Article Text

Abstract
Background Computerised provider order entry (CPOE) is rapidly becoming the mainstay in clinical care and has the potential to improve provider efficiency and accuracy. However, this hinges on careful planning and implementation. Poorly planned CPOE order sets can lead to undetected errors and waste. In our emergency department (ED), lactate dehydrogenase (LDH) was bundled into various blood work panels but had little clinical value.
Objectives This quality improvement initiative aimed to reduce unnecessary LDH testing in the ED.
Methods A group of ED physicians reviewed CPOE blood work panels and uncoupled LDH in conditions where it was deemed not to provide any clinically useful information. We measured the daily number of LDH tests performed before and after its removal. We tracked the frequency of other serum tests as controls. We also analysed the number of add-on LDH (ie, to add LDH to samples already sent to the lab) as a balancing measure, since this can disrupt work flow and delay care.
Results Through this intervention, we reduced the number of LDH tests performed by 69%, from an average of 75.1 tests per day to 23.2 (P<0.0005). The baseline controls did not differ after the intervention (eg, a complete blood count was performed 197.7 and 196.1 times per day preintervention and postintervention, respectively (P=0.7663)). There was less than one add-on LDH per day on average.
Conclusions CPOE care templates can be powerful in shaping behaviours and reducing variability. However, close oversight of these panels is necessary to prevent errors and waste.
- decision support, computerised
- emergency department
- information technology
- quality improvement
- decision making
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- decision support, computerised
- emergency department
- information technology
- quality improvement
- decision making
Introduction
Lactate dehydrogenase (LDH) is an enzyme that is found in nearly all tissues1 2 and can be elevated from many diseases (eg, myocardial infarction,3 tumour lysis syndrome,4 haemolysis5 and Pneumocysitis carinii pneumonia6). LDH is included in several computerised provider order entry (CPOE) laboratory panels in our emergency departments (EDs). However, as described by Jialal and Sokoll,7 its traditional usefulness as a screening test has been largely supplanted by more sensitive and specific biomarkers such as troponin, liver enzymes and other diagnostic techniques.
CPOE systems can aid in the provision of standardised, evidence-based care.8 Standardisation is particularly helpful in the fast-paced, high-stakes, hectic environment of the ED.8 9 CPOE has the advantage of facilitating forcing functions (FFs). FFs are processes built into a workflow that necessitate a certain action or outcome before subsequent actions can be performed.10 CPOE FFs have been shown to significantly influence test ordering in the ED.10 11 We embarked on a quality improvement initiative aimed to reduce unnecessary LDH testing in the ED by modifying CPOE laboratory panels.
Methods
This was a prospective, multisite quality improvement project carried out at two academic tertiary care EDs with a combined 112 000 annual visits. Both EDs belong to a larger institution and use the same CPOE system (EPR, QuadraMed Corporation, Herndon, Virginia, USA).
CPOE blood panels were reviewed by the lead author and a clinical biochemist and identified panels containing LDH. Panels are grouped by presenting complaint or syndrome, which included ‘abdominal pain’, ‘toxicology’ and ‘trauma’. The proposed removal of LDH from these panels was discussed by the entire ED physician group via an online survey and discussion. There was unanimous agreement among this group in favour of removing LDH from these CPOE panels.
The primary outcome was the ordering rate of LDH, with rates of complete blood count and creatinine as controls. We collected data between 30 April and 20 July 2017. The changes to the CPOE system were introduced on 22 June 2017. Preintervention and postintervention groups were compared with Student’s t-test. We also measured the rates of LDH add-ons to the lab (ie, when a provider adds an extra test to blood samples already received in the lab that was not ordered at the time of sending) as a surrogate to potential disruption to provider workflow and delays to patient care.
