Article Text

Abstract
Patients who do not have enough information about their discharge plans have decreased treatment compliance, decreased patient safety, increased emergency department (ED) recidivism, and poor satisfaction. This project aimed to develop and implement a method to assess and improve patient understanding of treatment and discharge plan in the ED. The authors developed a questionnaire to assess patient knowledge using Centers for Medicare and Medicaid Services and Joint Commission recommendations, areas of communication deficits reported in other manuscripts, and ED staff and provider input. Responses from patient interviews were then scored against the medical record. Three trained scorers graded all responses, and inter-rater reliability was calculated using the kappa statistic.
Baseline observations found that written discharge instructions were long and tedious, and important information was difficult to find. Based on initial patient scores, stakeholder interviews, and fishbone diagrams, the team developed a one-page simplified information page (SIP) targeted to inform patients their most relevant discharge instructions. Next, the SIP was tested on 118 patients to measure its effect on patient understanding. At the baseline study, no patients had complete understanding of their discharge instructions. The areas of lowest scores were medication instructions and indications to return to the ED. Implementation of the SIP resulted in statistically significant changes in score distribution across all questions assessed with the Wilcoxon signed-rank test. Interrater reliability between scorers was high (kappa=0.84). We incorporated the concept of the SIP to the cover page of our standard discharge instructions.
Healthcare providers often spend valuable time educating their patients, and it is important to assess the effectiveness of this teaching to identify areas in which we may improve health literacy and patient understanding. This project has shown that a simple, easy-to-read, concise page developed with patient input significantly improved ED discharge instruction knowledge.
- patient education
- medical education
- emergency department
- electronic health records
- health literacy
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Patient noncompliance with medical discharge instructions can lead to unfavourable outcomes when, for instance, prescribed medications are not taken, concerning symptoms are ignored, and follow-up visits are missed. Healthcare staff should makes efforts ensure that discharge instructions are fully understood before releasing a patient from the ED.
The process analysed in this project occurs at the time of patient discharge from the ED at Clements University Hospital, an urban academic hospital in Dallas, Texas. In 2017, the Clements University Hospital ED saw approximately 43 500 patients per year.
The aim of this project is to improve patient knowledge and understanding of their emergency medicine visit, as measured by our composite score, by 20% from March 2017 to January 2019.
Background
Printed hospital discharge instructions provide a permanent reference for patients with details about their medical condition, ongoing management of their illness and recommended follow-up. Even though most institutions use templates for discharge, the content of these instructions varies between individual providers based on what they believe patients need to know. It is often assumed that patients understand the documents they are given, but at least 78% of patients discharged from the ED exhibited comprehension deficits for at least one area of their ED care and discharge instructions.1 2
Patients are often unaware of their difficulties with comprehension, which raises concern for their adherence to treatment plans and possible future adverse events. One that may play a part in patient understanding of and compliance with medical instructions is health literacy, a patient’s understanding of information related to their medical condition and their ability to use this knowledge to make decisions regarding their healthcare.3 4 Mean ED patient reading levels range from grades 3 to 10 depending on the hospital setting, but even highly educated people have been found to have poor medical comprehension.5 Studies have shown that approximately one-third of Americans have low health literacy.6
There is little research to identify strategies and interventions to improve communication and patient comprehension at discharge from the ED. However, in the few instances when comprehension is studied, poor results have not necessarily resulted in changes to the printed materials given at discharge from the ED.7 In the inpatient setting, evidence increasingly shows that efforts to enhance information delivery at discharge have a positive impact on morbidity and resource utilisation.2
