Article Text

Abstract
In the UK, over 700 000 patients are affected by pressure ulcers each year, and 180 000 of those are newly acquired each year. The occurrence of pressure ulcers costs the National Health Service (NHS) more than 3.8 million every day. In 2004, pressure ulcers were estimated to cost the NHS £1.4–£2.4 billion per year, which was 4% of the total NHS expenditure.
The impact on patients can be considerable, due to increased pain, length of hospital stay and decreased quality of life. However, it is acknowledged that a significant number of these are avoidable.
In early 2015, it was identified that for the North East and North Cumbria region the incidence of pressure ulcers was higher than the national average. Because of this, a 2-year Pressure Ulcer Collaborative was implemented, involving secondary care, community services, care homes and the ambulance service, with the aim of reducing the percentage of pressure ulcers developed by patients within their care.
The Breakthrough Series Collaborative Model from the Institute for Healthcare Improvement provided the framework for this Collaborative.
In year 1, pressure ulcers were reduced by 36%, and in year 2 by 33%, demonstrating an estimated cost saving during the lifespan of the Collaborative of £513 000, and a reduction in the number of bed days between 220 and 352.
- collaborative
- breakthrough groups
- quality improvement methodologies
- quality improvement
- PDSA
- healthcare quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- collaborative
- breakthrough groups
- quality improvement methodologies
- quality improvement
- PDSA
- healthcare quality improvement
Introduction
Problem description
Knowledge concerning the prevention of pressure ulcers is readily available, and an in-depth review into the effectiveness of current practice was undertaken by Niederhauser et al.1
Conventional pressure ulcers occur where there is a bony prominence and there is compression of the skin or underlying tissue with an external surface.2 Commonly, these conventional pressure ulcers occur on the sacrum or heel and it is estimated that this accounts for around 70% of pressure ulcers in adults.3 4 However, pressure ulcers can also develop deeper, below the surface of the skin, badly damaging the muscle or bone underneath.5 Factors increasing the likelihood of these pressure ulcers occurring are immobility, incontinence and poor nutritional status.2
Pressure ulcers are an unwanted and often avoidable complication of care6–9 that affect over 700 000 UK patients per year.6 They are a common occurrence, particularly in patients whose mobility is limited due to illness, severe physical disability or increasing frailty.7 10 11 Pressure ulcers can lead to increased mortality, morbidity and reduced quality of life for the patient.10
Pressure ulcers can also result in longer hospital stays,10 with hospital-acquired pressure ulcers increasing length of stay by an average of 5–8 days per pressure ulcer.12 In addition, they represent a substantial financial cost to local National Health Service (NHS) Trusts and care providers. In 2004, pressure ulcers were estimated to cost the NHS £1.4–£2.4 billion annually, which was 4% of the total NHS expenditure.13 In 2015, the cost per pressure ulcer was estimated to vary between £1214 and £14 108 depending on its severity.10
More than 180 000 pressure ulcers are acquired each year.7 In 2011/2012 pressure ulcers were the largest proportion of patient safety incidents, accounting for 19% of all reports.8
Available knowledge
Given the often preventable nature of pressure ulcers, the occurrence of this harm to patients is a key indicator of nursing standards.14 The National Institute for Health and Care Excellence (NICE) guidance, the Institute for Healthcare Improvement (IHI) guidance, and the Surface, Skin inspection, Keep your patients moving, Incontinence/moisture, Nutrition/hydration (SSKIN) care model (refs8 15 16, respectively) all outline how to prevent pressure ulcers. Despite these being based on scientific evidence, it is clear from the prevalence of pressure ulcers still being reported nationally17 on the NHS Safety Thermometer18 that good pressure ulcer care is not consistently embedded into nursing practice.
The National Patient Safety Collaborative, which was established in 2015 and is the largest safety initiative in the history of the NHS,19 identified pressure ulcers as one of its first priorities. The North East and North Cumbria arm of the National Patient Safety Collaborative20 welcomed this because the incidence of pressure ulcers in the region was higher than the national average.17
Rationale
The North East and North Cumbria region adopted a Quality Improvement Collaborative (QIC) approach, specifically the IHI Breakthrough Series Model.21 This approach brought together a diverse range of UK healthcare organisations from across the region, namely secondary care organisations, community services, care homes and the North East Ambulance Service.
