Article Text

Abstract
General practice is at the forefront of the National Health Service, but is currently being overwhelmed by ever-increasing patient demand and financial constraints. Telephone consultations (TCs) have been used as a method to ease pressure on general practice. Many of these consultations are booked with general practioners (GPs), despite occasions when the patient could have either been signposted to self-help or offered an alternative service. This quality improvement project (QIP) aimed to evaluate the nature of TCs undertaken by GPs at our two practices; and whether the patients’ needs could have adequately been met without the involvement of a GP. Consultations where this was the case were deemed ‘possibly avoidable’, and those where involvement with a GP was the best option have been termed ‘essential’. A retrospective analysis was undertaken to establish a baseline figure for the proportion of possibly avoidable TCs in two practices. A new intervention was then introduced, with reception staff following a set of protocols when booking in patients. Patients who did not require a GP to deal with their query were actively signposted by reception staff to other allied healthcare professionals, non-medical staff or an alternative service at the time of booking their appointment. Two practices were involved in the study. After 2 Plan, Do, Study, Act (PDSA) cycles, the proportion of essential consultations taking place at both practices increased from 28.6% and 27.3% at baseline, to 82.6% and 71.4%, respectively. A lower number of possibly avoidable TCs equates to more time for essential TCs and greater value for money for the practice. Patient access to care is also improved, with patients directed to alternative and often quicker services which still meet their needs adequately. With the current system of primary care unable to cope with the demands it faces, interventions such as active signposting provide value for both GP practices and patients alike.
- general practice
- patient satisfaction
- quality improvement
- cost-effectiveness
- lean management
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
General practice is under immense pressure, with an ageing population; increase in long-term conditions and a reduction in whole time general practioner (GP) workforce per capita of the population accounting for much of the strain. With an increasing demand for appointments, telephone consultations (TCs) have been used to improve patient access to care by the GP surgeries involved in our study. While this has provided an effective alternative to more costly face to face consultations, staff noticed that many of these TCs were occupied by patients who may not have needed to speak to the GP at all and could have either been signposted to self-help, other allied healthcare professionals (AHPs) or dealt with by admin staff themselves.
This QIP aimed to evaluate the nature of TCs undertaken by GPs at our two practices and whether the patients’ needs could have adequately been met without the involvement of a GP. We also aimed to measure the impact of a new intervention allowing for safe substitution of TCs, with patients who did not require a GP to deal with their query being actively signposted by reception staff to other AHPs, non-medical staff or an alternative service at the time of booking. We hypothesised that this model could transfer time-consuming TCs from GPs to other staff or reduce the need for them altogether, hence freeing up appointments for patients who need to speak to or see the GP. As GPs are the most costly staff group in general practice, this would also represent a better allocation of financial resources for the practices.
Two locations were included in this study: Barlby Surgery and Kings Road Medical Centre (KRMC)—both London-based surgeries and members of the AT Medics group, which is responsible for providing primary care services through its 35 GP surgeries in London. The organisation promotes a culture of innovation and this specific project is one of the many methods through which they aim to enhance the service they can offer. The group has 2 20 000 registered patients in 16 London clinical commissioning groups (CCGs). Barlby and KRMC have 9600 and 11 500 patients, respectively. Both have recently been recognised as OUTSTANDING by CQC.
For the purposes of this study, any TCs that could not be safely substituted and required a GP have been classed as ‘essential’ consultations. Our aim was to increase the proportion of essential TCs booked at Barlby Surgery and KRMC from a baseline of 28.6% and 27.3%, respectively, to 70% in a 3-month time period. The standard was set with the aim of reducing possibly avoidable appointments while allowing a 30% margin with the understanding of patient preference—that some patients may still prefer to speak to a GP, and also erring on the side of caution to ensure that patient safety is not compromised.
Background
General practice is at the heart of the National Health Service (NHS), dealing with 90% of patient contacts within the NHS yet receiving less than a tenth of the total NHS budget.1 Despite NHS England promising an extra £2.4 billion of investment by 2020/2021, 2 it would be naïve to expect this to immediately solve all of the current problems in general practice. Among these problems is the level of stress faced by GPs. A recent Commonwealth Fund survey found that GPs in the UK had the highest stress levels of the 11 countries surveyed.3 In addition, just 22% felt the system worked well, indicating a much more deeply rooted issue which would need more than just investment to solve.3
At the heart of this dissatisfaction was GP workload, which was identified as one of the key issues affecting general practice in the GP Forward View.2 Figures from NHS England reflect this, stating that approximately 340 million consultations were carried out in general practice in 2011/2012, an increase of 300 million from 20 08.1 Additionally, a report commissioned by NHS England showed that 27% of GP appointments could have been avoided, with some individual clinicians reporting much higher figures.4 This begs the question, how can GP workload be better managed?