With its fast-paced and chaotic environment, communication can be difficult in the ED. Studies of recorded ED discharge encounters found that verbal exchanges between patients and providers were very brief (76 s on average for providers and 14 s on average for patients) and often incomplete.6 The discharge process is recognised as a time with increased risk for communication failures.2 7 One investigation found that almost half (42%) of patients received incomplete discharge instructions.8 This is a suboptimal approach as many patients do not understand their discharge medications and are often unable to recall even their primary diagnoses.9
The most frequent areas of deficiency were found to be medication dosage and duration (80%) and return instructions (79%), important components of post-ED care.6 Communication failures at hospital discharge have been found to lead to poor adherence with follow-up visits, incomplete laboratory testing and adverse events, resulting in repeat visits and increased hospital utilisation.2 In fact, reported noncompliance with follow-up appointments ranges from 20% to 67%, and one in five hospitalisations is complicated by a postdischarge adverse event, some of which may lead to preventable ED visits or readmissions to the hospital.10 With approximately 136.9 million visits to the ED in the USA in 2015, this is an important issue to address.11
One last, but incredibly relevant, consideration is patient satisfaction. Patient satisfaction is important as a measure of quality of care, but also economically as it is a factor for hospitals in Medicare reimbursement. Studies have shown that overall patient satisfaction levels increase when patients feel that providers are invested in their care, are well informed about the cause of their symptoms, tests that were conducted and reason for admission.12
Measurement
This study employed the Plan, Do, Study, Act (PDSA) cycle as a framework. The ‘Plan’ phase occupied a large portion of the project as we sought to understand current discharge practices in the ED and input of stakeholders. The scope of the patient care steps studied in this project was limited to the immediate discharge process. The patient population interviewed and studied was limited to those who were discharged from the ED, received medical treatment in the ED, and had medication or treatment changes on discharge. Patients were excluded if they did not choose to participate, were unable to participate (whether due to decreased consciousness or pain), were being admitted to the inpatient floor, or did not have any treatments prescribed on discharge.
Using the CMS OP-19 Transfer Record, Joint Commission recommendations for elements of high-quality discharge instructions and medical information, and interviews with ED physicians, nurses and staff, we chose six elements that were most important.13 We organised these into a short questionnaire to assess patient understanding. The questions were ‘What was your diagnosis?’ ‘What treatments did you receive in the ED?’ ‘What treatment (medications, diet, therapy, wound care, etc) was recommended to you now that you have been discharged, and what is the frequency and duration of the treatment?’ ‘What doctors or clinics do you need to follow up with after your ED visit?’ ‘For what symptoms or changes should you return to the ED?’ and ‘Have you read your discharge instructions?’
All ED physicians and staff were informed about the ongoing project. Interviews were conducted in person by trained medical students at the time of discharge. We chose the time after patients received verbal instructions from nurses and were given their after-visit summary (AVS), a packet of discharge instructions including prescriptions and instructions. This was an optimal time for our assessment as all standard discharge information had been disseminated and patients had their discharge documents in hand to use for reference.
Baseline data were collected from 50 patients who met selection criteria. The questionnaire assessed knowledge of the diagnosis, ED tests and treatments, postdischarge treatments (including prescription names and other care instructions), medication frequency, follow-up clinics and reasons to return to the ED (figure 1). These results show that patients’ understanding is lacking in the domain of post-ED care. The two lowest areas of comprehension are ‘reasons to return to the ED’ and ‘medication frequency and duration.’ There was a high variance in total scores, and none of the 50 patients analysed initially had complete comprehension of their ED visit and discharge instructions.