QICs aim to bring people together, often from different organisations, to share best practice and benchmark services in focused sessions. The strength of QICs lies in the collaborative efforts to bring together peers and experts in particular fields, allowing them to share their knowledge.21 22 Currently, there is a limited amount of available evidence which can categorically link QIC programmes to improved healthcare outcomes.22 Having said that the IHI states that dramatic results have been achieved using their Breakthrough Series Collaborative Model.21
The difficulty in assessing the effects of QICs arises for a number of reasons including the frequent attempts of QIC programmes to tackle complex, multifaceted issues, making outcome measurement difficult.23 The wealth of readily available knowledge on the causes and prevention of pressure ulcers suggests that the issue lies in the implementation of this knowledge into everyday practice, and the engagement of the healthcare staff, rather than in its complexity.
Research has shown that education around pressure ulcers for nursing staff can be incomplete or is often not extensive enough in this area.24 An article by Hebert and Oakley24 outlines previous work to engage staff to reduce pressure ulcers. In this work, standardised education workshops were delivered in an interactive and enjoyable way to engage staff.24 A key outcome of this was that learning needed to be ongoing. Other studies have cited key factors such as ‘buy-in’ from providers and front-line staff as well as the celebration of achievements.4 6
The IHI Breakthrough Series Collaborative Model provides a framework for implementing a QIC,21 with this being shown in figure 1.

The Breakthrough Series Collaborative Model.
This framework outlines eight key elements: topic selection, faculty recruitment, enrolment of participating organisations and teams, learning sessions, action periods, the model for improvement, summative congresses and publications, and measurement and evaluation.21
The framework recommends that collaboratives should range in size from 12 to 160 organisational teams, with short-term interventions being implemented over a period of 6–15 months.21 As figure 1 highlights, participants attend three learning sessions during the lifespan of the collaborative, and implement their learning between sessions, using the model for improvement methodology.
Specific aims
The primary aim of the Pressure Ulcer Collaborative was to reduce the percentage of pressure ulcers in participating teams across the North East and North Cumbria by:
50% in year 1 (over 12 months, July 2015 to June 2016).
20% in year 2 (over 9 months, March 2017 to November 2017).
Methods
Context
Thirteen healthcare organisations across the North East and North Cumbria were involved in year 1, and 10 in year 2, with eight of the organisations involved in year 1 also taking part in year 2, although the majority of teams within these organisations were different.
Organisations involved in this Collaborative were from secondary care, community services, care homes and the ambulance service. From secondary care and community services the vast majority of teams were ward based (trauma, orthopaedics, vascular, respiratory, palliative, surgical, medical, continuing care, cancer, complex mental and physical health, diabetes, elderly and gastroenterology) but three district nursing teams were also involved in year 1.
Although the diversity of these teams was recognised, as the principles of good pressure ulcer care remain the same, it was felt that this diversity would add a richness to the Collaborative, rather than it being a limiting factor.
Interventions
This Collaborative was initially planned to run for 1 year only. However, following completion of the first year, it was felt that there was scope to build on this learning, and therefore the Collaborative ran for a further year, with a 6-month gap between year 1 and year 2. This gap allowed for recruitment of teams and gave them the opportunity to collect their baseline data.
A description of the Collaborative structure and actions, using the key elements of the IHI Breakthrough Series Collaborative Model (outlined in ‘Rationale’), is described below:
A specific topic
The reduction of pressure ulcers was chosen because of their preventability, coupled with the fact that the North East and North Cumbria region was reporting a higher incidence of pressure ulcers than the national average.
Faculty recruitment
A faculty of six national and international experts were recruited to provide knowledge of pressure ulcer prevention and quality improvement. This included three experts from the South Eastern Health and Social Care Trust in Northern Ireland who had been involved in running a Pressure Ulcer Collaborative for 6 years, with some excellent results.
Enrolment of participating organisations and teams
The Director of Quality and Transformation at South Tyneside NHS Foundation Trust and City Hospitals Sunderland NHS Foundation Trust, who led on this Collaborative, used pre-existing relationships with healthcare organisations in the region to build a commitment to reducing pressure ulcers in North East and North Cumbria. Information days were also held, before the start of each Collaborative year, and representatives from all trusts were invited to attend.
