Article Text

Abstract
Background The ability to review preoperative radiographs during trauma and orthopaedic surgery is essential for the surgeon to provide optimum treatment to the patient. However, due to current information technology (IT) systems, screen-savers frequently interrupt the ability to review images and theatre staff are not routinely available to deactivate the screen-saver. This prolongs theatre time for the patient and affects the quality of care provided. The aim of this quality improvement project was to improve the availability of radiographs for the surgeon to review intraoperatively.
Method/results Data were collected from all trauma and orthopaedic theatres at two hospital sites covering all subspecialties and including emergency and elective cases. Baseline measurements showed that the frequency of preoperative radiographs not interrupted during an operation was 0% (0/50). Following this the Trust’s IT systems were improved to prevent activation of the screen-saver on the theatre computers using the generic theatre login details. After the first-cycle intervention, data were collected showing 52% (14/27) of preoperative radiographs were not interrupted by a screen-saver. The cause for this result being less than expected was investigated and found to be due to an alternative computer login being used on the theatre computers at one of the hospital sites. Education of theatre staff was then undertaken to ensure the correct theatre login was used and notices to remind staff placed on the theatre computers. After the second-cycle intervention, data were collected showing that 100% (26/26) of preoperative radiographs were not interrupted during operative time allowing the surgeon to review images when required.
Conclusion/implications This quality improvement project has made changes to theatre IT systems and practices of theatre staff which has resulted in a significant improvement in the ability for the operating surgeon to review preoperative radiographs intraoperatively.
- healthcare quality improvement
- information technology
- surgery
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
The vast majority of trauma and orthopaedic operations require review of preoperative imaging intraoperatively to guide management of the patient. However, the information technology (IT) systems in place at this trust, comprising two hospitals with elective and emergency operations at one site and elective work at the other serving a population of 370 000 people, resulted in the inability to review these images.
The IT system in each theatre comprised a single computer with Microsoft Windows 8 operating system and the option to login with generic theatre or personal login details. Once logged in the radiographs were displayed using PACS software.
It was noted that during operations which lasted from 15 minutes to 5 hours the screen-savers on these computers would activate after 10 min. Sometimes if theatre staff such as operating department practitioners were available they would be able to deactivate it by interacting with the computer. However, if the computer was not interacted with for longer it would lock the user account and the theatre staff member would not be able to log back in unless they knew the password details for that specific account.
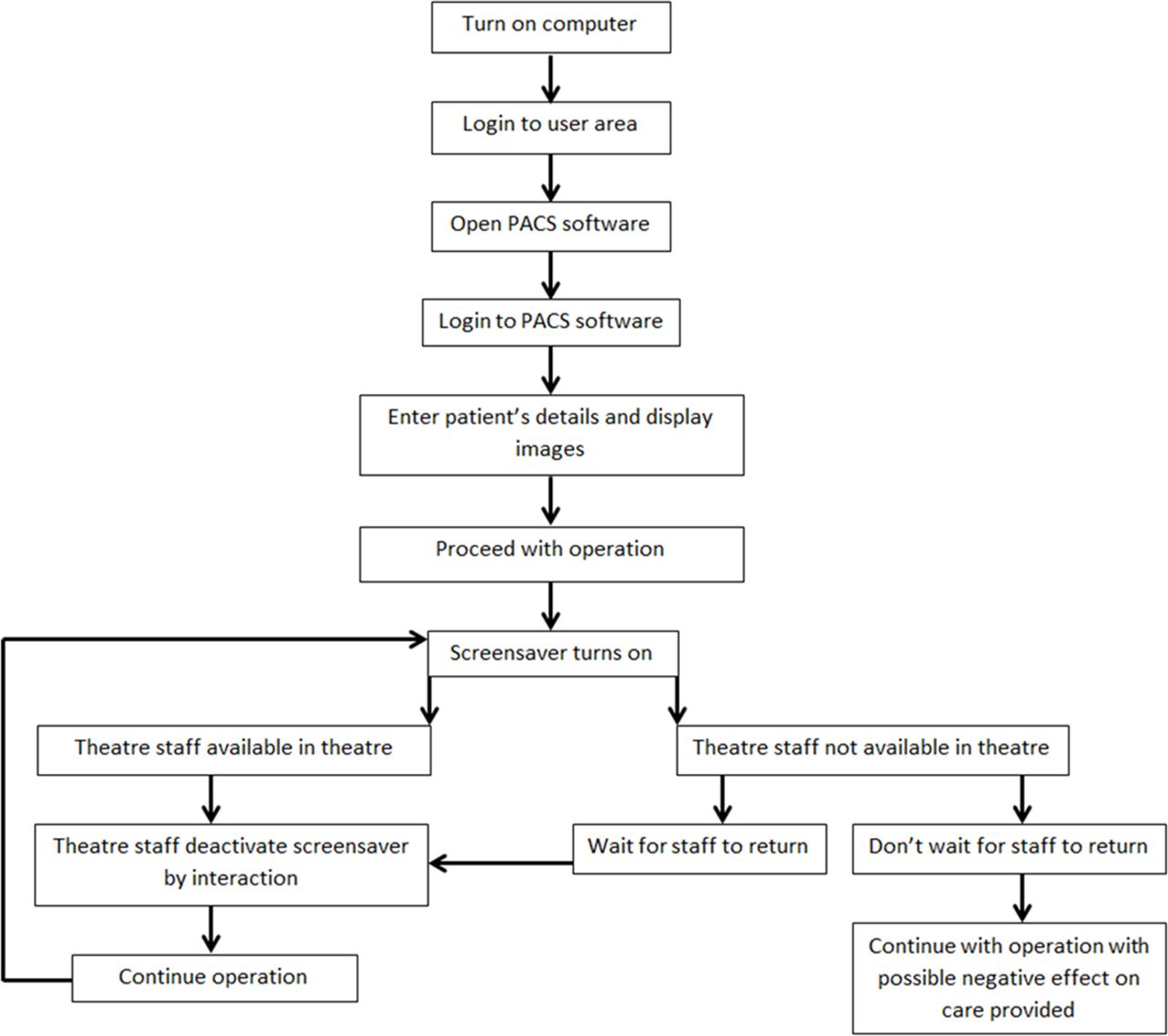
However, frequently staff were not available to do this and the operating surgeon either had to wait until they returned to the theatre or would have to continue without reviewing the images. This resulted in a reduction in the quality of care for the patient, a longer operating time or both (figure 1).

