Article Text

Abstract
Background The surgical post-take ward round is a complex multidisciplinary interaction in which new surgical patients are reviewed and management plans formulated. Its fast-paced nature can lead to poor communication and inaccurate or incomplete documentation with potential detriment to patient safety. Junior team members often do not fully understand the diagnosis and management plan.
Aims The aims of this project were to improve both communication and documentation on the surgical post-take ward round, influencing patient safety.
Methods The ward round was deconstructed to identify individual roles and determine where intervention would have the most impact. Ten important points were identified that should be documented in the management of an acute surgical patient; observations, examination, impression, investigations, antibiotics, intravenous fluids, VTE assessment, nutrition status, estimated length of stay and ceiling of treatment. A ‘Take Ten’ checklist was devised with these items to be used as a ‘time out’ after each patient with the whole team for discussion, clarification and clear documentation. Four plan do study act cycles were completed over a period of a year. A retrospective review of post-take documentation preintervention and postintervention was performed, and the percentage of points that were accurately documented was calculated. For further clarification, 2 weekends were compared—one where the checklist was used and one where it was not.
Results Results showed documentation postintervention varied between categories but there was improvement in documentation of VTE assessment, fluids, observations and investigations. On direct comparison of weekends the checklist showed improved documentation in all categories except length of stay. Junior team members found the checklist improved understanding of diagnosis and management plan, and encouraged a more effective ward round.
Conclusion The ‘Take Ten’ checklist has been well received. Three years on from its inception, the checklist has become an integral part of the post-take ward round, thanks to the multidisciplinary engagement in the project.
- patient safety
- quality improvement
- checklists
- surgery
- teams
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
The Royal United Hospital, NHS Foundation Trust, Bath, (RUH) is a busy district general hospital, providing secondary healthcare for 500 000 people across the South-West of England. The surgical take is busy and varied. Two consultant-led, post-take ward rounds take place each day in the surgical assessment unit (SAU), a 19-bed admissions unit that takes direct admissions from general practitioners and the emergency department. The bays are overseen by a ward manager (senior nurse), and three to five staff nurses with an equal number of healthcare assistants.
The daily ward rounds include the team of junior doctors on the take that day, as well as a senior SAU nurse. Because of the fast-paced nature of the ward information may not be documented or communicated effectively, and this can impact on patient safety. There is also a degree of variability in the way the ward round is conducted, depending on the lead consultant for that round.
Background
The ward round remains an essential part of the patient journey, acting as a key interaction, allowing for patient review and senior level decision-making. However, it can often feel rushed and lack necessary team members due to time pressures, other clinical commitments and rota limitations.
Several groups have studied the relationship between quality of ward rounds and patient outcomes, including Pucher et al1 who reported significant variability in ward round quality. They found that 41% of complications in surgical patients could have been diagnosed earlier or even prevented with more thorough ward rounds.1
The SWIFT Study2 looked at the impact of compliance with the European Working Time Directive and increased shift working on junior doctors' knowledge of newly admitted patients. It found that clerking the patient and attending the post-take ward round improved junior doctors’ knowledge of patient diagnosis and management plan. Reliance on a handover sheet for this information gave a significantly poorer score.2 This study highlights the importance of the post-take ward round for junior doctor understanding and the need for high quality documentation of patient plans.
A joint report from the Royal College of Physicians and the Royal College of Nursing3 released in 2012 recognises the importance of the ward round, and outlines ways to improve both its safety and efficiency. They recommend safety checklists to minimise errors and ensure full team participation, as well as advocating thorough and accurate documentation. They recognise the need for cultural change to implement increased ward round efficiency, and the importance of senior engagement.3 The latter is echoed in a recent multicentre study of surgical ward rounds, which found that less than 50% were conducted by consultants.4
Implementation of the WHO Surgical Safety Checklist has shown to reduce morbidity and mortality in surgical patients.5 The emergency laparotomy boarding pass has been implemented at RUH. It is part of the Emergency Laparotomy Pathway Quality Improvement Care Study for improving patient mortality after emergency laparotomy which has shown an overall reduction in mortality for these patients.6 Outside of medicine, checklists are used in several industries to improve safety in the workplace, most notably in aviation.7
Baseline measurement
The project was carried out by foundation year one (FY1) doctors on their acute surgical rotation. It was supervised by a consultant general surgeon, and consultation and input was sought from the ward manager and senior nursing team. During the 3 years that the project has run, one of the initial junior teams has remained at the hospital, and two further foundation doctors have been recruited. In this time, SAU has also been relocated as part of larger hospital-wide renovations.
