Article Text

Abstract
Background and objectives: Provision of evidence-based hospital stroke care is limited worldwide. In Australia, about a fifth of public hospitals provide stroke care units (SCUs). In 2001, the New South Wales (NSW) state government funded a clinician-led, health system redesign programme that included inpatient stroke services. Our objective was to determine the effects of this initiative for improving: (i) access to SCUs and care quality and (ii) health outcomes.
Design, setting and participants: Preintervention–postintervention design (12 months prior and a minimum 6–12 months following SCU implementation). Retrospective, public hospital audit of 50 consecutive medical records per time period of stroke admissions (using International Classification of Diseases (ICD)-10 codes). Combined analyses for 15 hospitals presented.
Outcomes: Process of care indicators and patient independence (proportional odds modelling using modified Rankin scale).
Results: Pre-programme cases (n = 703) (mean (SD) age 74 (14) years; female: 51%) and post-programme cases (n = 884) (mean age 74 (14) years; female: 49%) were comparable. Significant post-programme improvements for most process indicators were found, such as more brain imaging within 24 hours. Post-programme, access to SCUs increased 22-fold (95% CI 16.8 to 28.3). Improvement in inpatient independence at post-programme discharge was significant compared with pre-programme outcomes (proportional odds ratio 0.73, 95% CI 0.57 to 0.94; p = 0.013) when adjusted for patient clustering and case mix.
Conclusions: This distinctive SCU initiative was shown as effective for improving clinical practice and significantly reducing disability following stroke.
Statistics from Altmetric.com
The burden of stroke is predicted to increase in both developed and developing countries.1 Stroke care units (SCUs), which provide geographically localised multidisciplinary management, are internationally recognised as the most generalisable and effective treatment for stroke.2 Although poorly documented, SCU availability in different countries seems to range between 4% and 70%.3 In Australia, about 19% of acute public hospitals have an SCU.4 Strategies for improving the establishment of SCUs have not been well described.
