline.
L&D team leader will be contacted for help in case of unavailability of bed and for the women waiting longer than 15 min in triage. It will be the responsibility of the unit receptionist to keep a record of arrival and triage times for each woman, and in case of target time breach, he/she will activate the escalation by paging team leader. Nursing lead will also have the responsibility to investigate and respond to any patient feedback regarding triage flow and care process. They will be supported by the on-floor labour room consultant and physicians in the smooth triage process.
Study of intervention
The comparative review of quality assurance record forms of pre and postintervention audit was conducted to assess the impact and efficacy of application of the Donabedian model in our setting. All data recorded in the first quarter of 2018 and second quarter of 2019 as a preintervention and postimplementation audit were used to review the impact of quality improvement measures. These data were based on a convenience sample of women (n=200) attending obstetric triage as a pilot for preaudit (n=100) and postaudit phase (n=100).
All pregnant patients presented to obstetric triage with complaints related to pregnancy or non-obstetric issues and for maternal-fetal surveillance were included. Patients who were directly admitted to the L&D area were excluded.
Outcome measures
Waiting time: wait time from arrival (after registration) to initial nursing assessment, measured in minutes. Target was 5 minutes.
Acuity-based care: percentage of patients receiving acuity based care.Target was 50%.
Length of Stay: time from triage to final decision: either discharged, admitted in L& D, or shifted to the ward. Target was 120 minutes.
The data was input, coded, modified and analysed using MS Excel windows 10. The simple descriptive analysis was carried out for three categorical variables including LOS,waiting time and acuity based care using percentages differences to explore the trends and occurrences in pre and postintervention phases.
Patient involvement
Patients were not involved in the design, or conduct, or reporting, or dissemination plans of our quality improvement project.
Results
The pre and postintervention demographic data shows that labour pains were the main presenting complaint in patients visiting L& D triage. The breakdown of gestational age of women visiting the triage area indicated that 50% of women were between 37 and 41 weeks of gestational age, while 50% were between 24 and 36 weeks of age. Data of preaudit and postaudit results were compared for outcome measures of waiting time and LOS. In postimplementation audit, assessment for utilisation of acuity tool was also performed.
Figure 1 illustrates the measurement of triage wait time outcomes. We collected the data on wait time during preintervention phase and then in the postintervention phase, there is a significant difference in the pre and postintervention waiting time. In the preintervention, the wait time was up to 4 hours irrespective of the triage and urgency of the delivery. A five- minutes waiting time was met in only 6% patients whereas in postintervention phase, triage waiting time reduce significantly as 65% of the patients waited 5 min and the remaining 30% patients were assessed within half an hour.
As shown in figure 2, preimplementation (LOS) ranged from 30 min to 240 min. Only 64% met the recommended turnaround time of 120 min and for the remaining 36% patients, LOS in triage extended up to 3 to 4 hours, irrespective of their clinical presentations. Postimplementation results showed marked improvement with 75% patients having LOS of 30 min and for the remaining 25% this was 60 min.