The post-take ward round was deconstructed to identify individual roles of team members, and to see where an intervention would have most impact. A process map (figure 1) highlighted where communication and documentation of the management plan may be missed, and identified the role of FY1 in the ward round. It also highlighted the occasions during which they may be absent from key decision-making discussions that is, when getting imaging reports or requesting investigations.
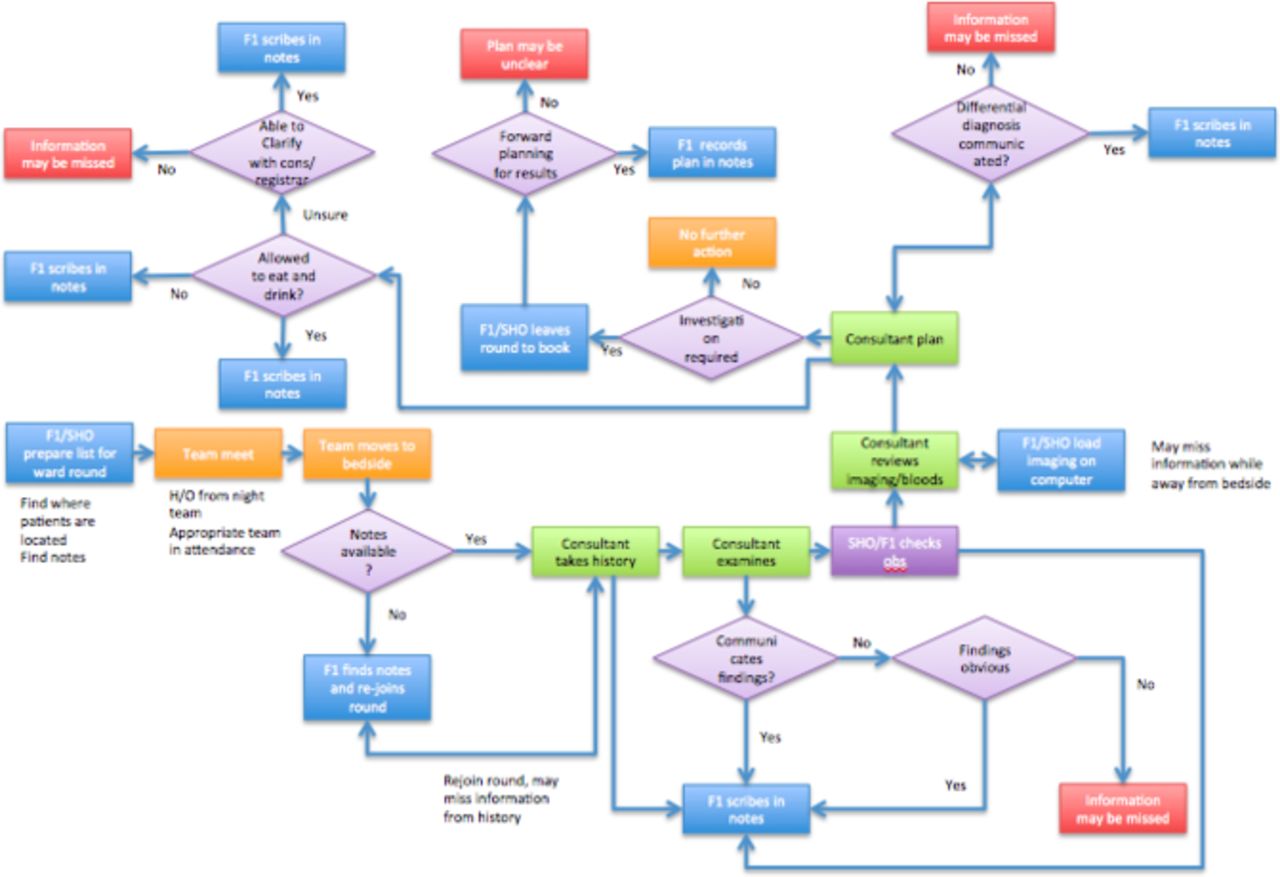
A process map of the post-take surgical ward round. F1, foundation year one doctor, H/O, handover; obs: observations; SHO: Senior house officer.