The King’s Fund highlighted various methods which would help general practice improve the current system.5 One such method was an improvement to patient access, with telephone and online triage potential methods of achieving this. Patient triage and TCs are already helping to reduce demand and pressure in primary care. TCs are an alternative to face-to-face consultations and are often quicker, cheaper and more convenient.6 A systematic review showed that TCs and triage reduced GP workload and revealed that at least 50% of calls could be managed by telephone advice alone (referral to face-to-face appointments were not needed).7
Dedicated TC clinics are employed in many of AT Medics’ practices, with an average cost of £8 per consultation compared with £17 for a face-to-face GP consultation. While reduction of the more costly face-to-face appointments represents a financial saving, there is also scope for further improvement. For example, a consultation with a physician’s associate or pharmacist would cost significantly less than with a GP. Using active signposting to safely reduce possibly avoidable appointments with GPs could lead to financial savings but in reality will free up time for GPs to focus on patients with more complex needs, therefore allowing longer consultations. From an organisational level (practice level), the practice is less susceptible to workforce pressures from GPs as patient needs could be met with AHPs or signposting.
Active signposting has come to the fore in recent years, with the aforementioned GP Forward View naming the method as the first of 10 high impact actions that could release capacity and thus free up GP time to care.2 As part of this, a large investment has also been created to enable the training of reception staff who would be implementing active signposting methods and many practices have begun employing them. Having said that, there is scarce data in the literature evaluating specific methods of implementing active signposting, and the results of doing so. We hope our QIP can provide an insight into the issue.
Measurement
Data were collected regarding two main domains: collection of TC data and staff member’s opinions on the new plans.
TC data were collected retrospectively, in the first week of December 2014 (baseline) and the first weeks of February and March 2015 (postimplementation), using the host clinical coded data. An additional set of data was collected at Barlby Surgery, in the first week of April 2015.
All TCs that occurred over a 5-day period were recorded and categorised as ‘essential’ (had to be handled by the GP) or ’possibly avoidable’. Possibly avoidable TCs were defined as those that could have been safely dealt with or without the need for a GP. For example, they could have been handled by administrative staff, AHPs or via self-help/online services. Possibly avoidable consultations were further categorised by the reason for the consultation. Microsoft Excel was used to analyse the data.
The baseline measurement showed that in Barlby Surgery, a total of 524 consultations were conducted over the course of 5 days and only 150 (28.6%) were essential. Similarly, only 27.3% (134/490) appointments were classified as essential over the same 5-day period at Kings Road Medical Centre.
Design
The initial results were striking and it became obvious that changes were needed. A new intervention to safely substitute potentially avoidable TCs was therefore adopted at both surgeries. The intervention consisted of seven protocols which were flow charts based on the most common reasons for possibly avoidable TC bookings. These protocols would be followed by reception staff at the time of booking, and outlined the process of actively signposting patients to the most relevant service—which in many cases would avoid a TC with a GP. Alternative services included another member of staff, or the patient completing the task themselves via the practice website. For example, someone calling asking for a sick note with duration of <7 days could be directed to the practice website where they could complete the task themselves, meaning they would not require a TC. Another example is the protocol used for test results, with figure 1 showing an example of the flow chart that was initially used.