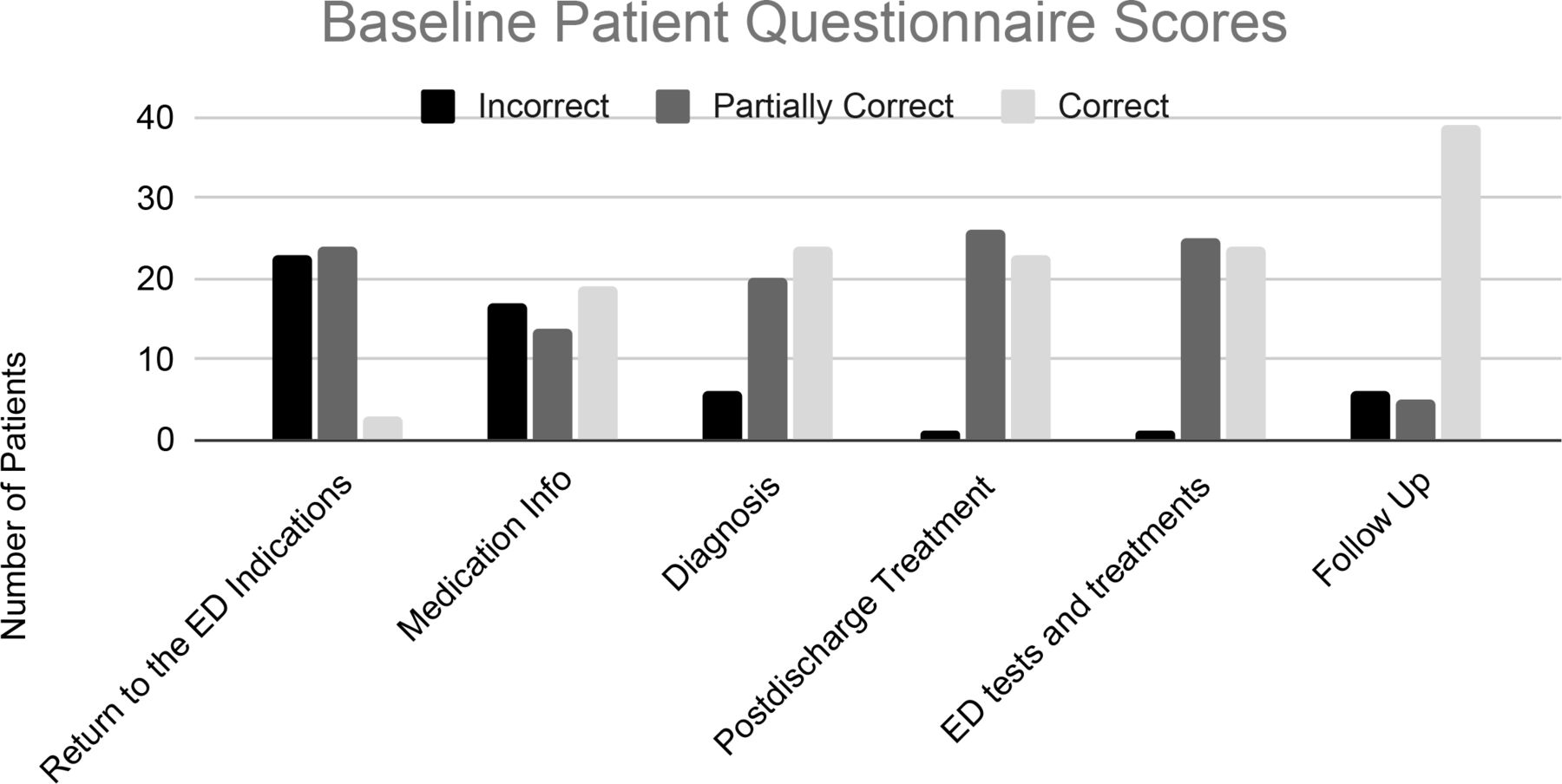
Baseline Patient Questionnaire Scores. Baseline discharge knowledge of 50 emergency depatment (ED) patients was assessed in six domains: indications to return to the ED, information about medications (frequency and duration), diagnosis, other postdischarge treatment (wound care, etc), tests and procedures performed in the ED, and follow-up (clinics to follow up with after discharge from the ED). The answers were graded as correct, partially correct or incorrect. The counts for each of these answers are presented here.