Junior doctors were informally surveyed to gather their experience of the post-take ward round. Feedback included ‘Unequal work load and responsibility’, ‘Rushed’, ‘Chaotic at best, dangerous at worst’ and ‘Unclear why investigations are being asked for’.
Based on our own knowledge of the surgical take process, in consultation with our consultant supervisor, 10 important points that should be documented in the assessment and management of an acute surgical patient were identified. These points were identified as those which form the initial patient assessment, and those which influence the ongoing patient journey. Clarification and documentation of these points at the initial post-take ward round, ensure all those involved in the patient’s care are aware of the working diagnosis and management plan. The points also allow for senior assessment of important decisions such as Venous thromboemolism (VTE) prophylaxis, antibiotic choice and nutritional status, as well as discussion of resuscitation status. It was felt that 10 points would allow a timely discussion, while ensuring all the important points for further management had been discussed.
A retrospective analysis of 31 patient notes from surgical admissions in April 2014 was undertaken over three separate weeks. Data were collected from the post-take ward round section in the RUH acute surgical admission proforma. The notes of patients seen on the post-take ward rounds that day were selected and assessed on SAU only. These were not formally randomised, but selected as a ‘snapshot’ of each take. The average number of patients seen on a weekly take is 115. This is calculated from data from our online referral system.
The 10 points assessed were:
Observations
Examination
Impression
Investigations
Antibiotics
Intravenous fluids
VTE risk assessment
Nutrition status
Estimated length of stay
Ceiling of treatment
Design
Following consultation with the senior nursing and clinical teams in SAU, a checklist was devised. The ‘Take Ten’ checklist included the 10 important points previously identified, and aimed to initiate a ‘time out’ after each patient, in which these points could be discussed within the multidisciplinary team. Ideally it would be led by the most junior member of the team and the plan from that discussion would be clearly documented in the patient notes.
Inclusion of these 10 points in the patient notes, in the form of a sticker or proforma was also considered. After discussion, it was agreed that this would create more paperwork, and may be completed without discussion. It was felt that the checklist would initiate discussion within the team and increase understanding of the management of each patient by all team members.
The checklist was printed on A4 paper and laminated. Initially 10 checklists were made and kept in the SAU office where handover takes place. The aim of the checklist was to improve documentation at the post-take ward round. This was measured as a mean proportion of points successfully documented, in subsequent data collection cycles.
Strategy and improvement cycles
Plan do study act (PDSA) cycle 1
Baseline data collected April 2014 (n=31).
Use of the checklist was initiated on the ward following baseline data collection. To promote use of the checklist, a presentation was given to all surgical consultants and registrars at the monthly audit meeting. The checklist was introduced to the F1s at their hospital induction, and it was discussed with staff nurses at their monthly meeting.
PDSA cycle 2
Further collection of data June 2014 (n=24), and comparison with baseline data. Weekend comparison data (n=18) were collected for presentation to surgical consultants to further encourage use of the checklists.
Data were presented to the surgical directorate, and feedback received from consultants and registrars on use of the list. An anonymous survey was designed to collect feedback from junior doctors using the checklist
Further data collection October 2014 (n=27).