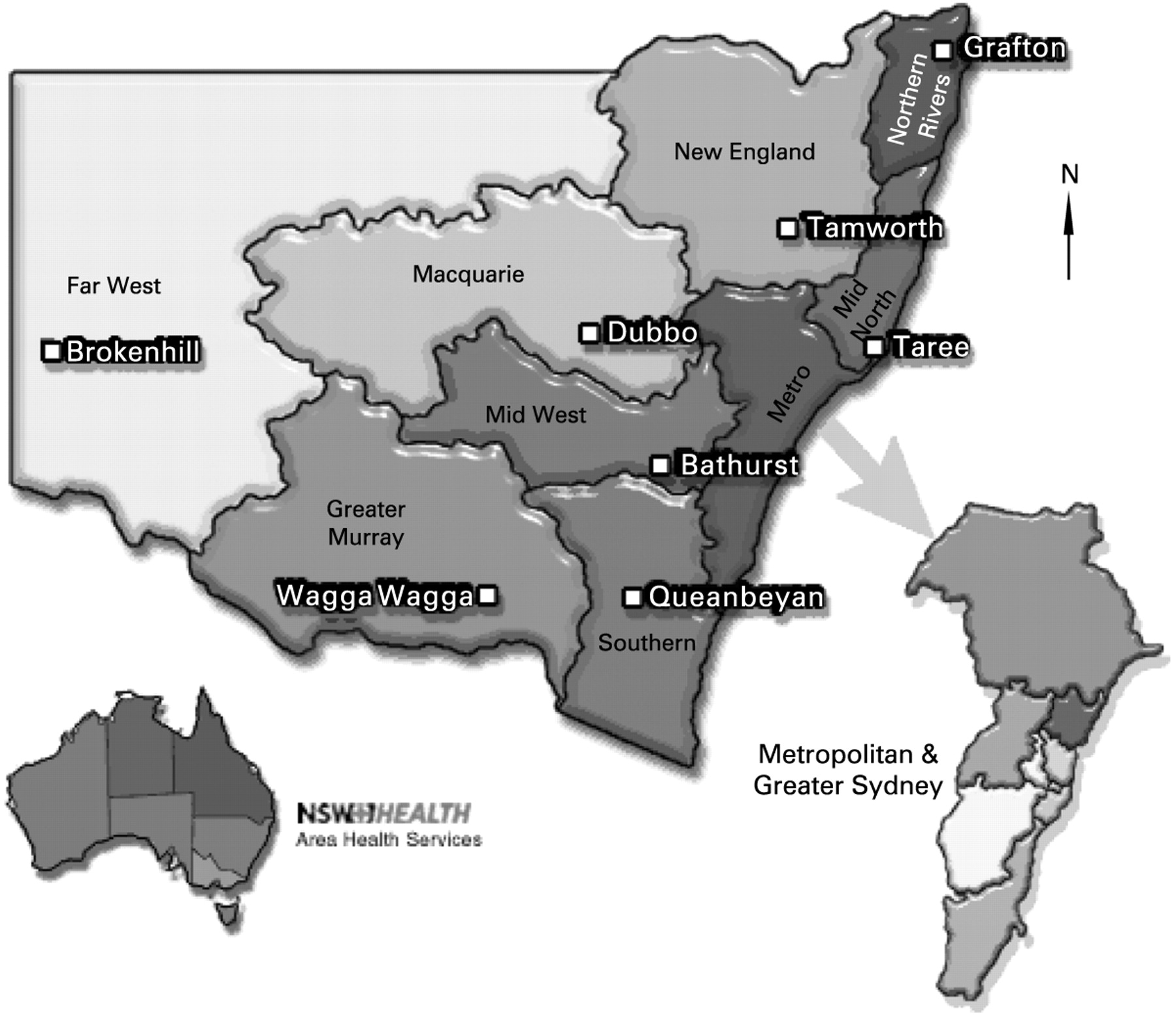
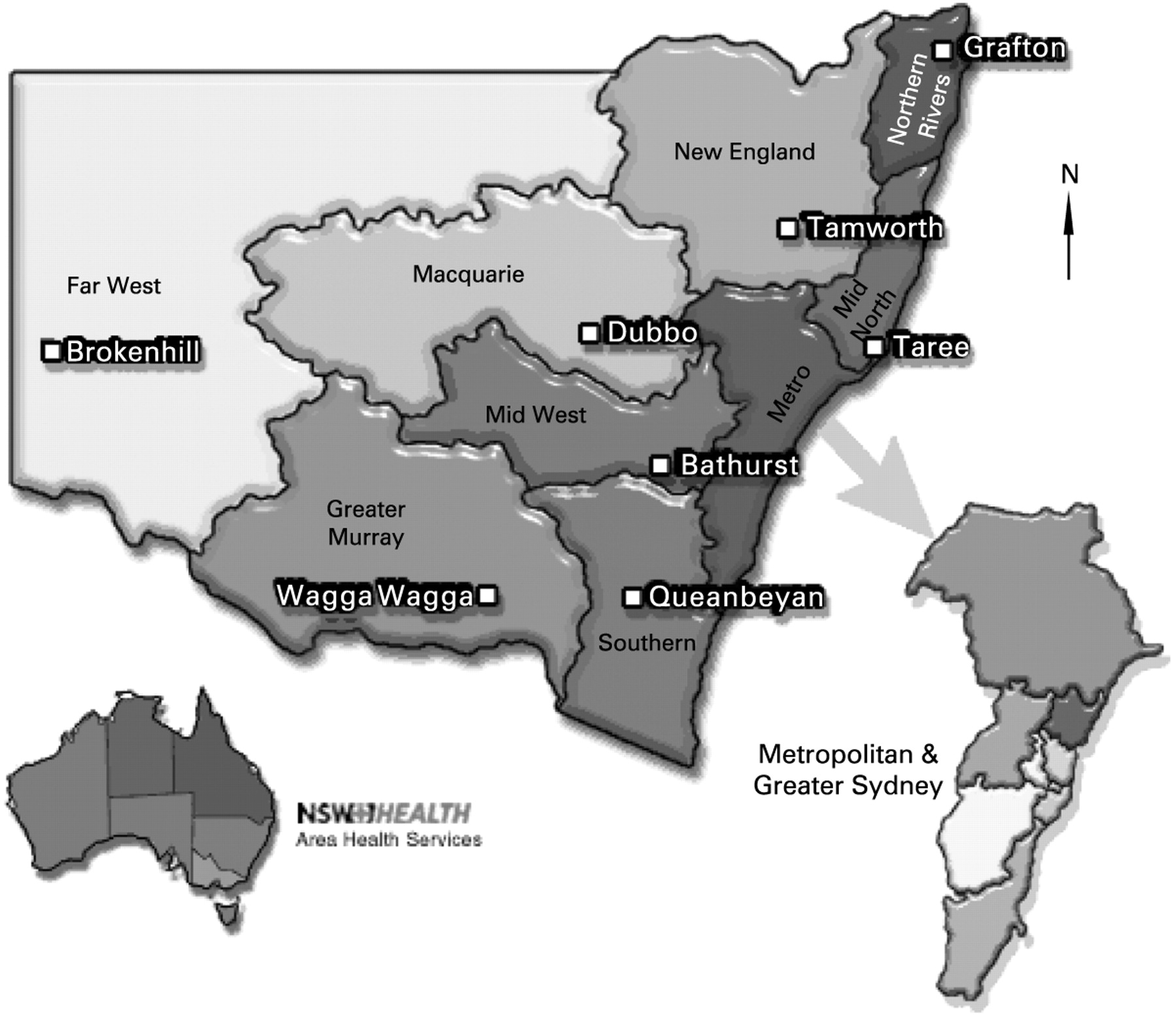
Although Australian national policy supports the establishment of SCUs,5 funding responsibilities are vested with separate state and territory governments. Therefore, low penetration of SCUs in this healthcare “system” suggested a significant policy–practice gap. In 2001, the New South Wales (NSW) government (responsible for about a third of the Australian population) enacted a health system redesign programme to improve access to evidence-based healthcare. It was the first to provide substantial funding for SCUs. The Greater Metropolitan Clinical Taskforce (GMCT) was subsequently established to bring clinicians and consumers together to work with the government to drive the programme objectives for the greater Sydney area67 (fig 1).
The original objectives of the stroke programme included establishing a coordinating committee and nine stroke area “networks” with 19 SCUs in hospitals admitting at least 200 strokes per year. In addition, minimum standards of care were to be developed and staffing and clinical training reviewed. Education forums and opportunities for networks to share information, such as clinical protocols, were also undertaken. Establishment funding, expended by June 2003, was mainly used for employing staff, purchasing equipment and/or ward refurbishments. Operational recurrent funding of approximately AU$10 million is ongoing. Prior to provision of establishment funding there were seven SCUs in the study region. In Australia, the length of stay for acute stroke care is typically between 10 and 11 days. Following the acute admission, patients are discharged home with or without additional outpatient rehabilitation services or they are discharged to an inpatient rehabilitation facility or to an aged care facility.
An external evaluation of the stroke programme was initiated with researchers from the National Stroke Research Institute (NSRI) (based outside NSW). The aims were to determine the effects of this programme for improving (i) access to SCUs and care quality and (ii) health outcomes by intention-to-treat, as well as for those receiving some or all of their care in an SCU.