This baseline data were collected and analysed with QI tools (fishbone diagrams, driver diagram and decision matrix) to identify the root causes of lower understanding and plan the best method for improvement. Based on our analysis, we determined that the best interventional strategy was to revamp the AVS.
Using prior patient studies and educational standard practices, we developed a one-page patient discharge summary, the SIP (figure 2). We tested the SIP on a sample of 118 patients at the ED and analysed the results. Five patients declined to be interviewed, citing reasons including being in pain, having other appointments to meet, wanting to leave the ED to eat and transportation arrival.

Simplified information page. Our one-page discharge summary document written at a Flesch-Kincaid grade 5 level includes simple pictograms to act as a memory aid.
Just as in the baseline assessment, interviews were conducted in person by trained medical students at the time of discharge. The patient’s baseline knowledge was first assessed with the six question survey. Then, the patient was assisted in filling out the SIP based on information from their ‘official’ discharge packet and readministered the questionnaire. After that, three medical students compared the patient’s answers to the medical chart information and assigned the patient a score based on how closely the answers they gave matched the patient chart. Additional information collected included whether patient rating of standard discharge instructions provided, whether discharge papers were read, Emergency Severity Index (ESI) score, patient (or parent for minors) age and education level.
Design
Accessible discharge instructions that empower patients to improve their understanding should improve health literacy and patient self-efficacy, a person’s confidence in their abilities to access, understand, and assess the resources around them to promote their well-being. Self-efficacy is linked to patient empowerment and improved health outcomes.1 A study funded by the Agency for Healthcare Research and Quality found that patients who have clear understanding of their after-hospital care instructions are 30% less likely to be readmitted to the inpatient setting or visit the ED than patients who lack this information.2
At the time of the baseline survey, the discharge instructions ranged from 6 to 22 pages long. The information was not always intuitively organised, and important information was not immediately visible on the first page. For example, the new prescribed medications were first mentioned on page 5 in this AVS.
Studies in learning theory have shown that it is difficult to retain large amounts of information accumulated in a short period of time, and patients retain as little as one-fifth of the information they are given.14–16 This is especially true when people are stressed or in pain, as is the case with many people in the ED. However, healthcare providers often focus on giving comprehensive information and complete instructions. Since patients will likely not be able to remember detailed medical information, it is important to effectively focus on the key points that patients absolutely need to know, rather than everything that would be potentially beneficial to know.8
The SIP aimed to balance the dual goals of providing complete yet condensed information by distilling the large amounts of information that patients are provided into one short, easy-to-read page with simple language, pictographs, and practical emphasis of key points. We aimed to improve the readability of discharge instructions by including all necessary information for patients on the first page of the AVS. Many of the items that increased the size (and decreased readability) of the documents cannot be removed due to institutional policy. Others are useful as a reference but difficult to quickly remember.
Strategy
About half (58/118) of patients did not read or reference their discharge papers. We addressed this by providing a very simple, accessible and interactive document. Multiple content and design points were taken into consideration when creating the SIP (figure 2). We included patients’ recommendations for printed materials, both published in prior literature and elicited during our interviews. Patients request that literature provided define complex words and ideas, provide motivational information (why do this), provide practical information and examples, use visual aids, provide a logical flow of information and emphasise key points.2 14
Multiple studies have shown that the reading level of ED discharge instructions often exceeds patients’ reading and health literacy levels. It is generally recommended that ED discharge documents be written at a sixth-grade reading level; these documents are typically written at a 9–10th grade reading level.2 7 The SIP was written at Flesch-Kincaid grade level of grade 5.
In addition to writing at an appropriate grade level, adding multiple methods of learning and making the document visually appealing are important. Adding pictographs is an easy method to improve patient comprehension and draw attention to specific areas.5 15 17 ‘The SIP contains small icons for subheadings (eg, a pill for new medications, a calendar for follow-up visits needed, and a red and white emergency cross for reasons to return to the ED). The icons chosen allow some consistency with the current AVS while also making the sections easy to find. In addition, the SIP requires someone to fill out the information—this acts as an additional kinesthetic learning tool and a method of teach-back, which has been proven effective for patient discharge comprehension.18 19 Additional design points included leaving white space and avoiding lengthy text and small fonts. Finally, we wanted to make the data accessible and user-friendly, so the SIP was limited to one page in length.