PDSA cycle 3
The checklist was amended based on feedback from users. Length of stay was replaced with drug chart review, and the hospital logo added to the checklist. The number of checklists available on the ward were increased, and the checklists were moved to the patient bedside to encourage use. A lunchtime meeting was held on SAU with nursing staff, and a feedback session held at the beginning of weekly F1 teaching. These meetings aimed to explore barriers to use of the checklist and encourage whole multidisciplinary team (MDT) involvement.
Further data collection April 2015 (n=26) and February 2017 (n=20).
Results
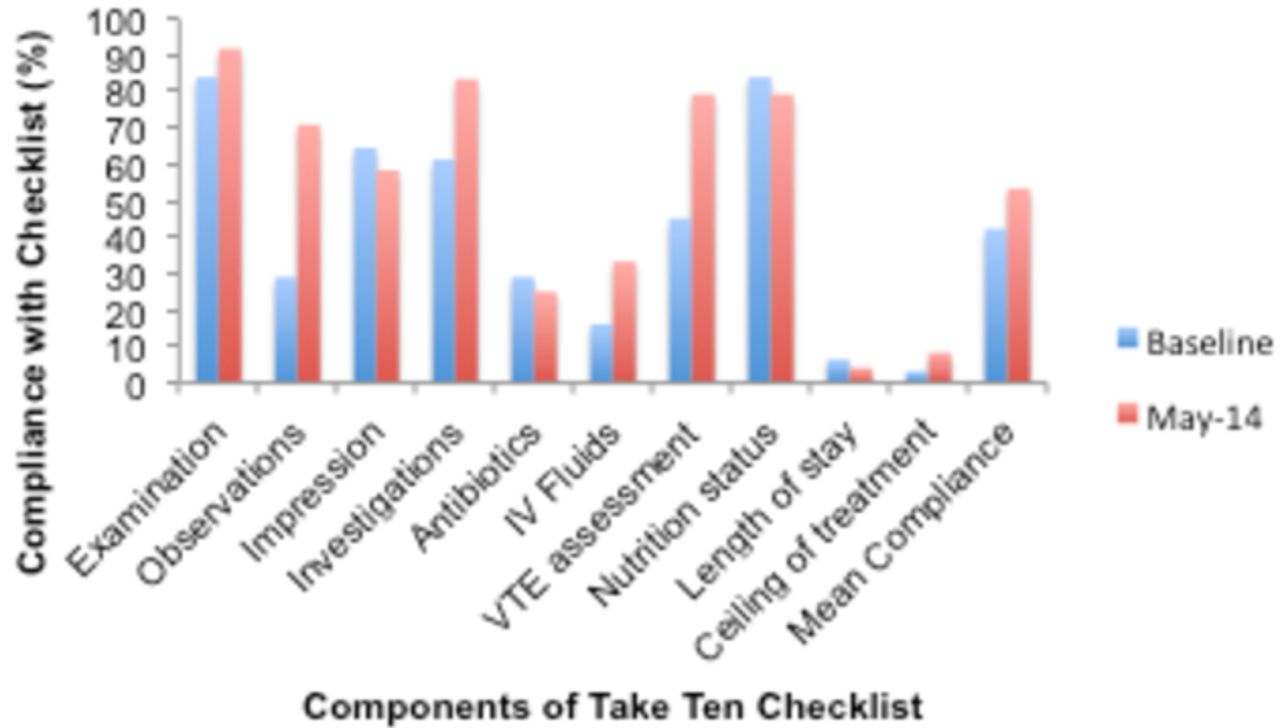
Retrospective data were collected at the start of the project. Selected clerking proformas for admitted surgical patients were reviewed, to assess whether each of the 10 points in the Take Ten checklist had been documented during the post-take ward round. After introduction of the checklist, the same process was repeated (figure 2).