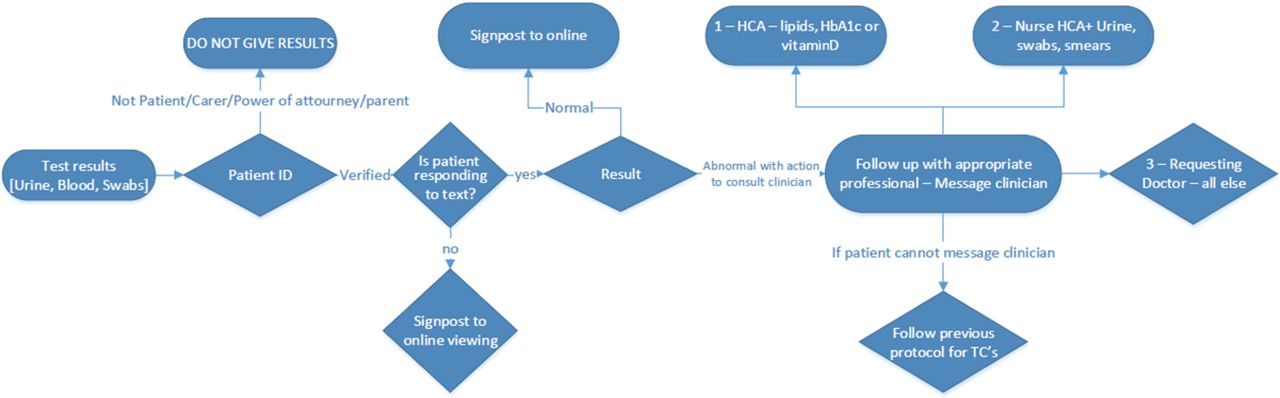
Example of one of the initial flowcharts used for PDSA 1HCA. HCA - healthcare assistant.
Receptionists were advised to respect patient preference, and also to book in the TC if there was any doubt whether or not it was essential. This aimed to prevent any compromise in patient safety or satisfaction.
These plans were applied throughout January and data were collected in the subsequent months. Our project team consisted of the authors of this study— with the other members of staff outlined below in PDSA 1.
Strategy
We employed the ‘Model of Improvement’ as a framework to guide our improvement project. This involved us first answering three key questions:
What are we trying to accomplish? Our aim was to increase the proportion of essential TCs booked at Barlby Surgery and KRMC to 70% in a 3-month time period.
How will we know that the change is an improvement? By collecting data evaluating the number of TCs taking place that were essential or possibly avoidable, as well as speaking to members of staff.
What change can we make that will result in improvement? The main idea for changed centred itself on a set of protocols which could be used by reception staff to actively signpost patients to the most appropriate service.
PDSA 1
Our first PDSA cycle involved the development of the protocol flow charts which would be used by receptionists when booking in TCs. These were developed through the following process:
Process mapping of the most common conditions/reasons for possibly avoidable TCs as identified by the baseline data;
Clinician led: this process was completed by one of the directors of AT Medics, who then drafted the protocols;
Workshops with non-participating practice (clinical meetings) to refine protocols (n=8);
Board review (GP directors n=6);
Second focus group with clinicians;
Implementation and training of reception staff.
The protocols were implemented in the two practices throughout January 2015; with all reception staff subsequently trained on their usage and paper copies of the flow charts visible at the reception desks. The aim of PDSA 1 was to increase the proportion of TCs being booked that were essential to >70%. We hypothesised that with adequate training of staff, this would be possible and the results somewhat reflected this. Although KRMC did not quite meet the target, both practices more than doubled the proportion of essential TCs being booked.
PDSA 2
The data collected after PDSA 1 broke down the number of essential and possibly avoidable TCs booked in by each staff member. It was obvious that certain members of staff were still not implementing the protocols correctly— and discussions in staff meetings made it clear that the protocols were not being used for every call. This led to one aspect of PDSA 2: which was the retraining of staff members by the management team, with extra input for specific members of the team. The protocols were also stuck on the wall in a smaller, more presentable format, which made it easier for reception staff to see them while on the phone. Our strategy for this part of the project hinged on engagement of the relevant members of staff so in addition to training, staff were regularly consulted in meetings and invited to give their feedback.
We anticipated that in addition to the changes as part of PDSA 2, staff would also become more comfortable with implementing the protocols from memory. We therefore hypothesised that PDSA 2 would further increase the percentage of TC bookings that were essential.
Results
Collection of TC data
Barlby Surgery
Our baseline data (pre-implementation) showed that a total of 524 TCs were conducted over the course of 5 days, and just 28.6% (150) of these were essential, meaning 71.4% were possibly avoidable.
In February, a month after implementation of the protocols as part of PDSA 1, a total of 188 TCs were conducted over the course of 5 days, and 74.5% (140/188) were essential. Following this, PDSA 2 was undertaken.
In March, following PDSA 2 a total of 187 TCs were conducted over the course of 5 days, and 82.9% (155/187) were essential, a further increase in the proportion of essential consultation.
