Article Text

Abstract
Introduction In April 2010, the government introduced a new Statement of Fitness to Work or ’Fit Note' for patients requiring time off of work or adaptations to their work due to illness. Responsibility to issue these documents has shifted from primary to secondary care. Hospital clinicians are required to issue for inpatients and for outpatients where clinical responsibility has not been taken over by the general practitioner (GP). However, awareness of this change is lacking. Misdirecting patients to their GP for the sole purpose of receiving a ’Fit Note' is an unnecessary use of appointment time and negatively impacts on patients. King’s College Hospital NHS Trust receives a number of quality alerts from primary care regarding this issue.
Methods A trust-wide educational initiative was designed and implemented to increase staff awareness of Fit Notes and their correct usage in order to reduce the number of patients being misdirected to their GP to obtain one. Interventions included direct staff engagement, a trust-wide promotional campaign and creation of an electronic version of the document.
Results Uptake of the electronic version of the Fit Note has steadily increased and there has been a fall in the number of quality alerts received by the trust. However, staff awareness on the whole remains low.
Conclusions Patients being misdirected to their general practice for Fit Notes is an important issue and one on which the baseline level of awareness among hospital clinicians is low. Challenges during this intervention have been in penetrating a trust of this size and getting the message across to staff. However, digitising the Fit Note can help to increase its use.
- quality improvement
- primary care
- patient-centred care
- medical education
- hospital medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Problem
Incorrectly directing hospital patients to their general practitioner (GP) when they require a Statement of Fitness to Work or ‘Fit Note’ delays the patient providing their employer with the required medical evidence of their health condition. If a GP appointment is for the sole aim of obtaining a Fit Note, this is a waste of an appointment for both the patient and the GP. Furthermore, the relevant discharge paperwork may not have reached the GP, resulting in further delays. Given the current strain on GP appointments, reducing wastage and duplication of work wherever possible is a priority.
Background
In April 2010, the government introduced ‘Fit Note/Statement of Fitness to Work’1 in response to Dame Carol Black’s report, ’Working for a Healthier Tomorrow'.2 This report concluded that illness is not just compatible with but improved by returning to work. Healthcare professionals need to adapt advice given to patients in order to reinforce this message.2 3 Fit Notes replace the old Med 3 Sick Note. Doctors indicate that either the patient is ‘not fit for work’ or that they ‘may be fit for work’ taking into account modifications to their hours or duties, for instance.4 Responsibility for issuing a Fit Note lies with the doctor who has clinical responsibility for the patient. For hospital-based doctors, this would be:
Following treatment in Accident and Emergency.
Following discharge after inpatient stay.
Following discharge after elective day surgery.
In outpatient clinic where the doctor has ongoing clinical care such as ophthalmology clinic or fracture clinic.
Guidance exists online on how to issue a Fit Note5 as well as guidance from Royal Colleges on suggested recovery times.6 7 Much of the recent Fit Note literature focuses on their use in primary care and their impact on long-term sickness. Little work has focused on Fit Note usage in secondary care. Historically, it has been suggested that hospital clinicians lack knowledge on this subject8 and we found this to be the experience in our trust.
King’s College Hospital NHS Foundation Trust is split over five geographically distinct sites in South East London. It is one of London’s largest and busiest teaching hospitals employing around 11 600 staff.9 In addition to providing services to six local boroughs, it provides tertiary and quaternary services. On average, 71 000 patients of working age are admitted yearly, and there are 2 21 000 unique outpatient contacts.10
When eligible patients are discharged without a Fit Note or have been told, incorrectly, to see their GP for one, ’Quality Alerts' are raised by the GP to notify the trust of the incident. An increasing number of alerts were being raised by GPs in areas served by our trust. The issue was flagged at primary care liaison meetings, where trust and primary care representatives meet regularly, and subsequently escalated to hospital management. Following this, the postgraduate medical and dental education department (PGMDE) was asked to design an initiative to address this issue.
Aims
The goals of this project were to design and implement an educational initiative across all sites of the trust from December 2016 to July 2017, with the aims of increasing staff awareness and correct provision of Fit Notes. This should reduce the inappropriate usage of GP appointments for Fit Notes related to hospital procedures or diagnoses.
Methods
Interventions and team
Our project used the Model for Improvement by Langley et al 11; improvement arises from action using a stepwise Plan–Do–Study–Act cycle (PDSA). A team was formed of postgraduate education fellows, led by the director of medical education, and the primary care liaison office in addition to expertise from the clinical systems team.
A multipronged approach was agreed with a trust-wide publicity campaign alongside targeted promotion to the junior doctors.