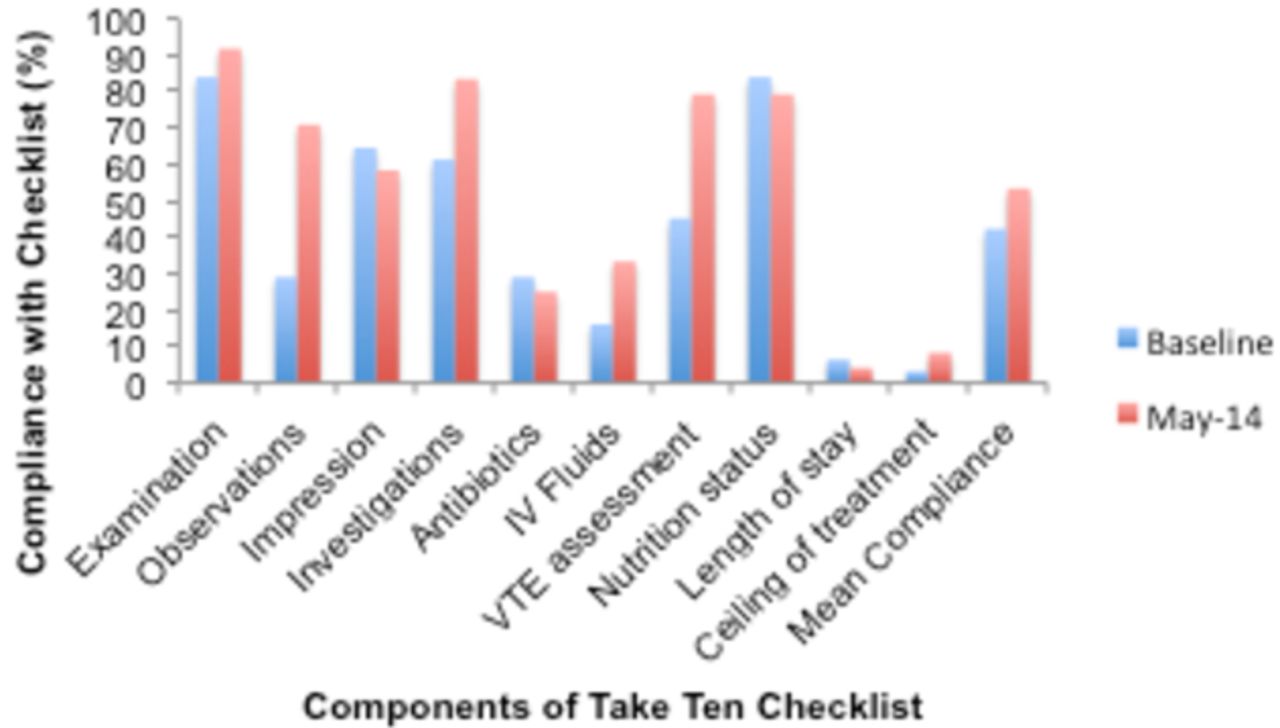
Graph comparing baseline data with data collected following PDSA cycle 1 (initial introduction of the checklist). PDSA, plan do study act; IV, intravenous.