METHODS
We used a preintervention–postintervention study design including consecutive audits of up to 50 medical records with a discharge International Classification of Diseases (ICD)-10 code for stroke for each time period. The pre-programme period was 12 months prior to the stroke programme commencing (mostly cases treated in 2001 and 2002). The post-programme period required cases to be admitted a minimum of 6–12 months following service enhancements (between 2003 and 2005). SCUs providing pre and post data by December 2006 which had received enhancement funding were included in this analysis (n = 15). Participation was voluntary and permission from the hospital administrators was obtained. Where required, approval by a human research and ethics committee was gained.
To maintain privacy, patient data were de-identified and only aggregated data are presented. Patient eligibility criteria were: diagnosis of stroke (ischaemic or haemorrhagic stroke); acute symptoms lasting more than 24 h; admission to hospital; and availability of the medical record for audit.
Data collection
An audit tool was developed that included clinical performance indicators advocated by the National Stroke Foundation (n = 9) and endorsed by the Australian Government,8 as well as high priority indicators previously reported by the NSRI.910 A range of measures were incorporated relevant to medical, nursing and allied health clinicians, such as brain imaging, allied health assessments, neurological observations, and reflecting timing of interventions, types of intervention and facilitators of better management (eg, use of clinical management plans).
For consistent data abstraction, participating hospital staff were trained by the GMCT stroke programme manager (previously trained by the NSRI). Completed audits were processed at the NSRI. Programmed data logic checks were implemented to verify the data (eg, date ranges and subcategory responses to primary questions). Inter-rater reliability was assessed by undertaking a 10% random audit of medical records in two of the hospitals, using a blinded and independent assessor.