The number of staff in each Collaborative team was not specified, due to the varying sizes of the teams involved. This meant that Collaborative team size varied from three to eight members of staff.
Learning sessions
Three 1-day learning sessions were delivered during each year of the Collaborative. These were held in the North East. The purposes of these sessions were so attendees could learn from the experts regarding pressure ulcers and quality improvement, share their own experiences and learn from their peers, and decide on next steps.
Action periods and the model for improvement
Implementation of learning took place between sessions, with these being referred to as action periods. During the action periods, the Faculty provided support via visits, email, telephone and webinars. Also, teams involved in year 2 received a copy of ‘The Improvement Guide: A Practical Approach to Enhancing Organizational Performance,’25 as well as a process mapping guide developed by the Academic Health Science Network for North East and North Cumbria.
The model for improvement methodology was used by teams during the action periods to implement change:
Plan-Do-Study-Act cycle 1 following learning session 1
Participants undertook local adaptation of existing models such as SKKIN.16 Progress was continually evaluated and led to improvements being made within the majority of participating teams.
Time was taken to understand what the key factors were to successful implementation, which included a patient safety culture and good leadership.
Some teams did struggle with implementation, stating that it was time consuming and staff shortages were making it challenging to implement. On investigating further, it did become clear that culture and leadership were also underlying causes.
Stakeholder analysis26 was undertaken within these teams, and then the levers/benefits for implementing good pressure ulcer care for these staff were identified. Time was also considered, and information was shared with individuals and teams regarding the extra time patients can stay in hospital because of acquiring a pressure ulcer, and the impact this can have within a healthcare setting. In addition, the increased costs and number of bed days associated with not providing good pressure ulcer care were used to accelerate staff recruitment. From this a process of winning hearts and minds took place, with some success.
Plan-Do-Study-Act cycle 2 following learning session 2
As all participating teams started the Collaborative with varying levels of pressure ulcer interventions and care in place, learning session 2 had a focus on shared learning.
Participating teams were asked to consider implementing interventions shared by other teams and national and international experts. Ideas included, but were not limited to, the implementation of pressure ulcer clocks, training of staff (both face to face and via e-learning), adding body maps to admission checklists, optimisation of nutrition and hydration and involving patients and carers.
This approach was successful as it enabled teams to identify tests of change within their own local setting.
Plan-Do-Study-Act cycle 3 following learning session 3
Considerable emphasis was given to sustainability throughout years 1 and 2 of the Collaborative, with teams being asked to consider sustainability when they were identifying ideas and approaches for change. Learning session 3 built on this, with teams being asked to use the Institute for Innovation and Improvement (2007) Sustainability Model27 to assess the likelihood of sustaining their changes, and from this identify areas which needed further attention. Action plans were subsequently developed to remove/reduce the barriers/challenges identified.
One of the issues highlighted during this Plan-Do-Study-Act (PDSA) cycle was that a small number of teams felt some matters were outside of their control, particularly regarding behaviours of some staff. Discussions took place with these teams regarding focusing on what they could influence, and also developing strategies for raising concerns.
Summative congress and publications
Celebration events were held at the end of each Collaborative year where teams shared their progress and data via videos and storyboards. These were excellent events as they enabled teams to take time out to consider their own achievements, but also to continue learning from others.
Measurement and evaluation
Participating teams were asked to submit data each month on the number of pressure ulcers. See ‘Measurement’ for more information.
Study of the interventions
It was clear early on in this Collaborative that each team involved already had interventions in place regarding pressure ulcer prevention and care. What was also apparent was that the number of interventions and the impact of these varied considerably across teams, as did the challenges and barriers they faced. It was therefore felt that, during the lifespan of the Collaborative, the ‘what’, ‘how’ and ‘when’ interventions were implemented would very much depend on the individual team context. It was acknowledged that from an overarching Collaborative perspective this would make assessing the impact of interventions challenging, but was felt necessary to meet the needs of participating teams.
It was hoped that adopting the IHI Breakthrough Series Collaborative Model would provide a framework which was structured enough to foster a supportive environment for learning and building capability, but flexible enough for teams to identify and implement those interventions which they felt would have maximum impact in their local setting/context.
To assess this, at the end of each Collaborative year a survey was circulated to all those involved to measure the impact of the approach adopted, which enabled both qualitative and quantitative evaluation.