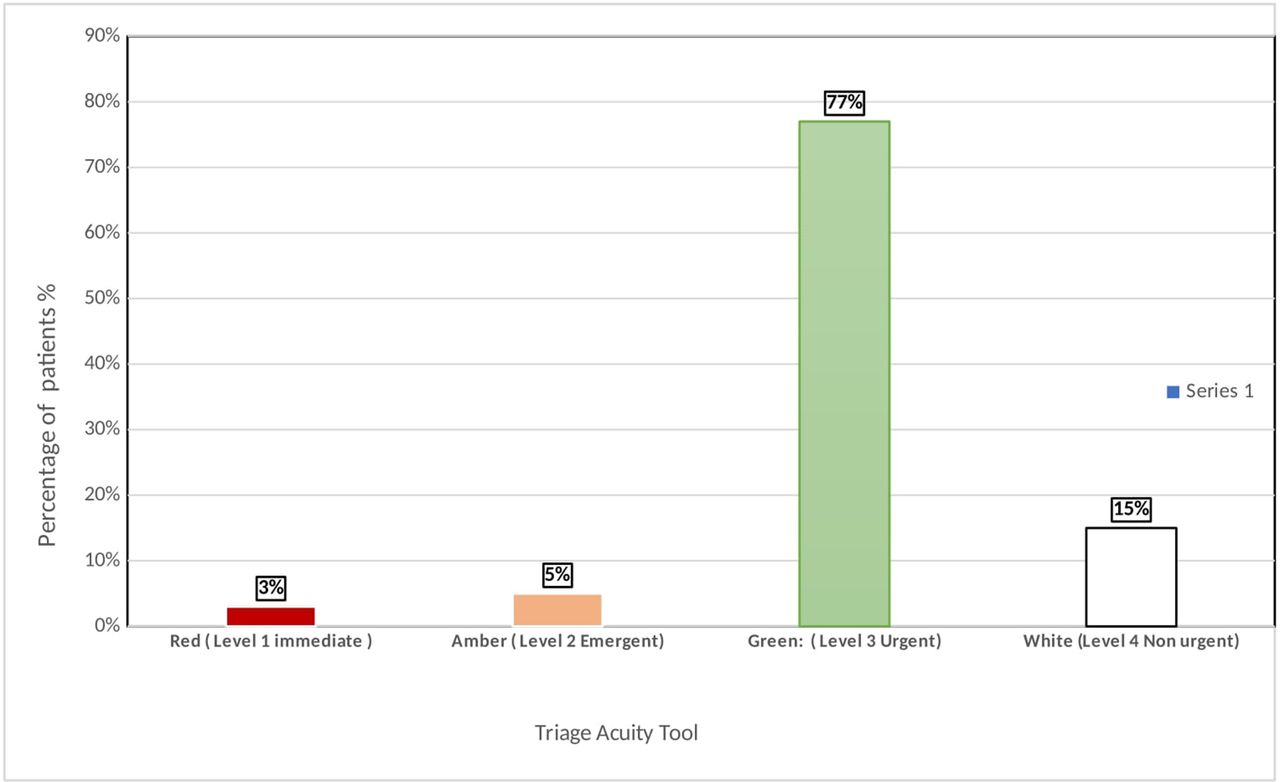
Figure 4 presents implementation of obstetric acuity tool that categorised patients in the postimplementation in four levels of urgencies which did not use to happen before. The data shows that 3% of patients were in the red category, 5% with amber category, 77% with green category and 15% were -non-urgent (white category) cases. Acuity tool implementation helped the staff to do triaging based on urgency level and accordingly accommodate the patients based on their clinical presentations and complexities. As no such assessment had been conducted previously, no data were available to compare the triage urgency.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Utilisation of acuity tool.
Discussion
Summary
As elaborated in figure 3, the Donabedian model enabled improvement at all levels of obstetric triage, and changes implemented with PDSA cycles helped to achieve performance above desired targets. The improvement in LOS and 5 min wait times is indicative of an effective and efficient system with greater ability to triage and prioritise acuity-based care.
Interpretation
Wait times are considered as one of the main indicators of patient satisfaction. Though, there is no consensus on what is the right and appropriate waiting time for a pregnant patient who presents at obstetric triage, initial assessment for prioritisation should be done in the shortest possible time. During the initial project phase, we decided to achieve 5 min waiting time for at least 50% of patients for initial assessment. Improvement in waiting time was above the planned targets and achieved in 6-months period. There are limited studies from LMICs showing improvement in waiting times in high volume obstetric. A study reported from Ghana addressed the third delay in understanding wait times at a high-volume hospital. An improvement programme for obstetric triage reduced the median patient waiting time from facility arrival to first assessment by a midwife from 40 min to 5 min (p<0.001) over the 5-year intervention.10 Murray A implemented MFTI tool in a rural community hospital and reported improvement in patient arrival to priority index assignment from 21.6 min in first month to 6.3 min in third month. This improvement was 50%to 100% over the period of first to third month.11
At our facility, the acuity tool was introduced for the first time for obstetric triage. The tool, we adapted was based on four-tiered validated Birmingham Symptom Specific Obstetric Triage System.9 25 This was decided to first assess its uptake, understanding and application for the revised system. In the postimplementation audit, the use of the acuity assessment tool was evaluated, and the percentage of women at each level of emergency was assessed. Our results were comparable to those of a locally conducted study. This comparative study used five-tiered Maternal Fetal Traige Index for obstetric triage improvement and results showed 2% of patients were in category 1, 5.6% were in category 2, and majority were in remaining categories.26
There has been a clear improvement in LOS from 240 min (4 hours) to 60 min. These findings were congruent with other studies addressing quality improvement strategies for obstetric triage. DePaoli W., used lean transformation methodology in a university hospital of an urban city and results showed LOS reduction from 152 minto 120.58 min.27 Rovai and Champagne also mentioned that with standardised workflows, reduction in LOS was achievable and reported improvement from 97 min to 82 min based on 10 months data.28 Our target for LOS was 120 min and reducing timeline for non-urgent (low acuity) cases helped to achieve marked improvement in LOS. Similar observations were shared by Smithson et al,14 who in a prospective study evaluated impact of OTAS tool. He used simulation modelling and emphasised that fast track for low acuity patients (levels 4 and 5) helped to reduce overall LOS from 101 min to 73 min.