Study end points
The primary end point reflects level of impairment following stroke and was based on the modified Rankin scale (mRS)11 score at discharge or 7–10 days after the stroke (range 0–6, 0 indicating no residual symptoms through sequential levels of disability to 6 indicating death). Secondary outcomes included adherence to individual process indicators as explanatory variables and proportion of severe complications.
Definitions
Process indicators
Admission to SCUs: percentage of patients admitted from the emergency department.
Access to SCUs: percentage of patients spending some time in an SCU.
Brain imaging: both CT and MRI.
Swallowing ability: documentation by any health professional.
Adherence rates: reflects care that should have been given (number of cases adhered/total applicable cases).
Clinical care plan: evidence of a written plan by health professionals.
Clinical pathway: structured tool detailing the activities of care during hospital admission.
Outcomes
Independence at discharge: mRS 0–22
Severe complications: any new medical condition occurring during hospitalisation and considered incapacitating, life-threatening or resulting in a prolonged stay or increased patient acuity.
Statistical analysis
Intention-to-treat and “on-treatment” (cases receiving some, or all of their care, in an SCU) analyses were undertaken for pre-programme–post-programme comparisons. Data were analysed using STATA version 8.0. χ2 tests were used for categorical variables, Fisher exact test for dichotomous variables, and the Mann–Whitney test for skewed continuous variables. Patient outcomes were investigated using ordered logistic regression to estimate the proportional odds ratio over all levels of the mRS (Stata Annotated Output: Ordered Logistic Regression; http://www.ats.ucla.edu/stat/stata/output/stata_ologit_output.htm; retrieved on 28 January 2007). Logistic regression was also used for dichotomous patient outcomes.
Adjustment for patient case mix was based on a validated prognostic model11 when comparing patient outcomes. These variables included independence prior to stroke (mRS 0 or 1), age, arm deficit, speech impairment, incontinence (within 72 h), and ability to walk unaided on admission. Adjustment was also made for patient clustering within hospitals.
Inter-rater reliability was assessed with the κ statistic. Agreement between observers was deemed to be excellent if κ>0.8, good if κ >0.6⩽0.8 and moderate if κ>0.4⩽0.6. The level of significance was p<0.05.
RESULTS
Fifteen hospitals contributed 1587 cases (pre-programme: 703 and post-programme: 884). Baseline demographic characteristics and stroke severity status were mostly comparable across the time periods (exceptions: history of hypertension and incontinence within 72 h). The mean (SD) age of the patients was 74 (14) and about half were men. When pre-programme cases were compared with post-programme patients treated in SCUs (mean age 78 (13) years, women 48%) the only significant difference was more pre-stroke independence in the post-programme SCU group (table 1).