Results
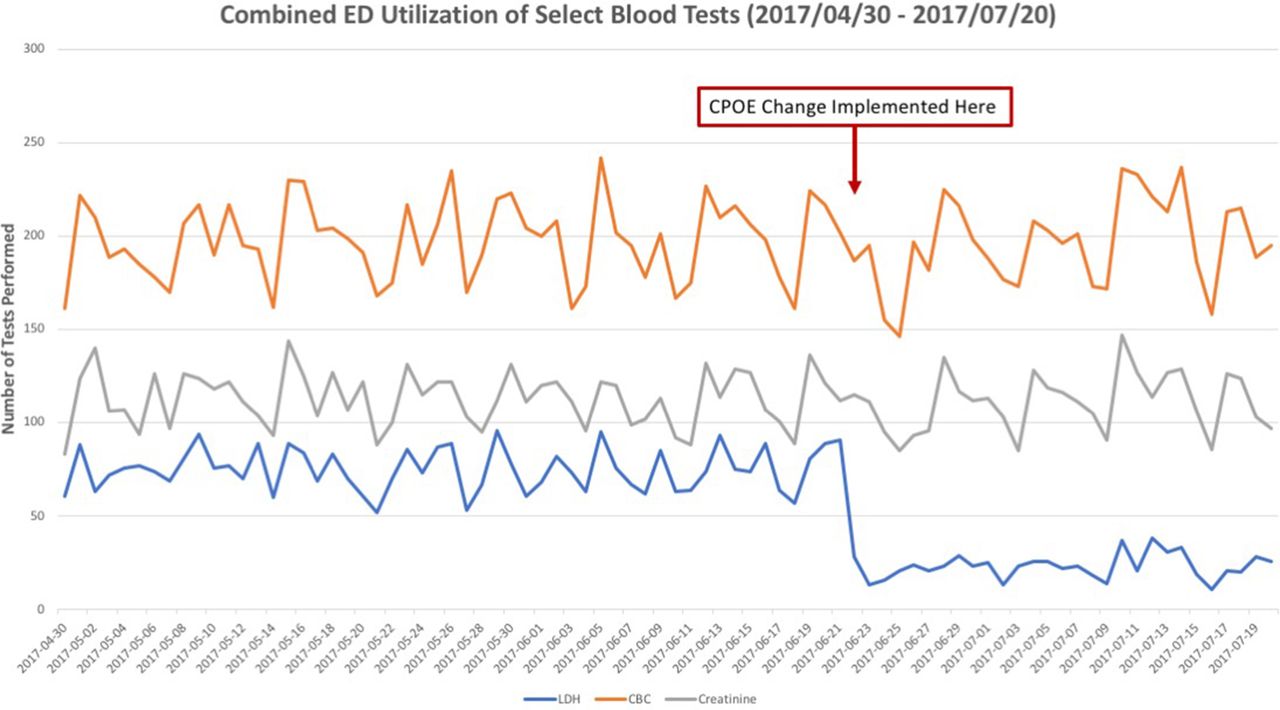
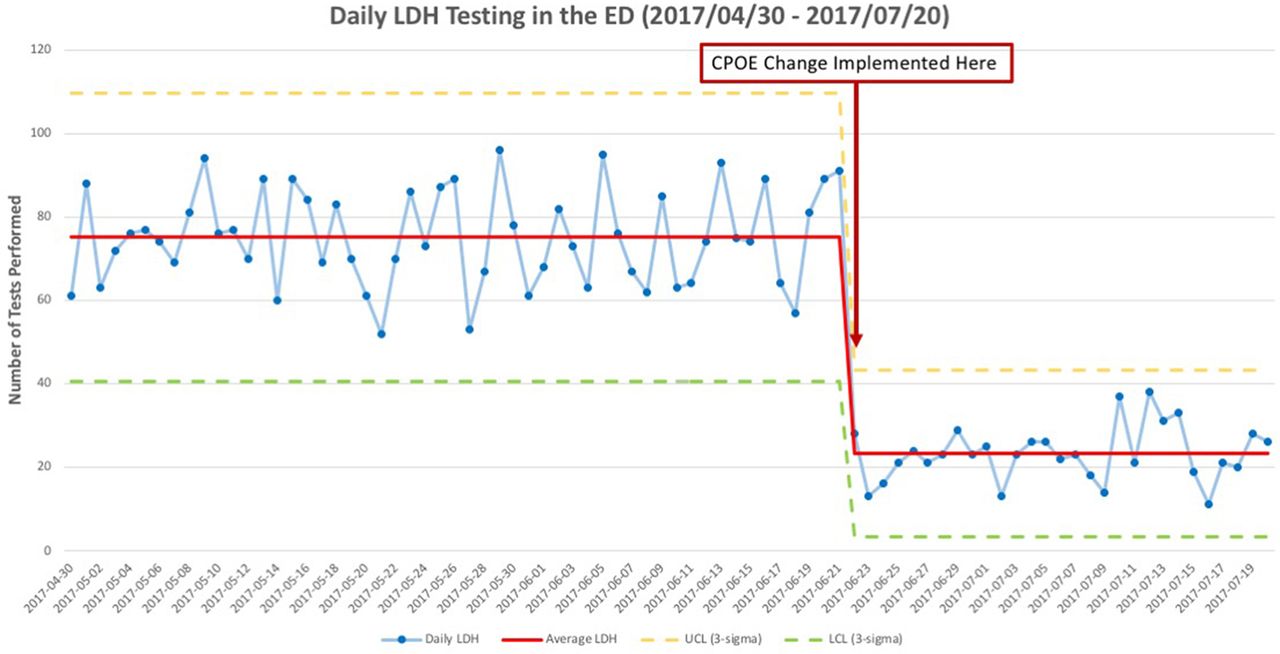
The daily rates of ordering for the selected tests across both EDs are shown in figure 1 and table 1. The rate of LDH ordering was 75.1 tests per day prior to the intervention and dropped to 23.2 tests per day afterwards (69.1% relative reduction, P<0.00005). The rates for the controls did not change (table 1). Using run charts, it is shown that the intervention reduced the rate by more than 3 SD away from the preintervention mean, signifying special cause variation that was sustained (figure 2). In our analysis of add-on rates, there was an average of fewer than one instance per day. At our institution, it costs $1.76 Canadian dollars per LDH test run, translating to savings of $33 340.56 annually.