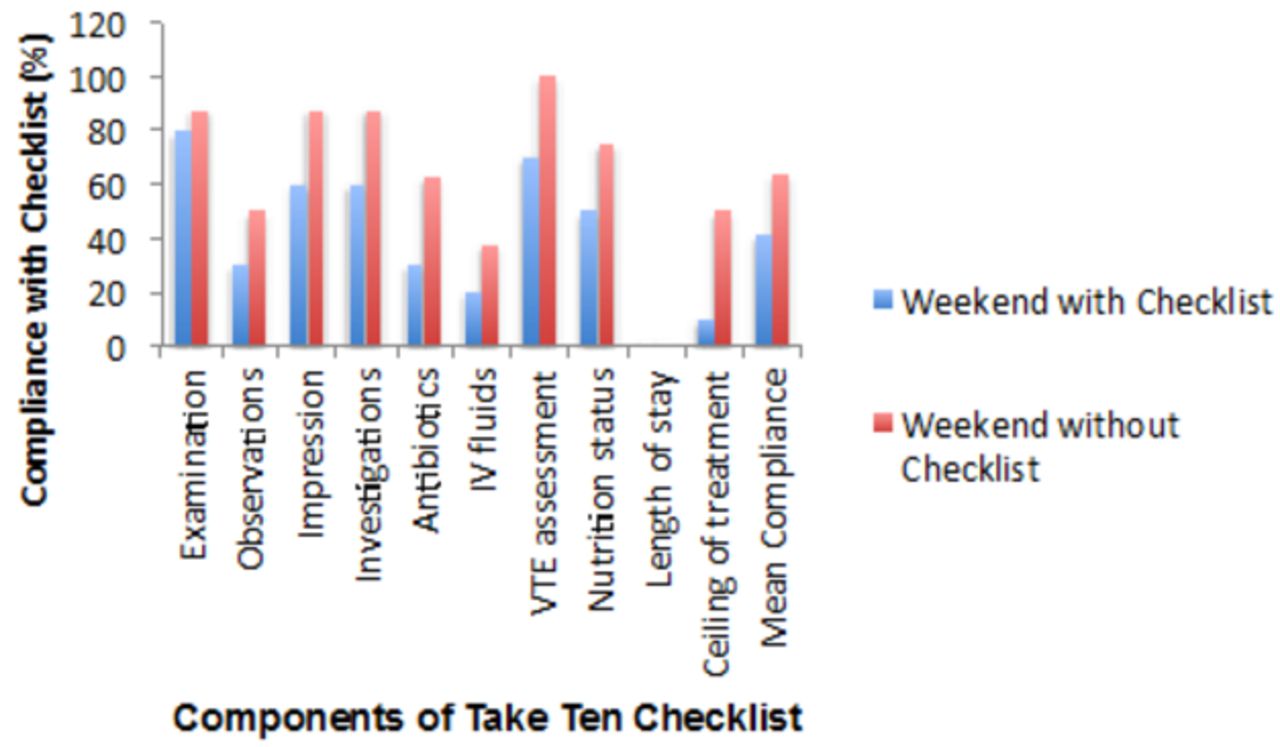
This initial comparison showed some improvement in documentation, but it was clear that not all consultants were using the checklist. Consequently, the postintervention data contained ward rounds both with and without checklist use. It was decided that a direct comparison in a more controlled manner (checklist vs no checklist) would be useful. This showed an improvement in documentation on the weekend the checklist was used, compared with the weekend it wasn’t (figure 3). The areas showing most improvement included documentation of impression (of diagnosis) and investigations needed, which both improved from 60% to 87.5%. Ceiling of treatment was documented in 50% of proformas when the checklist was used and only 10% when it was not. These data were used in our next presentation to consultants, to highlight effectiveness of the Take Ten checklist, and promote universal use.