Prior to the project, Fit Notes were issued as paper A5 documents, stamped to prevent abuse. The team felt that an electronic version that could be accessed via the electronic notes system, Electronic Patient Records (EPR), used at King’s College Hospital would make it quicker and easier for staff to use and this may therefore help to increase usage by staff.
Measures
A number of outcomes were measured during the project. First, the number of quality alerts received by the primary care liaison team relating to non-issuing of Fit Notes. Second, staff awareness of Fit Notes and their correct usage. It was anticipated that in the initial phase, the number of quality alerts would rise. Increased awareness of the hospital clinician’s responsibility to issue Fit Notes and the trust-wide improvement programme were thought to be potential drivers behind this. Success would be defined as a fall in the number of quality alerts received (following an initial rise) and increased staff awareness of Fit Notes. This was to be assessed via a staff survey.
Ethical considerations
Ethical approval was not necessary as this was a quality improvement project with no potential harm to patients. Staff surveys were anonymous.
Study design
Funding was not required as existing staff and resources were used on the project. The project ran from December 2016 until July 2017 and data were collected throughout. Achievements of the initiative were analysed midpoint through the intervention period.
PDSA 1: A team from PGMDE collaborated with the Clinical Systems Development Team to develop an electronic copy of Fit Note. This is an exact replica of the paper version with the added traceability to a specified user provided by EPR. This also allowed us to keep track of Fit Note usage for audit purposes. The electronic version was introduced into mandatory EPR training for all new staff during induction. EPR use is not however currently trust-wide. Staff at sites not using EPR continue to use the A5 paper copies.
A page on the hospital intranet was created to inform staff of the Fit Note policy, the electronic ordering and a step-by-step guide on how to do this. The page directed staff to the government webpage for further guidance if needed. The initiative was publicised trust-wide in a number of ways. The weekly electronic hospital newsletter and posters displayed in prominent areas such as the doctor’s mess and ward staff notice boards were used to publicise Fit Note policy. Each clinical division was asked to nominate a lead to produce departmental guidance to distribute and help spread awareness. Weekly junior doctor teaching sessions were targeted at regular intervals to increase awareness and troubleshoot any on the ground problems.
Quality alerts raised by primary care were received by our primary care liaison team. They were cascaded to the relevant clinical services by the liaison team along with information on Fit Notes, a link to the intranet page and the name of a member of the postgraduate educational team in order for departmental training to be arranged. GPs were kept updated with the Trust’s project via the monthly primary care liaison newsletter as well as being informed of the action point from any alerts raised.
PDSA 2: It was decided that the interventions needed to be more targeted and focused on individual departments at a time. It was also felt that there needed to be greater buy in from senior clinicians. Although leads had been asked to create their own local guidance to distribute, it was felt that they may need support in this. Clinical leads for each department were contacted by the medical education fellows to arrange for the fellows to visit the department and deliver an update on the topic. This took the form of a short PowerPoint presentation usually delivered at clinical governance meetings. Single page written guidance (see online supplementary appendix 1) devised by the education fellows was also sent to service managers and educational leads to be distributed to staff, particularly new starters following induction.
Supplementary file 1
The quality alert reports were copied to a named medical education fellow working within the PGMDE. They made direct contact with the medical and nursing teams involved in the incident, to seek their views and gauge awareness of Fit Notes. Ward or departmental training was also offered during these conversations. This led to a greater number of departments who had been in receipt of a quality alert agreeing to and receiving teaching for their staff.
Liaising with the ward managers allowed the views of the nursing staff to be sought, with nursing colleagues encouraged to challenge doctors at point of discharge or during discharge planning if a patient was being incorrectly diverted to their GP for a Fit Note. The nursing discharge checklist will be amended at its next review date to incorporate a Fit Note check box. This will allow staff to prompt the discharging team if needed. Ward clerks were informed of the move to electronic issuing of Fit Notes to facilitate the correct signposting of staff who need to provide one for their patient.
Results
Staff awareness
In our initial staff survey, 22 staff responded: 12 consultants, 7 specialty registrars, 1 speciality trainee 1-2 or equivalent, 1 associate specialist and 1 clinical lecturer. Of those 22 respondents, 64% stated that they were aware of Fit Note but only 59% correctly identified whose responsibility it was to issue them. Of those staff whom were aware, 24% of respondents had become aware from our staff campaigns. No respondents stated that they had received any formal training at an undergraduate or postgraduate level on the issuing of Fit Notes. Despite the trust-wide campaign regarding the online availability of Fit Note within the electronic ordering system, 95% of the staff who responded were not aware of this change, which was disappointing for the team. This highlights the difficulties of penetrating a trust of this size. As well as lack of existing baseline Fit Note awareness, voluntary uptake of departmental training offered via email following quality alerts was low.