Measures
Number of pressure ulcers
The aim of this Collaborative was to reduce the number of pressure ulcers in participating teams across the North East and North Cumbria by:
50% in year 1 (over 12 months, July 2015 to June 2016, with baseline data being collected in the 3 months prior to this).
20% in year 2 (over 9 months, March 2017 to November 2017, with baseline data being collected in the 3 months prior to this).
In year 1, a 50% reduction aim was chosen because, although it was recognised that this would be challenging, it was anticipated that some teams would rise to the challenge. In year 2, the percentage aim was reduced because for some teams the aim in year 1 had proved too ambitious and if it had remained the same it may have impacted on recruiting teams for year 2.
The number of pressure ulcers was collected by participating teams and then translated into a percentage by the Faculty to assess achievement against the aims. For each year, the percentage reduction is based on the mean from the 3-month baseline data compared with the mean from the final 3 months of data collected.
Although it would have been preferable to have had a longer baseline data collection period, as these data were not readily available, and to keep momentum, baseline data were collected for a period of 3 months for each year of the Collaborative.
Teams only submitted data regarding ‘avoidable’ pressure ulcers, which are those acquired while the patient was in their care. They were not asked to submit ‘unavoidable’ pressure ulcers as these are those not acquired while the patient was in their care, and would therefore not have been indicative of that team’s quality of care.
Teams were asked to record the number of pressure ulcers, rather than prevalence or incidence rate, to simplify the data collection process. This is therefore different from that collected in the nationally implemented Safety Thermometer which measures prevalence.17 Measuring prevalence allows the total number of pressure ulcers in a particular area to be recorded. However, as data are collected on a particular day, once a month, this could mean that the same pressure ulcer may have been recorded more than once if the patient had a pressure ulcer for more than 1 month. Collecting the incidence of pressure ulcers would have enabled teams to understand the rate of occurrence of pressure ulcers.
Pressure ulcers are graded with increasing severity from categories 1–4, according to the European Pressure Ulcer Advisory Panel classification system.28 Teams were not asked to specify the grade of pressure ulcer to simplify the data collection process by teams. In year 1, teams were asked to submit the number of pressures from grades 1–4, and in year 2 grades 2–4. This change was made in year 2 because some organisational policies did not require teams to collect grade 1, and therefore aligning the data collection to that already in place simplified the process. It was also hoped that this would increase data submissions.
Teams were encouraged to use a safety calendar to record and monitor the number of pressure ulcers in their ward/area. The safety calendar is a normal calendar (sometimes shaped as a cross) labelled with the day of the month. When a pressure ulcer is classed as ‘avoidable’ this is coloured red on the safety calendar, and yellow when a pressure ulcer is classed as ‘unavoidable’. This method of data collection was chosen as it is simple to record, in real time, and easy to view, thereby encouraging front-line teams to take ownership of the data.
Collecting the number of pressure ulcers enabled cost impact and bed days saved to be calculated:
Cost impact
This was assessed using the Department of Health and Social Care Pressure Ulcer Productivity Calculator.29 The calculator attributes a cost to pressure ulcer care based on the grade of the ulcer and the accompanying complications that arise. As pressure ulcer grades were not recorded by teams for this Collaborative, it has been impossible to identify the actual cost. However, an estimate can be gained if all costs are based on grade 2 pressure ulcers using, for each year, the 3-month baseline data collected and the final 3 months’ data collected. Two caveats should be attached here. First, as the Pressure Ulcer Productivity Calculator is based on the estimated cost of pressure ulcer care at 2008/2009 prices, the costs now will inevitably be higher. Second, for this study the calculation is based on grade 2 pressure ulcers. The costs for a grade 1 pressure ulcer are minimal (approximately £1000) compared with that for grades 2, 3 and 4 (approximately £3000, £4000 and £6000, respectively), and it was therefore felt that basing this calculation on grade 2 pressure ulcers would provide the best estimate, although it is acknowledge that this is imprecise.
Bed days saved
This was calculated on the number of bed days saved based on the NICE Guidance Costing Statement on pressure ulcers,12 which states that hospital-acquired pressure ulcers increase the length of stay by an average of 5–8 days per pressure ulcer. With all non-ward-based data being removed (district nursing teams and care homes) the calculation for each year is based on 3-month baseline data compared with the final 3 months’ data collected.