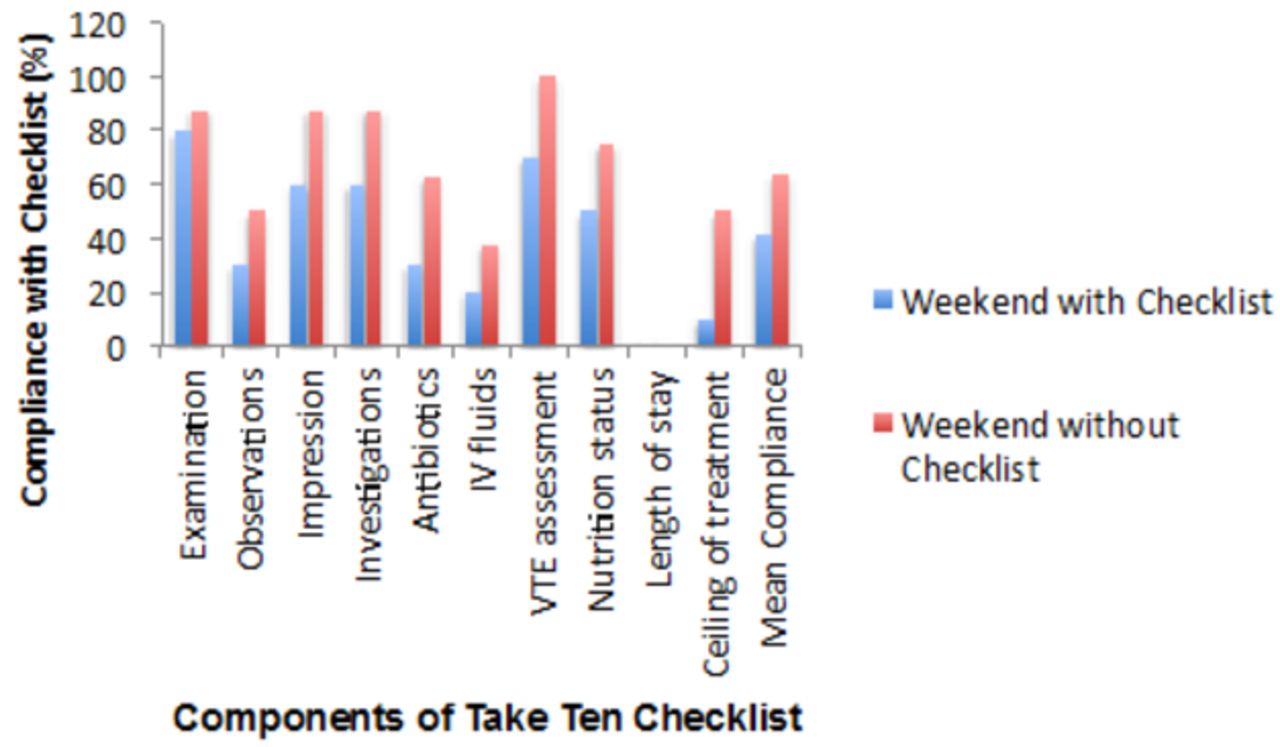
Graph comparing data from two weekends, one where the checklist was in use, and one where it was not. IV, intravenous.
Qualitative data collection involved circulation of an anonymous questionnaire asking FY1 doctors about their experience of using the checklist. This comprised six questions, exploring frequency of use, barriers to use of the checklist, and whether they felt Take Ten increased understanding of patient diagnosis and management. It was sent to all junior doctors on the acute surgical rotation via an online survey programme.
In the participating group, 80% of FY1 doctors (n=7) had a better understanding of the patient diagnosis and management plan and 100% felt the Take Ten could help facilitate a discussion about resuscitation status. However, 60% were not happy to initiate use of the checklist. Further investigation of this point found that the more junior team members found it difficult to instigate action in what they felt was a senior-led ward round, with some stating they felt the ward round could be an intimidating environment. They did however feel that the checklist itself empowered them to ask questions and clarify management plans when used. After a further presentation of the Take Ten results at the surgical directorate meeting, along with the weekend comparison data, the checklist was amended taking into consideration feedback from the consultants. Length of stay was replaced with drug chart review and the hospital logo was added to the checklist. The number of checklists available were increased and the checklist was moved from the SAU office where handover takes place, to the patient observation charts which are kept by the bedside. Further data were collected following this change.
Figure 4 shows a steady improvement in the mean compliance with the 10 points of the checklist following each PDSA cycle, and demonstrates the sustainability of the project, with good compliance almost 2 years on from PDSA cycle 3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chart showing project sustainability over 34 months with a steady increase in number of points correctly documented. PDSA, plan do study act.
An anonymous survey was repeated 3 years after inception of the project, this time including consultants, junior doctors and nursing staff using the checklist. Results showed that 100% of FY1 doctors (n=10), consultants (n=3), surgical registrars (n=4) and senior nurses (n=5) thought that the Take Ten checklist contributed positively to patient safety. Consultants also thought that the checklist improved patient flow through the hospital, as well as outcomes for patients and education for trainees. Comments included ‘should be used in all surgical wards, not just post-take ward round’, and ‘a simple and now essential tool for the ward round’. No consultants surveyed declared any conflicts of interest.