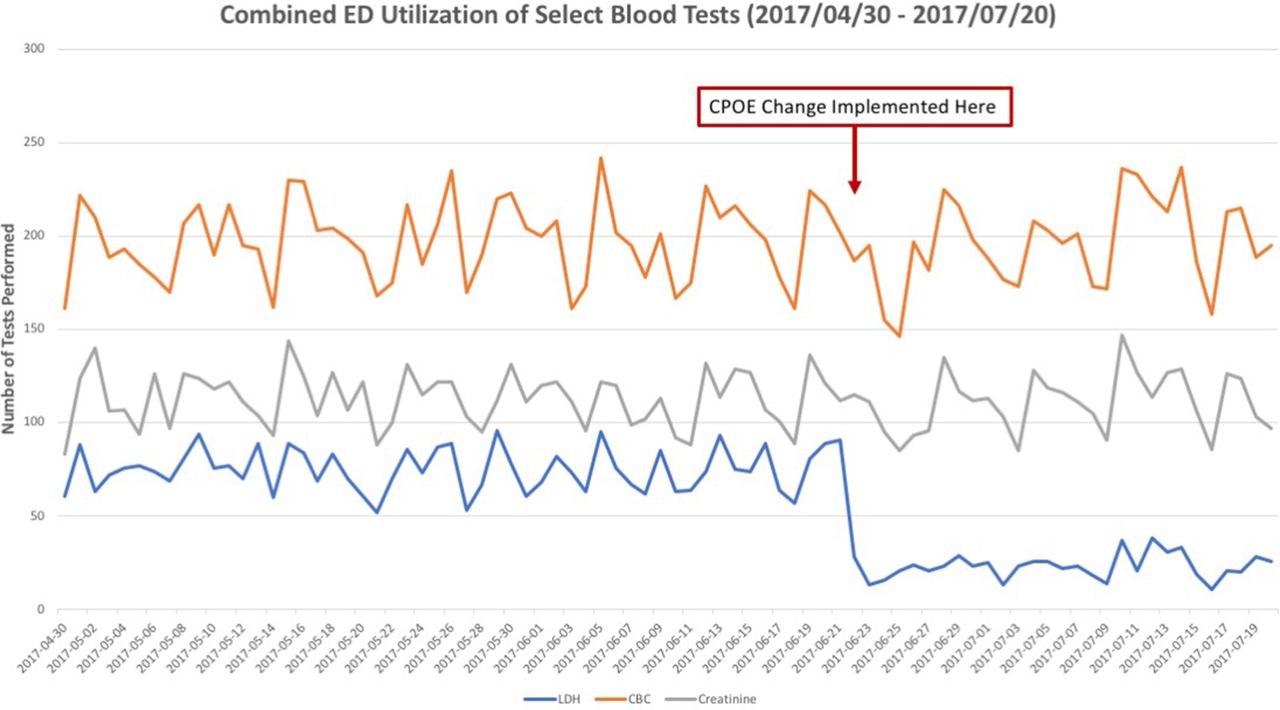
Combined daily ED utilisation of select blood tests. CPOE, computerised provider order entry; ED, emergency department.

{kind=link}
{kind=link}
Combined daily ED utilisation of serum LDH testing. CPOE, computerised provider order entry; ED, emergency department; LDH, lactate dehydrogenase.
Combined average daily ordering rates for selected tests across both ED sites
Discussion
This project highlights the double-edged sword of CPOE. While CPOE order sets reduce practice variation and improve adherence to guidelines, they can also have unintended negative consequences.12 13 For example, CPOE order sets may contribute to perceived loss of physician autonomy,9 increased patient length of stay9 and workflow disruption.14 Design and upkeep of CPOE systems require vigilance, given that design flaws can have far-reaching implications, including potential adverse events.15 16 Including LDH as a default order prompted wasteful, non-evidence-based test ordering practices. By eliminating LDH from standard panels, it required providers to actively choose to order LDH and subsequently produced a dramatic 69.1% reduction in testing. Physicians were surveyed postintervention, and they did not even notice its absence in the lab panels. Through this, we were able to eliminate waste, improve testing stewardship and cut costs with no apparent adverse effects.
There was no change in the rates of the control groups, suggesting that the change is not attributable to other background effects or overall changes in provider behaviour.
Limitations
The limited scope of this project did not allow for a full assessment of unintended consequences, namely ED length of stay. We captured that there was less than one LDH test added on to bloodwork already sent to the lab daily, which we expect will not contribute substantially to ED length of stay or workflow disruption. Considering the immediate success of this intervention, there were no additional plan-do-study-act cycles performed in this project.
Acknowledgments
We would like to acknowledge Dr Paul M Yip from the University Health Network for his help in coordinating and implementing the project, as well as gathering the data.
References
Footnotes
Contributors JC conceived and planned the project, conducted the physician group survey, implemented the interventions, collected the data, analysed the data, drafted and edited the report and submitted the report. CRA conceived and planned the project and helped draft and edit the report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Paul M Yip.