In April, a total of 213 TCs were conducted over the course of 5 days, and 82.6% (176/213) were essential. Compared with the baseline figure of 28.6%, this represented a vast increase in the proportion of essential TCs. The total number of TCs in the 5-day measurement period in April was also 311 fewer than in December.
Kings Road Medical Centre
At KRMC, baseline data showed that a total of 490 TCs took place over a 5-day period, of which 134 (27.3%) were essential. This corresponded to just 27 out of the 96 TCs taking place on average per day being essential.
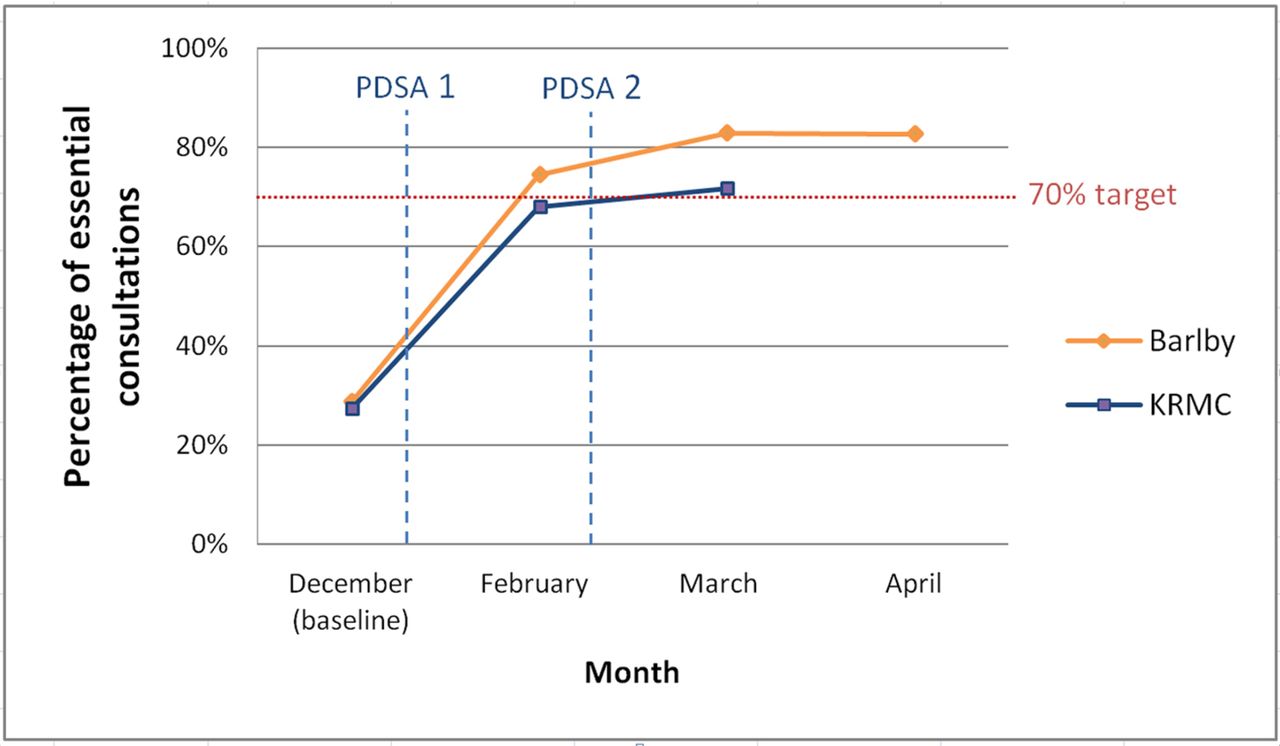
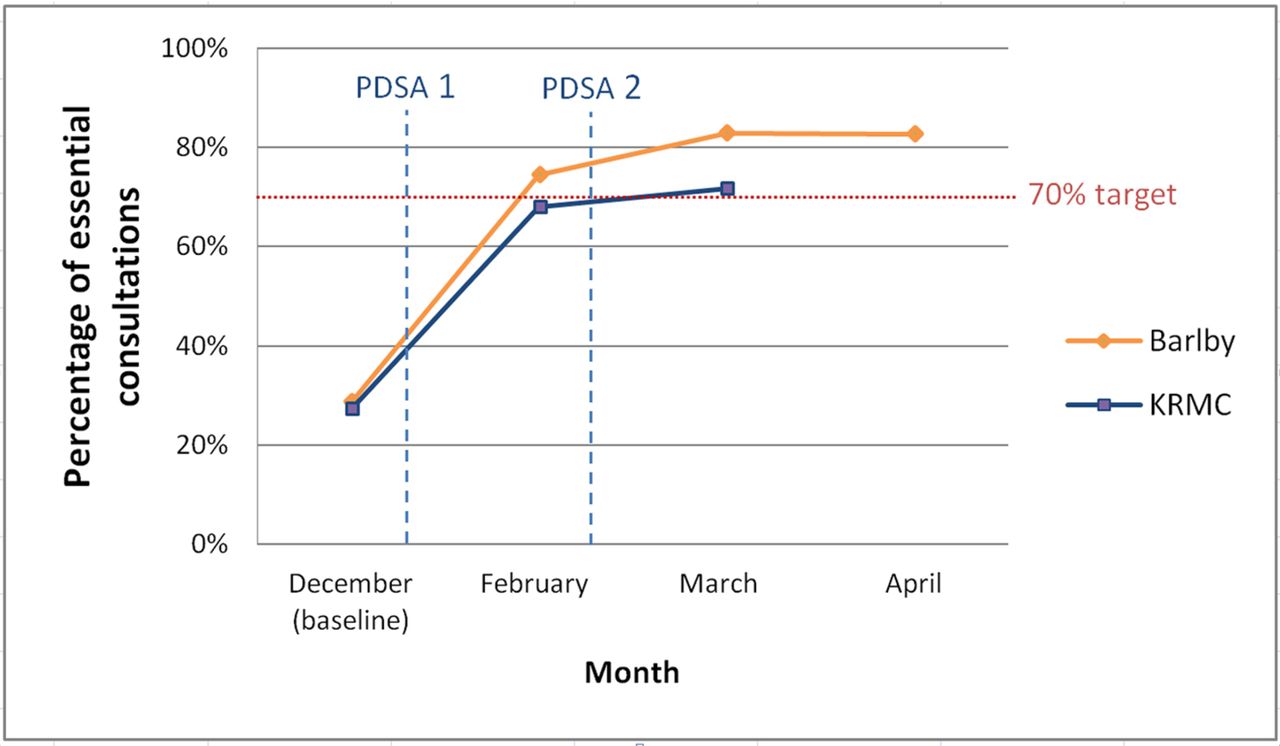
After implementation of the protocols, 68.0% (166/244) of TCs taking place were essential in February, with a further increase in March after PDSA 2, where 71.7% (218/304) of TCs were essential. Again, comparing the baseline figure of 27.3% to the figure after PDSA 2%–71.7%, there is a significant increase in the proportion of essential consultations. The total number of TCs taking place also fell from 490 at baseline to 304 after intervention. Figure 2 illustrates the results in a graphical format for both practices.
{kind=link}
{kind=link}
Graph showing change in percentage of of essential consultations over time.
Appreciative inquiries
Barlby Surgery
Two appreciative inquiries, one with a member of the administrative team and one with a GP, were conducted after PDSA 2. Both were very happy with the protocols and felt that they were working well. Patient access had greatly improved and the protocols had ‘significantly reduced the number of non-medical TCs’. This reduction meant that ‘a GP could concentrate on their skills of being a doctor, rather than conducting administrative work that could have been carried out by other staff'. Similar views were expressed in the meetings.