The repeat survey also showed that some FY1 doctors still hold reservations with initiating the checklist on a ward round, and stated that they believed senior nurses should be the team members responsible for this. Of the senior nurses questioned 100% felt comfortable initiating the checklist. These results reflect the way in which the checklist is currently used, with nursing staff most frequently initiating its use.
Lessons and limitations
The main challenge was encouraging individuals to take leadership of the checklist on a daily basis. Initially, it was thought that the FY1 doctors would be best placed to lead the checklist, as they are a constant feature in the ward round. They are also a group motivated to implement change, especially as proper use of the checklist would directly influence their working day. However, the questionnaire highlighted that FY1 doctors were reluctant to suggest use of the checklist. Senior nursing staff on SAU were approached, but had some concerns that their other commitments on the ward would prevent their facilitation of the checklist use. After discussion with the wider MDT, and as the checklist has become integrated into the daily ward round, we have found that the nursing staff are in fact the key drivers of checklist use, encouraging MDT involvement and removing ward round hierarchy. It is felt that this has been a real factor in the sustainability of the project. Thanks to the engagement and involvement of the wider multidisciplinary team, Take Ten has now become an integral part of the post-take surgical ward round despite all but one of the original project leaders moving on from the Royal United Hospital. Based on user feedback, there is hope to transfer a similar checklist to the surgical inpatient wards in the near future. Reflecting on the project, a lot has been learnt about the practical aspects of designing and implementing quality improvement projects. Given the problems encountered later in the project with stakeholder engagement, we could have taken longer in the early stages of the project to identify our key stakeholders. We would have then gathered opinion on how to improve the current system, giving those on the ward a feeling of responsibility and engagement with the project.
Limitations of the project include a small sample size. Data were limited by the number of patients admitted to SAU and reviewed on the surgical take on the days that data were collected. This was a particular issue as members of the team left for rotations in other hospitals, limiting the time available to them to collect data. As the project has evolved we have identified further issues with use of the checklist for outlying patients, and those seen outside of the surgical admissions unit. Identifying a more accessible form of the checklist may be one way of solving this issue, and is currently being assessed.
Conclusion
Implementation of the ‘Take Ten’ checklist resulted in improved documentation on the post-take ward round. Qualitative data from the FY1 doctor cohort were positive, most notably improving junior doctor understanding of patient diagnosis and management, and encouraging communication with senior team members. All users of the checklist feel it contributes to improving patient safety, and improves the post-take ward round experience.
When presented at various meetings, the issues highlighted in the project have resonated with many other doctors working within both surgical and medical settings. Accurate communication of the initial consultant review and their decision-making process is vital, as decisions made here can shape the rest of the inpatient stay. We feel Take Ten has made a real and sustainable impact in improving documentation on the surgical post-take ward round, and hope to roll out the concept to the wider hospital in the future.
Acknowledgments
The authors thank SKR for her ongoing support and guidance with this project, and the staff of the Surgical Assessment Unit for their invaluable feedback and enthusiasm for Take Ten.
Footnotes
Contributors DAB, CA, AT: conception of the project, data collection, interpretation and analysis, drafting of the initial paper, and final approval of the version to be published. DAB also revised the article following initial and subsequent peer review and was responsible for overseeing further data collection. JP, TF: data collection, interpretation and analysis; final approval of the version to be published. SKR: supervised data collection and project progression throughout, assisted with drafting of initial paper and final approval of the version to published.
Competing interests The Royal United Hospital Foundation NHS Trust is one of the centres which participated in the Emergency Laparotomy Pathway Quality Improvement Care (ELPQuiC) Study for improving patient mortality after emergency laparotomy. SKR was a co-author for the study and collected data for this study, in addition to the Take Ten project.
Provenance and peer review Not commissioned; externally peer reviewed.