It was especially important to improve the AVS as there was a small significant difference in patient knowledge between those who read and those who did not read the AVS. This is very relevant since most patients do not read the AVS, so it is important to make discharge documents easy and accessible to motivate patients to use them. Our SIP has the potential for greater effect as it was designed to specifically target the lowest-scoring areas.
We implemented the core ideas of the SIP into the cover page for the AVS/standard discharge packet. The cover page now includes pictograms, simplified follow-up and medication instructions, and a summary of the tests performed in the ED.
Results
Notably, 86/118 (73%) of the interviewed patients gave the ED staff a 10/10 rating on their standard discharge instructions they were given, saying that they understood their discharge instructions. However, median composite score was only 4 out of 6.
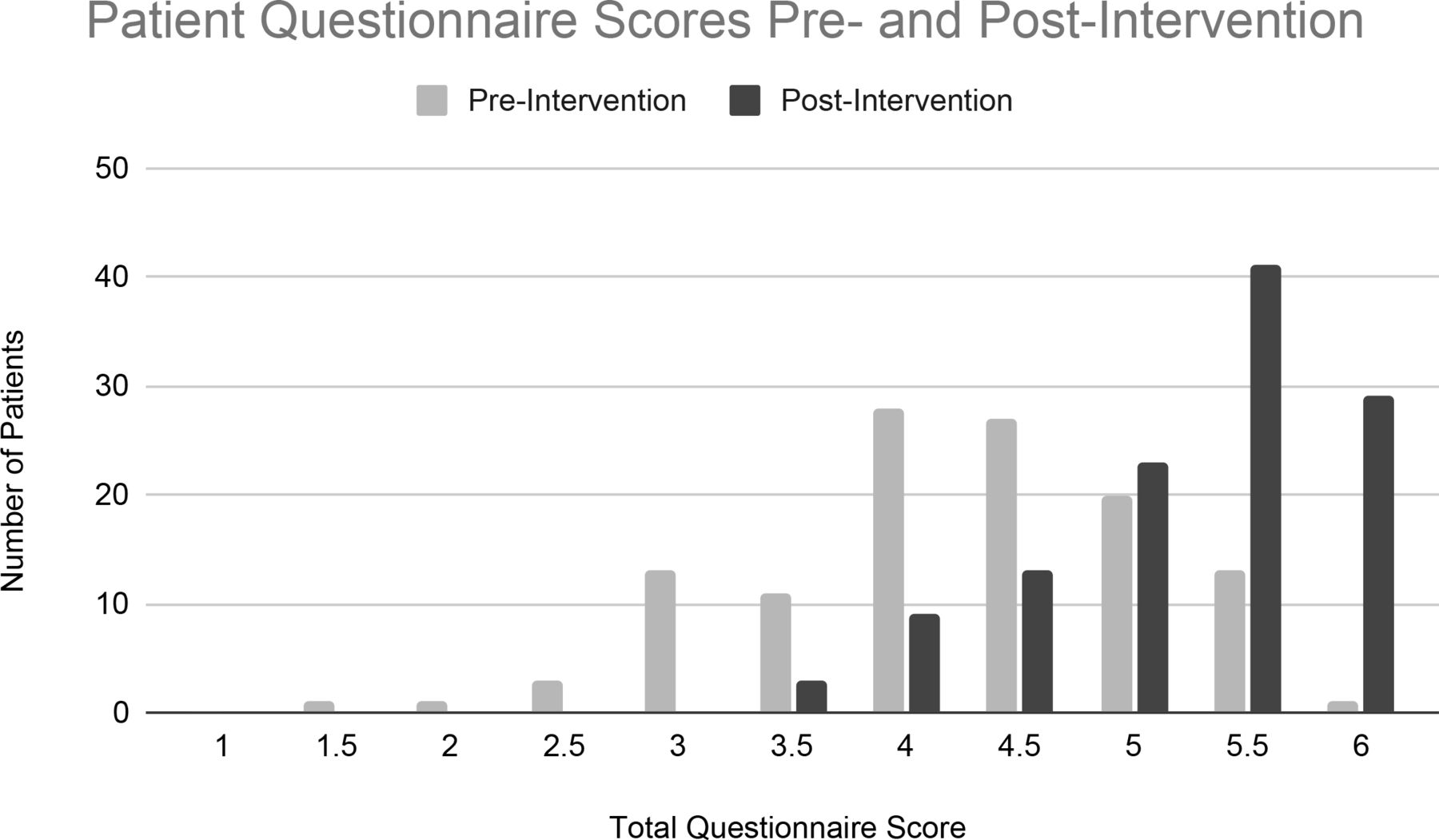
Comparison of preintervention and postintervention scores with Wilcoxon signed-rank test showed a significant change across all question categories. The change in composite scores can be seen in figure 3. The most noticeable changes occurred in the lowest-scoring initial knowledge categories: indications to return to the ED and medication details. No patients scored less than 3 points total postintervention. Median composite score improved from 4.5 preintervention to 5.5 postintervention (out of points), a change of 22%. One patient lowered their assessment of standard discharge instructions after they were given the SIP.

{kind=link}
{kind=link}
{kind=link}
Patient Questionnaire Scores preintervention and postintervention. Discharge knowledge questionnaire scores of 118 patients preintervention and postintervention after using the SIP via a teach-back method. The same domains of knowledge and scoring method were used as in the baseline questionnaire. SIP, simplified information page.