In the second cycle, a follow-up survey sent after the intervention period was completed by 18 doctors: 12 consultants, 1 associate specialist and 5 junior doctors, across a range of specialties and trust sites. Of those 18 respondents, 77% were aware of Fit Note as a concept with 66% correctly identifying whose responsibility it was to issue. Awareness of Fit Note policy as a result of our campaign was 39%. Only three doctors stated that they had had training in Fit Note completion and only one of these was from their undergraduate training. This leaves 82% of respondents, of grades ranging from foundation through to consultant, who should be issuing Fit Notes, who have received no training on the subject. This is similar to the figure in the initial survey of 100%. This emphasised to the team the size of the task in trying to implement an educational intervention on a mass scale.
Electronic issuance and quality alerts
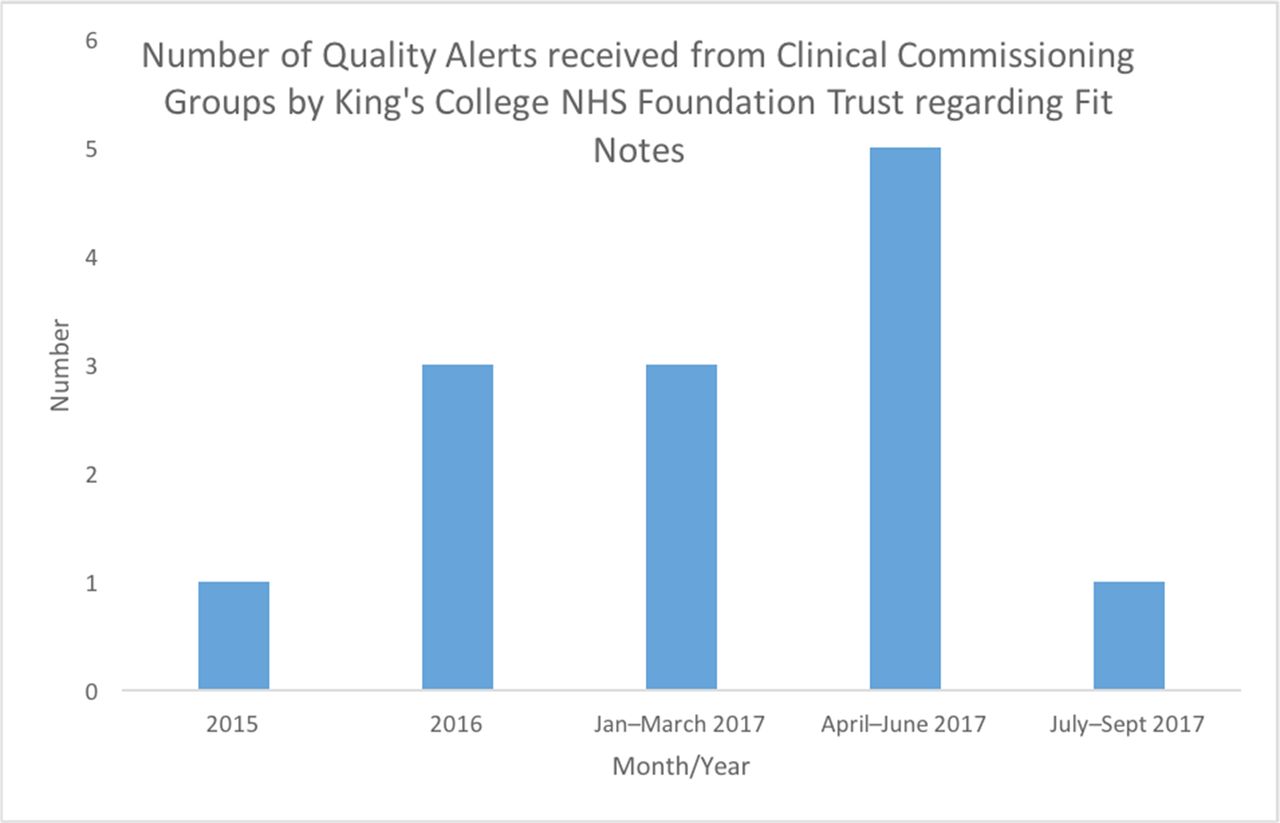
Encouragingly, there has been an increase in electronic issuing of Fit Notes (figure 1) with senior medical staff issuing them as well as more junior members of the team (figure 2). This is important as in some instances, such as elective surgery and outpatient clinics, the patient may see only the consultant. The number of quality alerts received by the trust has also fallen (figure 3) following the expected increase in number at the start of the educational initiative.