Sustainability is considered an essential aspect of the quality improvement process. The Donabedian framework facilitated quality assurance with regular evaluation of structure, process, and outcomes for ongoing quality improvement. The triage process was monitored continuously with unit-based compliance surveys and hospital quality and patient safety department overseeing the compliance by carrying out close and open medical record audit.
Lessons and limitations
This quality initiative was a multidisciplinary teamwork, we ensured that all members were involved throughout the process by attending team meetings, collecting written feedbacks, and by individual discussions. Their input during the planning process contributed to the achievement of a new sustainable system. A key lesson learnt throughout the process was the importance of the PDSA cycles, which helped to optimise each step prior to full implementation in L&D.
There is a lack of literature in the Pakistan’s context that focuses specifically on managing labour triage in tertiary care settings. Even though the new obstetric triage implementation system has significantly improved the care process, it is necessary to develop a validated acuity tool from a local perspective.
The acuity tool, we used for our quality initiative was based on the available evidence and adapted for local use. The tool validity and reliability in local setting was out of scope for our project as this quality improvement initiative was conducted for triage system improvement within defined timelines.
As our quality initiative mainly focused on efficient and effective system change, another hindrance was limited outcome measures. The outcome measures of patient satisfaction were not evaluated in this study. However, this outcome measure can explicitly be assessed by qualitative research in the future. Similarly, for generalizability of information, there is a need to plan a robust randomised controlled trial. However, these results were achieved cost-effectively with existing resources, and no additional budgetary or financial assistance was obtained.
Conclusion
The project aimed to improve the quality of care for obstetric patients by focusing on the implementation of a sustainable alternative instead of a short-term intervention. The project team was able to identify the gaps in the triage system using the systematic approach, making interventions that focused on these gaps to minimise the risk of unsafe care. To maintain the continuous improvement, the project team has selected unit leads to secure the project aims. This is also reinforced by quarterly audits of quality and patient safety unit to ensure compliance with the revised process. Considering the significant results achieved by this project, it is essential to ensure that these improvement interventions circulate in our obstetric units in secondary hospitals. In addition, evidence is urgently needed in lower-middle-income countries, particularly those in the South Asia where maternal mortality and morbidity are prevalent. Triage systems such as these have great potential to strengthen the system of patient-centred and safe care.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Exemption from the hospital ethical review board was obtained. Already collected, and entered data were extracted from the department’s data repository based on medical records to explore the impact of changes with the obstetrics triage improvement process.
Acknowledgments
The authors would like to acknowledge Dr. Maleeha Naseem and Dr Azra Amerjee for their input for the manuscript and the support of the nursing staff for management of triage process.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SN and LS conceptualised the idea of the triage improvement. SN, SS, and ZI worked closely under supervision of LS in the development of the system and implementation of triage management on floor. SB supported in writing of the research paper and ethical review approval process. All authors have made equal contribution in writing and reviewing of the manuscript.
SN is responsible for the overall content as the guarantor and accepts full responsibility for the work and/or the conductof the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.