Inter-rater reliability testing indicated key variables used for case mix adjustment, subgroup classification or as process indicators as generally demonstrating excellent or good agreement. Poor agreement was noted for ability to walk on admission, discharge delays, premorbid mRS and use of care plans.
Influence of programme on patient outcomes
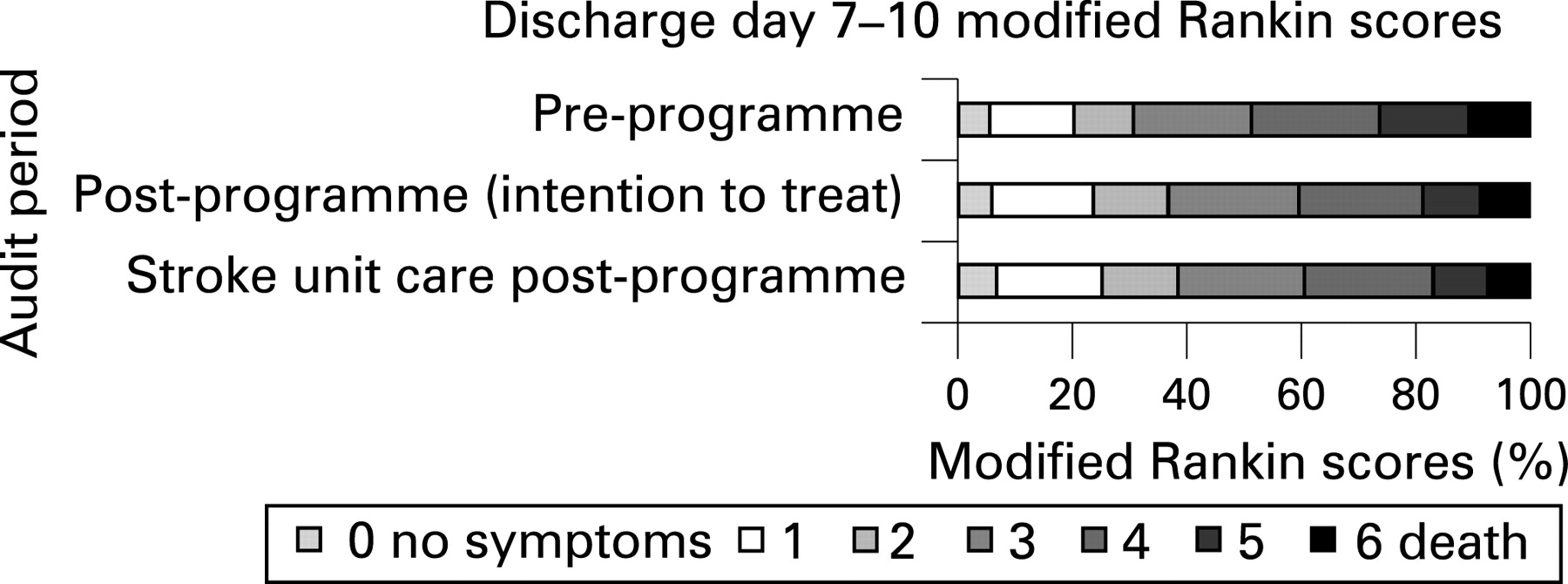
There was significant post-programme improvement across all levels of the mRS scores at discharge or 7–10 days after the stroke compared with patient outcomes pre-programme (table 2 and fig 2). Post-programme patients experienced fewer disabling outcomes (proportional odds ratio adjusted for case-mix and patient clustering OR 0.73; 95% CI 0.57 to 0.94). This result was further improved in post-programme patients receiving treatment in an SCU. When the mRS was dichotomised, the odds of being independent at discharge (mRS 0–2) improved post-programme (odds ratio (OR) 1.31, 95% CI 1.07 to 1.63) and was better if treated in SCUs (OR 1.39, 95% CI 1.12 to 1.74). However, adjustment for case mix and patient clustering eliminated the statistical significance (intention-to-treat OR 1.47, 95% CI 0.94 to 2.30; on-treatment OR 1.48, 95% CI 0.93 to 2.35). Treatment in an SCU also reduced the odds of severe complications (OR 0.55, 95% CI 0.37 to 0.82). However, the statistical significance was again lost with adjustments for patient case mix and clustering (OR 0.67, 95% CI 0.32 to 1.39).

{kind=link}
{kind=link}
Clinical management between audit periods
Prior to the programme, only 13% of cases were admitted to SCUs from the emergency department, whereas post-programme, 71% were directly admitted (OR 16.8, 95% CI 12.8 to 22.0). There was also a 22-fold increase for treatment in an SCU (admitted or transferred during admission) between the time periods (pre-programme 17% versus post-programme 81%, OR, 21.8; 95% CI 16.8 to 28.3). If treated in SCUs, most patients received at least 50% of their care in SCUs regardless of time period (pre-programme 86% and post-programme 89%).
Compared with pre-programme estimates, significant post-programme improvements were found for most process of care indicators. These improvements were consistently more pronounced if the patients were treated in SCUs (table 3). Post-programme patients were three times more likely to have brain imaging (OR 3.1, 95% CI 1.8 to 5.2) and twice as likely to have regular neurological observations (OR 2.35, 95% CI 1.6 to 3.4) within 24 h of admission. Post-programme cases received more allied health assessments (OR 2.4, 95% CI 1.5 to 3.6) and more family meetings within 7 days of admission (OR 3.7, 95% CI 1.1 to 12.3). If treated in an SCU with ischaemic stroke, the odds of receiving aspirin within 24 h as new treatment were 76% increased (OR 1.76, 95% CI 1.41 to 2.19) and a 38% greater chance of being discharged on anti-thrombotic therapy (OR 1.38, 95% CI 1.02 to 1.87).
Overall, approximately 3–5% of patients received palliative care and about 10% died in hospital. Median length of stay was about 9 days. More post-programme patients were discharged home and there was a reduction in inpatient admissions for rehabilitation (table 4).