Kings Road Medical Centre
Appreciative inquiries were again conducted with one receptionist and one GP. The GP stated that there was a ‘noticeable decrease in the number of possibly avoidable TCs he had to deal with’. The receptionist commented on the ease of implementation of the protocols and the fact that he was able to follow lots of them off the top of his head without looking at the flow charts.
Lessons and limitations
The baseline results showing that almost three-quarters of TCs were possibly avoidable made for striking reading. The Primary Care Foundation’s figure of 27% of appointments being possibly avoidable was far lower than what was recorded at our practices where over half of appointments were deemed possibly avoidable, however the report did mention that individual clinicians did report figures much >27%.4 Variability between what individual clinicians considered as ‘possibly avoidable’ was also noted and that probably accounted for the high figure at our practices. Clinicians at the practices involved in the study know that there were many alternative services already in place that could have provided an alternative to a TC with a GP, leading to a lower threshold for appointments to be deemed possibly avoidable.
Our findings suggested that the implementation of protocols for active signposting had played a significant role in reducing possibly avoidable TC bookings, which additionally led to a large reduction in the total number of TCs taking place. This also represented an improvement in patient access to care, with many of the outcomes from having been signposted giving the patient a quicker response to their query, for example, being advised to access certain test results online which would give an immediate answer.