Survey evaluation of approach adopted
Staff were asked to complete a survey, which sought to gain both quantitative and qualitative feedbacks, to understand what has supported as well as hindered the success of this Collaborative.
The survey for year 2 differs from that for year 1. The number of questions was reduced, and also reworded in places. This was to increase the number of surveys completed in year 2.
Both surveys were circulated at the end of each Collaborative year, in electronic form in year 1 and electronic and paper form in year 2.
Analysis
Reduction in the percentage and number of pressure ulcers
Run charts, using the IHI interpretation,30 have been used to demonstrate the reduction in the number of pressure ulcers. This approach was chosen as it enables consideration of special and common cause variation. Ideally, a far longer baseline data collection period would have taken place to support the validity and reliability of the findings because with only three data points for each Collaborative year it cannot be ascertained whether the baselines are demonstrating random variation or whether there were already interventions happening which impacted on these data.
Survey evaluation of approach adopted
The use of surveys enabled an analysis of the overall impact of the Collaborative. The quantitative questions identified the percentage impact, whereas the qualitative questions enabled causal analysis to be undertaken to understand why people answered in the way they did.
Ethical considerations
Potential ethical issues were considered in the design and implementation of this Collaborative. Although the number of pressure ulcers was shared with the Faculty by participating teams, patient identifiable information was not. Within the teams/organisations themselves they adhered to their own ethical policies and procedures.
Results
Data submission by teams
In year 1, thirteen teams spanning five organisations submitted data. In year 2, twenty-five teams spanning nine organisations submitted data. The only organisation/team who did not submit data in year 2 was the North East Ambulance Service NHS Foundation Trust. This was because patients only spend a very short time in the care of the ambulance service and it would therefore not have been possible to determine whether a pressure ulcer was ‘avoidable’ in these circumstances.
Reduction in the percentage and number of pressure ulcers
The percentage/number reduction in pressure ulcers in year 1 was 36%/48 and in year 2 was 33%/38.
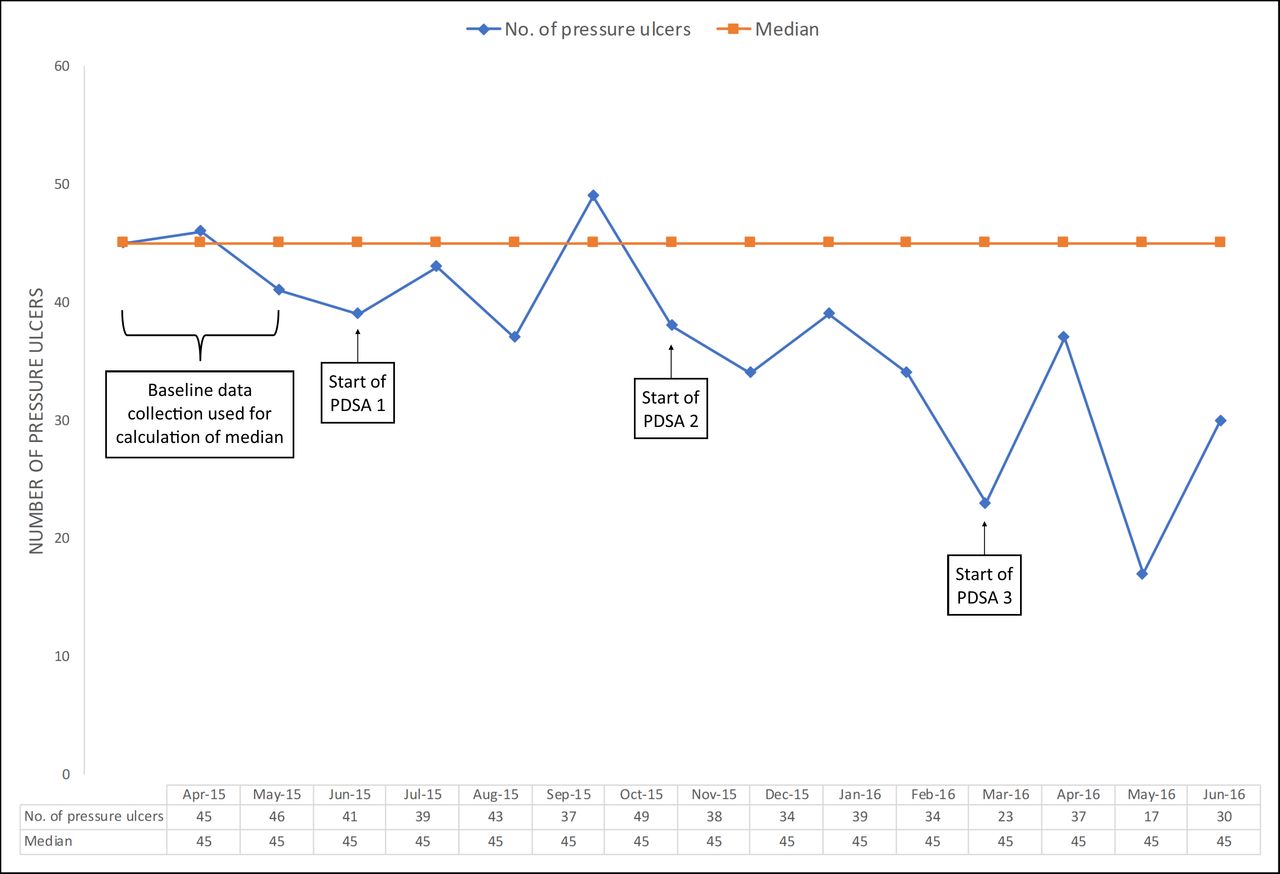
Figure 2 demonstrates that following the baseline data collection period there is a ‘shift’ (which is where there are six or more data points below or above the median line). Therefore, if the assumption is made that the baseline data are random, this graph suggests special cause variation, where the changes implemented have generated a change which is sustainable over time.

Year 1—number of pressure ulcers (monthly). PDSA, Plan-Do-Study-Act.