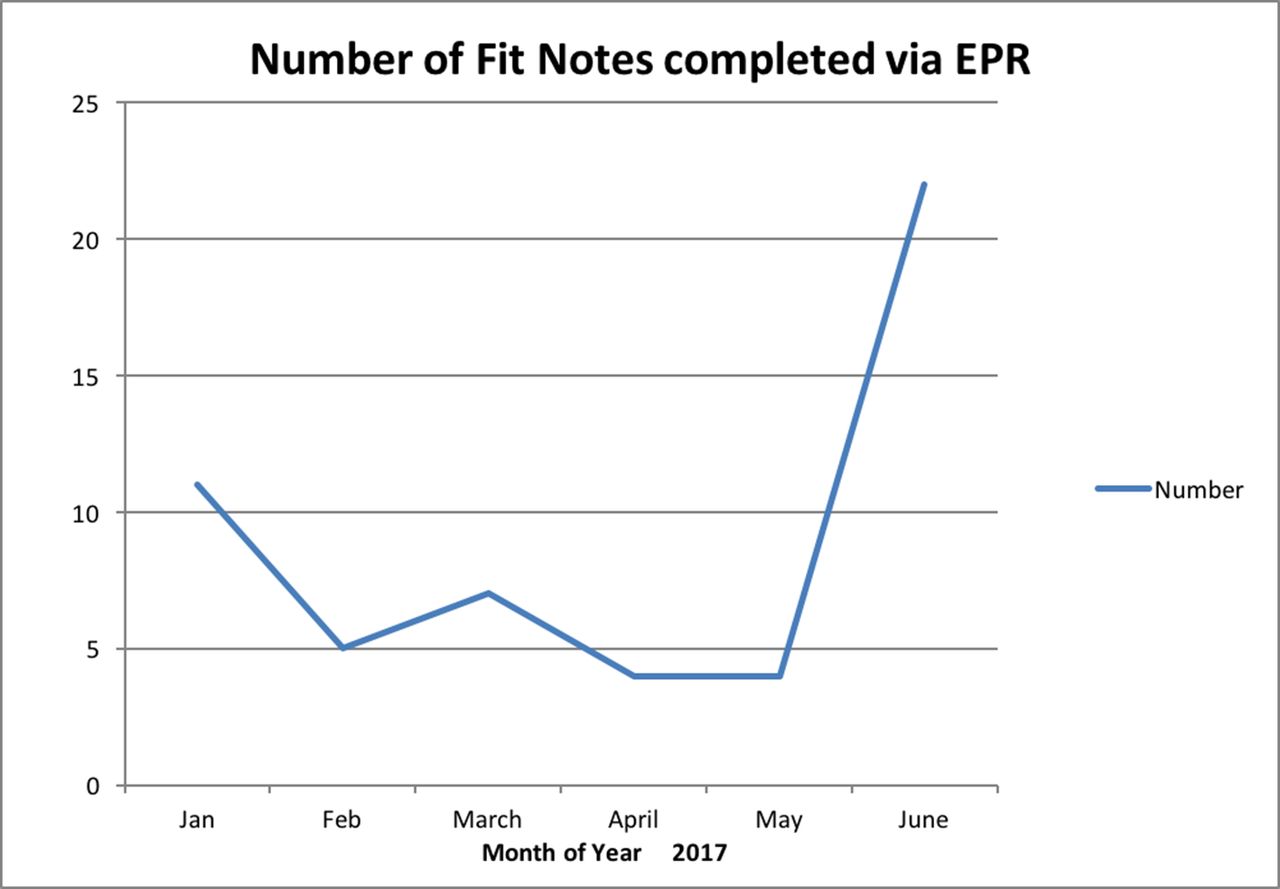
Number of Fit Notes completed via Electronic Patient Records (EPR) at Denmark Hill site from January to June 2017.

Number of Fit Notes completed via EPR at Denmark Hill by grade of requester.

{kind=link}
{kind=link}
{kind=link}
Number of quality alerts received by the trust on the issue of Fit Note non-issuance. Initiative began December 2016.
There has, however, been informal feedback that some departments have had difficulties printing the document or have had difficulties with lack of working printers in the clinical area. These issues were fed back to the clinical systems team and services managers, depending on the specific issue in order for them to be addressed.