The patient population was split almost equally between people with and without college education. Most patients were presenting for acute conditions, but most of those interviewed were not severely ill as measured by their ESI score. Average age of the group was 45.6 with SD of 16.6.
Inter-rater reliability was used to measure the overall index of agreement. Each rater assigned a score for patient responses for each of the six questions preintervention and postintervention (0 for incorrect, 0.5 for partially correct and 1 for correct). The three scores were compared against each other and the mean of these scores was calculated: κ=0.84 (range 0.635–0.9449), which indicated substantial agreement in scores. This high score allowed us to conclude that the scores are adequate for assessing the data in this study.
χ2 comparison of baseline and preintervention scores was statistically significant for only one of the six questions—postdischarge treatment (p<0.01). In terms of OR, there was a 3.85 (1/0.2597) times lower odds of incorrect/partial-correct answer for the postdischarge treatment question in the preintervention compared with baseline.
The effect of demographic characteristics on patient scores was examined in the baseline and preintervention groups. We then investigated the effect of different characteristics on score improvement preintervention and postintervention. In the baseline group, age, education level, main ED provider, AVS read status and education level were analysed using χ2 and Fisher’s exact test. A statistically significant difference was found only in the category of medication frequency and duration in comparing AVS read status (p<0.01). In addition to the factors studied in the baseline group, insurance status, disease chronicity, ESI score and number of ED visits in the last 12 months were studied. χ2 analysis of these factors found no significant effect on preintervention scores based on these characteristics. Repeated measures analysis of variance test did not show any significant effect on patient score changes preintervention and postintervention based on any demographic characteristics.