Figure 3 also demonstrates a ‘shift’, but this forms part of the baseline data and therefore before the start of PDSA 1. Due to only three baseline data collection points being available, it is not known whether this is part of random variation or whether it is special cause variation. There is also no evidence of special cause variation following the start of the PDSA cycles. There are reasons which could possibly be attributable to the reduction from January 2017. An engagement event was held not long before the start of the baseline data collection period, where the success stories from those involved in year 1 were shared. Some teams may have taken this learning and implemented changes before the start date of year 2. Also 8 of the 13 organisations involved in year 1 went on to take part in year 2. Although the majority of teams within these organisations changed in year 2, there may well have been some internal organisational dialogue/sharing because of increased interest gained at the engagement event, again resulting in changes being implemented before the start of year 2.

{kind=link}
{kind=link}
{kind=link}
Year 2—number of pressure ulcers (monthly). PDSA, Plan-Do-Study-Act.
Estimated cost impact
Based on all pressure ulcers being grade 2, the Pressure Ulcer Productivity Calculator suggests that:
Year 1: with a 36% reduction in pressure ulcers there has been a cost saving in the region of £284 000.
Year 2: with a 33% reduction in pressure ulcers there has been a cost saving in the region of £229 000.
Estimated total cost saving during the lifespan of the Collaborative: £513 000.
Estimated reduction in bed days
Based on the view that hospital-acquired pressure ulcers increase the length of stay by an average of 5–8 days per pressure ulcer,12 and removing all data submitted by teams on non-hospital wards, it can be calculated that:
Year 1: there was a reduction of seven hospital-acquired ‘avoidable’ pressure ulcers, therefore, bed days saved is between 35 and 56.
Year 2: there was a reduction in 37 hospital-acquired ‘avoidable’ pressure ulcers, therefore, bed days saved is between 185 and 296.
Estimated total reduction in number of bed days during the lifespan of the Collaborative: 220–352.
Findings from the surveys
Year 1—key points:
A total of nine members of staff responded to the survey.
Around half (55%) felt the Collaborative had allowed them to make a positive impact on the number of pressure ulcers in their ward/area.
Seventy-eight per cent said the Collaborative had empowered them to make a difference in reducing the number of pressure ulcers within their ward/area.
Eighty-nine per cent felt more knowledgeable about quality improvement.
The majority (67%) said they had been able to engage patients and carers in the process.
Year 2—key points:
A total of 23 members of staff responded to the survey.
One hundred per cent said the changes they and their team had implemented through the Collaborative had made a positive difference to pressure ulcer care.