Discussion
Despite targeted educational initiatives and trust-wide promotional campaigns, training in Fit Note procedure and awareness of the issue remain low. This reflects existing literature.8 12 One trust has addressed this issue by designing an e-learning module.12 This successfully improved confidence and visual identification of Fit Notes but both uptake of the module and subsequent issuing rates remained poor. This suggests that although e-learning modules increase knowledge of Fit Note policy, this does not translate into workplace practice. There is also a risk of overloading new starters with information at induction such that key messages like Fit Notes become lost. Targeted teaching early on in the academic year, such as to the foundation doctors or at a grand round helps to reduce this overload.
Although issuing Fit Notes may only form a small part of hospital doctors’ workload, this needs to be addressed in order to improve efficiency and more importantly, the patient experience. It is also crucial that all staff are aware of the benefits of returning to work. This includes nursing staff who play a key part in the patient journey. Nursing staff are often in post for longer than junior doctors, who rotate through hospitals as part of training programme. Although it is the doctors’ responsibility to issue Fit Notes, it is important that patients are given the correct information about how to obtain one and on their usage by all members of the clinical team. Raising awareness among all staff members encourages the sharing of best practice between staffing groups and helps to ensure the sustainability of the project. Low staff awareness within the hospital however, forms part of a wider issue. Research shows that as well as hospital staff, GPs, who issue Fit Notes much more than frequently than hospital staff, have not been properly trained to use the system.13
Penetrating a trust of this size with a message about a change in practice was difficult. Getting staff to read and engage with electronic communication ‘en masse’ is challenging. Using electronic questionnaires sent out via the staff bulletin to scope awareness had low uptake. This means that the responses elicited may not be an accurate reflection of the awareness of the larger staff body. We cannot, therefore, extrapolate the results to the rest of the trust. Staff engagement was much better when individuals were contacted directly and training taken to the department. However, this is more taxing on manpower and may be less sustainable in the long term.
At present, the form is available by electronic ordering at one site only. Once it is trust-wide, there will be less variance in practice across sites and it will allow us to keep track of Fit Note usage across the whole trust rather than just at one site. Incorporating consideration of Fit Note as a mandatory box in the discharge summary would help both to raise awareness and hopefully reduce the number of applicable patients being discharged without one. This was a goal set by the team at the start of the intervention, but it was not accomplished during the study period due to a number of external factors. We are continuing to work with the clinical systems team to ensure that it features in the redesign of the discharge summary.
Moving Fit Notes to an electronic order has allowed us to keep track of their issuing and reduces the risk of abuse of the document. However, successful implementation of any electronic document relies on sufficient hardware to ensure ease of printing. Otherwise, it is easy for staff to become disillusioned with the initiative and abandon the process.
It has been essential to communicate with our colleagues in primary care about this project. Fit Note best practice is a shared issue and is important that our colleagues are aware it is being addressed in secondary care. Working with the trust’s primary care liaison team was key in sharing this issue and facilitating an open dialogue with our primary care colleagues. Moving forward, having mandatory comments on Fit Note status as part of the discharge paperwork will allow our colleagues in general practice to be included in conversations had with patients, for example, ‘patient advised to self-certify for 7 days or less’ or ‘Fit Note issued with the following advice’.
Change is not always welcomed. Several staff expressed concerns at having to issue Fit Notes. In particular, concerns related to lack of occupational health training and lack of time were repeatedly voiced. There was also a perceived risk that patients would repeatedly attend hospital for Fit Notes and that they might be misused. On each occasion, it was reiterated that the documents were advisory only and that the advice given should be framed in terms of function. Staff were also pointed towards educational material they could use.
Conclusion
This project aimed to improve staff awareness of Fit Notes and reduce the number of patients being sent incorrectly to their GP. It was guided by a PDSA cycle. Targeted responses to quality alerts by a named member of staff were essential to ensure uptake of training by the involved departments, as well as providing a contact for any technical issues or questions.
Challenges remain in reaching all staff in a trust of this size and ongoing promotion will be needed to ensure capture of new starters. It is also important that the hardware can support any changes to software as otherwise lack of working printers, for instance, will become a barrier to issuing of Fit Notes. Nationally, there is a need to address the lack of awareness and lack of priority given to the issue at both the undergraduate and postgraduate medical levels as well as ensuring other members of the team, such as nursing staff and ward clerks, are aware of the correct procedure for issuing a Fit Note so that the patient does not receive conflicting or erroneous information.
Acknowledgments
The project team are grateful for the contributions of Richard Yorke, Clinical Systems Development Consultant and Rebecca Barnes, Primary Care Liaison Manager for all their assistance with the project.
Footnotes
Contributors TL proposed the idea, all authors contributed to the design and implementation of the proposal, AM, OK and CM contributed to data collection, AM drafted the manuscript and all authors made critical revisions and approved the final manuscript.
Disclaimer The views expressed are those of the authors and not necessarily those of the National Health Service or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.