DISCUSSION
Important changes in clinical practice and patient outcomes were identified following investment in stroke services in the Greater Metropolitan Area of NSW. In particular, the study provided evidence that better access to important aspects of organised stroke care such as timely and early allied health assessments, brain imaging and appropriate use of aspirin, which are consistent with current clinical practice guideline recommendations.12 These improvements were supported by increased use of care planning and admissions to localised SCUs. The increased access to SCUs with better adherence to important clinical processes of care resulted in about a third of patients following stroke having improved outcomes compared with pre-programme estimates. These findings are consistent with other similar observational studies.13–16
The proportional odds modelling using the mRS was chosen as the more precise method of analysing the outcome data between programme time periods rather than using a dichotomous cutpoint.1718 Indeed, the importance of the stroke programme and subsequent better effectiveness of SCUs was evidenced more clearly, in a demonstrated shift away from higher scores (worse outcomes) towards lower scores (greater independence) (see online supplementary data for web-only table and fig for estimated “modelled” prediction scores). The power to detect differences in the occurrences of severe complications was compromised by a low event-to-variable ratio.
As this was a pragmatic audit, hospital-based clinicians collected the data. Nonetheless, the data collected were shown to be reproducible by an independent and blinded auditor. This has also been demonstrated in another similar study.19 Other potential sources of reporting bias include abstracting process of care data from medical records, which may not have been routinely recorded or required subjective judgements. Steps to minimise bias included using external investigators to analyse the data, supplying a data dictionary and consistent auditor training. Other limitations include the possibly better recording of process data and outcomes given improved use of clinical management plans. In addition, changes in clinical practice may have occurred over time irrespective of the programme. These factors may be overestimating the effects of the programme, but as the effects are mostly large, this cannot explain all the differences. Furthermore, the sampling strategy was non-random and this may have led to biased estimates of effects and differences between comparator groups. However, the approach of using consecutive admissions is consistent with other similar research in this field.16
We acknowledge that in the univariate analyses presented for demography, risk factors and indicators of stroke severity (table 1), a spurious statistically significant finding was probably because of the conduct of multiple comparisons. The observed differences while significant at the 0.05 level were small enough to justify the assumption of comparability of the two cohorts. Further, we have made adjustment for differences in case mix in multivariate analyses. The coherence between the magnitude of the impacts of the intervention were consistent across processes of care and patient outcomes, providing confirmatory evidence that these findings are valid.
CONCLUSION
We have been able to highlight improvements in the quality of care as a consequence of the NSW GMCT stroke programme being implemented. The success of the GMCT stroke unit programme has resulted from, among other things, effective implementation of a governmental health policy by the development of a strong partnership between stroke clinicians and health service management. An important initial incentive to form this partnership was resource allocation to establish or enhance SCUs. Better patient outcomes were clearly observed associated with greater adherence to evidence-based practice. Individual hospital stroke services also possibly benefited from the audits by using their individual results to focus additional improvements in stroke care at their centres. Audit and feedback cycles can be effective at changing clinical practice.20 With continuing demonstration of the effectiveness of such programmes, hopefully more Australian states, and other countries where access to SCUs is not universal, will invest in initiatives to forge partnerships between stroke clinicians and health service management resulting in improved access to SCUs.
Acknowledgments
The involvement of the hospital staff, and the assistance and cooperation of the Stroke Program State Manager, Mark Longworth, and the Area Stroke Clinical Nurse Consultants is acknowledged. We also acknowledge the area directors of Stroke Services across the GMCT network for supporting this work: C Storey, D Crimmins, J Sturm, M Pollack, A Zagami, D Serisier, A Corbett, A McDougall, J Wood and P Landau. The authors thank S Morrisey, B Quang, N Chivatas and A Young for their contribution to data processing. We also thank L C Quang for her contribution to teleform questionnaire development and database management. J Stork is acknowledged for her contribution as the blinded independent auditor.
REFERENCES
Supplementary materials
web only appendix 17/5/329
Files in this Data Supplement:
Footnotes
Funding: The GMCT evaluation was supported by New South Wales Health, which was facilitated by the Greater Metropolitan Clinical Taskforce and the New South Wales Stroke Services Network Coordinating Committee.
Competing interests: CL is the head of one of the dedicated stroke units involved in this study. However, he was not directly involved in the collection of data or analysis of the results.
Linked Articles
- Quality lines