Ninety-one per cent felt the Collaborative had empowered them to make a difference in reducing the number of pressure ulcers. Feedback given from one of the two people who did not answer this way stated that it was ‘already part of job role.’
Ninety-six per cent felt more knowledgeable and capable of carrying out quality improvement work. The one person who did not feel this way stated that they ‘already had knowledge of quality improvement techniques.’
Eighty-three per cent had engaged with patients and their families to prevent/reduce the impact of pressure ulcers during the Collaborative. Half of the 17% who had not done this said this was because they had no direct patient contact.
When asked to rate their overall experience of the Collaborative (based on very poor, fairly poor, neither poor nor good, fairly good, very good) 91% described this as either fairly or very good (48% and 43%, respectively). No one rated their experience as very poor or fairly poor, but the feedback from one of the two people (9%) who rated their experience as ‘neither poor nor good’ stated that ‘We didn’t get much support from the Trust, that is, Tissue Viability Link.’
Learning from qualitative feedback for years 1 and 2:
The learning sessions are an excellent way of bringing people together for sharing knowledge and expertise on a particular topic area.
Having the time out to attend the learning sessions is highly valued by those involved.
Being part of a Collaborative can act as a lever to galvanise teams to work together between learning sessions.
Support at senior levels within the organisations/teams is very important, and when this is not evident sustainability can be challenging.
Making time for improvement is always difficult, and therefore having a meaningful narrative to win hearts and minds is imperative.
Recognise that not everyone will want to be involved, but focus efforts on those who do.
There is sometimes apprehension about engaging with patients and families in improvement work. One of the reasons for this is that some staff feel they should be viewed as experts and think that asking patients and families for help might be viewed negatively. However, those staff who do have found it a worthwhile experience.
The celebration events are a key part of the process in terms of rewarding teams for their work so they feel empowered to continue when the Collaborative comes to an end.
Discussion
Summary
What has been demonstrated by this study is that during the lifespan of the Collaborative across the North East and North Cumbria region, even though the aim of 50% was not achieved in year 1, the aim of 20% was surpassed in year 2, and there has been a substantial reduction in the percentage/number of pressure ulcers (year 1: 36%/48, year 2: 33%/38). The reduction in pressure ulcers also indicates an estimated cost saving in the region of £513 000 and reduction in the number of bed days of between 220 and 352. These are significant achievements given that pressure ulcer care is a key indicator of nursing standards.14
The analysis of the survey results demonstrates that for most of those who completed the survey they felt pressure ulcer care had improved as a direct result of being involved in this Collaborative, and as individuals they felt more knowledgeable, empowered and more able to improve pressure ulcer care.
Therefore, it is suggested that the Collaborative approach adopted, based on the IHI Breakthrough Series Collaborative Model,21 proved to be structured enough to foster a supportive environment for learning and building capability, but flexible enough for teams to identify and implement those interventions which they felt would have maximum impact in their local setting/context.
Interpretation
There is a wealth of information written about how to prevent pressure ulcers, such as NICE guidance, IHI guidance and the SSKIN care bundle (refs 8 15 16, respectively), but a high number of pressure ulcers are still being reported nationally. This suggests that it is not just about providing support/information on ‘what’ to do, but a considerable emphasis is also needed on ‘how’ to do it within individual organisations and teams.
A diverse range of organisations/teams were involved in this Collaborative. Factors including leadership, culture, buy-in and time will have influenced their results, as will the fact that the organisations/teams themselves identified and implemented changes which they felt would achieve the most impact within their own environments, rather than the Collaborative Faculty being prescriptive. The diversity of the teams involved and the range of the challenges they faced has enabled the ‘what’ to be shared and ‘how’ this can be done, which has brought a richness to the Collaborative, which could potentially have proved to be a limitation.
Limitations
Data collection and analysis
Teams were asked to submit the number of pressure ulcers on a monthly basis, rather than using the prevalence data available through the Safety Thermometer. This means the data collected are not directly comparable to nationally collected data, which is a limitation in comparing the results of this study to a wider data set, which could have been used as a control group.
The Collaborative did attempt to measure pressure ulcers in the simplest possible way to make the process easy and convenient for staff working within busy ward/area environments, with the view to increasing the participation of the teams involved. However, not including the grade of pressure ulcers was a limitation in understanding the precise impact this study has had on patient care as well as costs, as there may have been a reduction in the more severe grades of pressure ulcers (grades 3 and 4) but this information was not captured.