After interviewing patients, we invited them to give us feedback about the SIP. We were pleased to receive a lot of positive feedback: ‘single sheet is much better,’ ‘more helpful than looking through all the paperwork; they end up in the trash,’ ‘this is great since I don’t have time to read through the regular discharge papers,’ ‘I will put it up on my fridge as a reminder,’ and ‘keeps it simple and sweet.’ Some comments were a little more neutral: ‘very helpful, but I would read the whole document anyway,’ ‘no negatives—(speaking in general) it either won’t matter or patients will be glad for more information.’ Others offered constructive criticism and recommendations: ‘discharge papers should be emailed in case the papers get lost’ (MyChart, an online healthcare record portal, is available to patients and they were informed), ‘make the print larger—older people need larger print!’ ‘I’m not a fan of duplicate or discordant instructions—think of risk implications.’ Although we encouraged patients to fill in the answers on the SIP themselves, not all patients were able to do so. Reasons for this included pain, hand injury, eye injury and learning disability, in which cases we assisted in filling out the sheet. We implemented the change of increasing the font size for the SIP.
Lessons and limitations
Our study showed that a clear majority of patients have incomplete understanding of their ED discharge instructions and that the SIP can significantly improve patient knowledge. Previous studies conducted on the topic of discharge understanding found that 78% of patients had incomplete understanding of their instructions as measured by deficiency in one or more knowledge area.8 Our preintervention analysis suggests that that number is likely higher as only one of the 168 patients interviewed had a perfect composite score without intervention. The success of our SIP attests to the idea that patient comprehension is closely related to the working memory of patients, which is improved with short, focused instructions rather than long, comprehensive and complex messages.20 It also corresponds to the idea that the best way to improve health literacy is to provide digestible information rather than simply measure each patient’s health literacy level.
Many different strategies to improve patient discharge knowledge have been attempted including video interviews, patient discharge sheets targeted towards specific diseases and structured discharge sheets. Structured presentation of information such as our SIP that includes useful instructions for follow-up and symptoms that are warning signs helped patients feel empowered and secure as well as acting as a reminder of education received in the hospital.15 17 21 Our patients provided feedback that mirrored these sentiments as well as suggested future courses of action. We created another version of the SIP with larger font size to accommodate our vision-impaired patients. One of the concerns raised was that the SIP may lead to writing different instructions than provided, but having a time for teach-back and discussion during the discharge process using information from the AVS should minimise the risk of inaccurate information. Additionally, the standard discharge instructions are always available as the ‘gold-standard’ reference.
No patient demographics (age, education, etc) were found to significantly affect patient scores or patient score improvement, suggesting that insufficient patient knowledge is a global problem that requires a global solution rather than one affecting a particular patient population. Going through the SIP with patients requires additional time from ED staff, which may affect sustainability. This has broad implications on patient outcomes as well as healthcare costs since it requires more provider time and resources. Our approach to minimise this was to incorporate the lessons we learnt on readability and accessibility using the SIP into the cover page of the standard discharge instruction packet. This reduces some of the possible benefit from active patient involvement and teach-back, which is a limitation, but creates a viable long term change.
Conclusion
Our study has shown that a simple one-page intervention can significantly increase discharge understanding through ease of use and accessibility, and we achieved our aim of increasing patient composite questionnaire score by 22%. Patients across all demographic categories benefited from the SIP, demonstrating that both the problem and solution are universal rather than specific to a particular group of patients, which makes our intervention worthwhile for the whole ED population and really all patients being discharged from a healthcare facility. Many patients do not read their discharge papers, and it is important to motivate them to read these important documents by making them as accessible as possible. Through the EHR, we applied the concepts of the SIP to create a more accessible cover page for the standard printed patient discharge packet, creating a sustainable improvement in patient discharge instructions.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
As this was a quality improvement project, IRB approval was not required. The project was approved by the University of Texas Southwestern Quality Improvement Patient Safety programme and ED Quality Improvement Committee.
References
Footnotes
Contributors CD, EP, AB and GR conceived and planned the study. CD, KJ and BS interviewed patients and compiled data. CD, EP, SM, AB and GR contributed to the interpretation of the results. CD took the lead in writing the manuscript. All authors provided critical feedback and helped shape the study, analysis and manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.