There was a very slight difference between results from the two practices, implying that any benefits of implementing the protocols would be influenced by the members of staff using them. This reinforced the importance of staff engagement and the need for proper training on use of the protocols, which was the focus of PDSA 2. This also reflected the value of gaining feedback from staff, who were ultimately the people who the implementation would effect. Their feedback allowed us to make further improvements to the protocols such as making them available in a more presentable and accessible format. It was clear that some of the protocols were slightly harder to follow than others, partly due to their complexity or layout which could often be unclear. Without prior knowledge or training, applying some of the protocols could be a challenge. Since conducting the study, refining the flowcharts and ensuring they are easy to follow has therefore been an ongoing focus and to aid this, AT Medics has since developed demonstrative videos as part of the receptionist training.
We were able to achieve the target of 70% essential TC bookings at both practices. In addition, we believe the results of our project are sustainable—represented by the target being maintained at the end of the study period which was a number of months after our original implementation. This was likely aided by the culture instilled within employees of AT Medics for whom innovation is the norm and adopting improved methods of functioning is encouraged. With the GP Forward View also providing a £45 million investment dedicated to training staff in areas such as the use of protocols for active signposting, the ability to commit resources to such activities is far higher than may have been the case in previous years, further adding to the likelihood of the intervention being sustainable.
It was important for us to note that signposting would not always be appropriate for certain patients, for example, those who are less comfortable with internet use for whom a TC may still be necessary, although again this often did not have to be with a GP. Additionally, some doctors may still want to have a conversation with their patient to maintain their doctor-patient relationship so directing them to another service may not be helpful. In these circumstances, reception staff were trained to be open and were not overly strict if the patient wanted to speak to a doctor or if there was any doubt whether the reason for booking was in fact possibly avoidable. A cautious approach was still encouraged so as not to compromise patient safety.
Conclusion
The current system of primary care is unable to cope with the demands of an ageing population; therefore, new ways to provide high-quality care in a quick and efficient manner are vital. Our intervention represents one method of improving management of GP workload, with the results of our study showing that active signposting can vastly reduce the proportion of possibly avoidable TCs, as well as the total number of TCs taking place. Patients could also benefit from improved access to care, with potentially quicker resolution of their problems. For example, the patient may be directed to online services where they could access certain results immediately, or arrange an appointment with an AHP much sooner than would have been possible with a GP.
The resulting saving in time and cost may also have a wider impact on care, with AT Medics in particular hoping that this will aid plans to increase the length of face-to-face consultation in the chronic care clinic. While we did not directly assess this in our study, there is also the possibility that a better managed workload would have a positive impact on stress levels for GP, which if the case would undoubtedly be beneficial for patient safety.
Following on from the success of the protocols, the results of this study were presented to the board of AT Medics, who subsequently approved their use in the remainder of the practices run by the company. Since the study period, the protocols have undergone further development including through the use of PDSA: evolving into ‘SMART’. This is a system used to train receptionists in active signposting, which incorporates an online module with videos demonstrating the application of each protocol. A limitation of the protocols was that at times, some of the flow charts could be hard to follow—particularly if you were looking at them without any training or prior experience. Being able to complement the flow charts with videos and role plays has been an important step in maximising their effectiveness and ease of use for reception staff. Adding new protocols where possible, and improving the layout of existing protocols has been a priority since the study was conducted and is still an ongoing process.
The work was recognised in a case study by the Nuffield Trust and was featured in an article by NHS England.8 9 SMART continues to be highly successful and has now become the norm in all of AT Medics’ practices. The protocols are also featured as a case study in the General Practice Development Plan—part of the GP forward view.2 We hope that our QIP gives evidence of the effectiveness of active signposting and encourages more practices to employ similar methods. Central to the success of the project was the culture of innovation at AT Medics, which we believe is a culture that needs to be more widely embraced to secure the sustainability of primary care as a whole.
Acknowledgments
The authors would like to thank all of the staff at the two study practices for their participation in the project. Without their enthusiasm for change, the results would not have been possible.
References
Footnotes
Contributors MAT was responsible for the original concept and design of the study, and played a primary role in developing and applying the implementation. FS and BS were involved in data collection and analysis, as well as drafting the manuscript which was revised by MAT.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.