Changing the data collection requirements for year 1 (grades 1–4) and year 2 (grades 2–4) again makes understanding the true impact of the Collaborative challenging. However, this change was made to ensure data were collected in line with the majority of organisational policies and to increase data submissions.
Not all year 1 teams collected data for the purpose of this Collaborative. This is a limitation for these teams in understanding whether the changes they made resulted in the most positive outcome. In addition, it made it difficult to share their learning with other teams as they did not have the data to support their assumptions. It has also been a limitation for the Collaborative in understanding overall impact.
Due to interpretation of the pressure ulcer categories by teams there may be discrepancies in the recording, however, so long as each team was recording the number of pressure ulcers consistently this should not affect the overall reduction presented.
The use of surveys proved beneficial in understanding staff views on the Collaborative, but it would have been useful to have had before and after surveys undertaken at the start and end of each Collaborative year to further help in understanding impact.
Design of the Collaborative
The Collaborative was purposely designed so the organisations/teams themselves decided what to implement and when the right time was to do this, taking into consideration their local context, rather than the Collaborative Faculty being prescriptive. This supported implementing change within a diverse range of organisations/teams but has the limitation that it is difficult to understand which interventions reaped the most benefit within certain settings.
Sustainability
Sustainability was given considerable emphasis throughout years 1 and 2 of the Collaborative to support the likelihood of changes in practice becoming ‘the way we do things round here’ within participating teams. The individual teams will know whether their interventions have been sustained within their own working environment. However, since the end of the Collaborative, regionally no assessment has been made as to which interventions have been sustained in the longer term and what factors have aided/prevented sustainability. This is a limiting factor because this information could be useful for other teams/organisations who are trying to reduce pressure ulcers across the region and beyond.
Conclusions
This Collaborative has proved to be successful in reducing the percentage of pressure ulcers across North East and North Cumbria, by 36% in year 1 and 33% in year 2. This reduction demonstrates potential cost savings of £513 000 and reduction in bed days between 220 and 352. Therefore, this Collaborative has improved patient care.
Its success is attributable to adopting the IHI Breakthrough Series Collaborative Model. It is acknowledged that there can be difficulty in assessing the effectiveness of QICs, particularly when the chosen topic is complex and multifaceted.23 However, for pressure ulcer prevention there is a wealth of knowledge readily available, and the issue lies in the implementation of this.
This Collaborative enabled teams from 13 organisations in year 1, and 10 organisations in year 2, to learn and share together and also learn from national and international experts in pressure ulcer care and quality improvement. This supported teams in making informed decisions about what would improve pressure ulcer prevention in their own working environment, along with the quality improvement skills to make this happen.
Due to the diverse range of organisations involved in this Pressure Ulcer Collaborative (namely secondary care, community services, care homes and the ambulance service) it is suggested that this approach to pressure ulcer care could and should be adopted in other health and social care environments.
The focus on sustainability was introduced at the start of each Collaborative year, and discussed throughout. In addition, the expectation was clearly made that those teams involved in the Collaborative would share and spread their learning to other teams within their organisations. So, although the impact of sustainability and spread are outwith the findings of this study, it would be useful to revisit this in the future.
Acknowledgments
We acknowledge all the teams who took part in this collaborative for all their hard work. We thank our colleagues from Ireland, Brenda Carson, Linda Kelly, Nichola Gullen and Fionnuala Gallagher, for presenting and sharing their knowledge and experience of pressure ulcers and quality improvement. This approach and the outcomes of this work have also been published on the AHSN Network website.
References
Footnotes
Contributors JW was responsible for the overall content and is the guarantor of this study. BB and AB designed the collaborative. BB, AB and JW designed and delivered the learning sets. KS, JW, APR and SC were responsible for the data analysis. AMBCC managed the collaborative. JW, AMBCC, KS and SC supported the writing of the manuscript. JW and AMBCC were responsible for editing the manuscript.
Funding Funding was provided by the Patient Safety Collaborative National Programme, with the organisation and management of the Collaborative being delivered in partnership with the Patient Safety Collaborative and the Academic Health Science Network in the North East and North Cumbria.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Trust-specific data were submitted by teams involved to the faculty team, as they collected the data at source.