Process map.
The aim of this project was to completely prevent the interruption of onscreen theatre radiographs by theatre screen-savers during all operations in trauma and orthopaedic theatres across two hospital sites.
Background
There is no documented literature on this problem being recognised or having undergone quality improvement. Due to the similar IT systems used by different National Health Service trusts and from the experience of working in different regions, this is a common problem with a simple solution that can easily be employed by others.
Measurement
The total duration of data collection was 4 months. Baseline data were collected over a 2-month period. Data were collected daily on weekdays from one of a possible seven trauma and orthopaedic theatres that were running over the two hospital sites. The theatre list the data was collected from on that day was chosen by use of the random sampling function on Microsoft Excel with each theatre having an equal chance of being selected. Data were then collected using a proforma from each theatre case that happened to be on the chosen theatre list that day.
Of the 50 operations, the intraoperative radiographs were interrupted in 50 (100%) cases.
Subsequent data were collected by the same random sampling process continuously on weekdays throughout the rest of the project. It was established whether the outcomes were due to interventions by analysing the data points after the introduction of an intervention, for example, baseline data were collected for 2 months and then analysed. The first intervention was then introduced and data collected for 1 month and analysed followed by introduction of the second intervention with data collected for a further month and analysed.
Design
This project followed the Plan–Do–Study–Act (PDSA) cycle format. The project team consisted of the author with key figures in the IT service help desk as well as theatre staff. The focus of the first PDSA cycle was to improve the local IT systems. It was thought that if the IT team understood and appreciated the problem then intervention would be much more streamlined. It was originally thought that this would be a simple process that would take a short amount of time; therefore, an original project time of 3 months was expected. However, it was quickly learnt that to make changes to IT infrastructure across both sites was actually a very complex process that had to be approved by the higher levels of IT management. Frequent communications were essential to this project to ensure interventions were introduced and progression was made without excessive delay. However, the project time did have to be extended to 4 months. It was also expected that once the IT changes were made it would affect every computer in the trust regardless of login details used. It was later appreciated that due to the way IT systems are structured this was not the case and education of staff was needed to ensure the correct computer access was used to prevent the interruption of the radiographs. This was the focus of the second PDSA cycle.
Strategy
In the first PDSA cycle, the first step was to begin discussions with the IT team to highlight the issue and the negative effect on both the clinical care of patients and pace of the theatre lists in order to ensure it was understood this was an intervention worth implementing.
Initially progress was very slow; however, through further discussions, the pathway to implement this change started to appear. This involved submitting formal documents to the IT change board meeting which consisted of assessing the positives and negatives of the implementation before any intervention would be done. Improved quality of care and theatre list efficiency were obvious positives but had to be weighed against the negatives of cost, time, detrimental effect on computer monitors and possible risks of affecting other IT systems by implementing the change. Eventually through extensive communications the intervention was approved and the IT team were able to alter software to ensure that when using the theatre login details screen-savers were deactivated. Initially during this cycle progress was slow through email correspondence and due to being directed to various other departments within the IT team. However, once the correct team was identified and persistently followed up, progress was made. The important learning point from this cycle was the importance of communication and getting ‘buy in’ from the IT team which was only achieved through face-to-face conversations as opposed to electronic means. This was a valuable lesson learnt which was put into effect during the rest of the project preventing further delays in progress.
Measurement at the end of the first PDSA cycle was unsatisfactory after data collection. The reason for the lack of significant improvement was investigated and found to be due to theatre staff at one hospital site using personal login details. Because of limitations in the IT infrastructure, the IT team were only able to deactivate the screen-savers on the generic theatre login and not personal or ward login areas. The reason for this was the negative effect it would have on the Trusts’ monitors and because of security and confidentiality reasons the personal logins had to lock themselves out after a period of inactivity.
The second PDSA cycle involved identifying this issue and tackling the cause. It was decided that it was likely that all the theatre staff were not aware of the implementation and the need to use the generic theatre login details. The second implementation consisted of education of theatre staff through the use of verbal communication and notices placed around the theatre computers advising staff to use the theatre login and the reason why. Data were then collected to see the effect of this intervention. This cycle demonstrated the importance of ensuring all stakeholders and team members are aware of any changes made and appreciate the reasons for the change in practice. It was thought that education alone was not enough to make the changes; therefore, the addition of a notice on the monitor of each theatre computer was used to remind staff (figure 2).
Notice.
Results
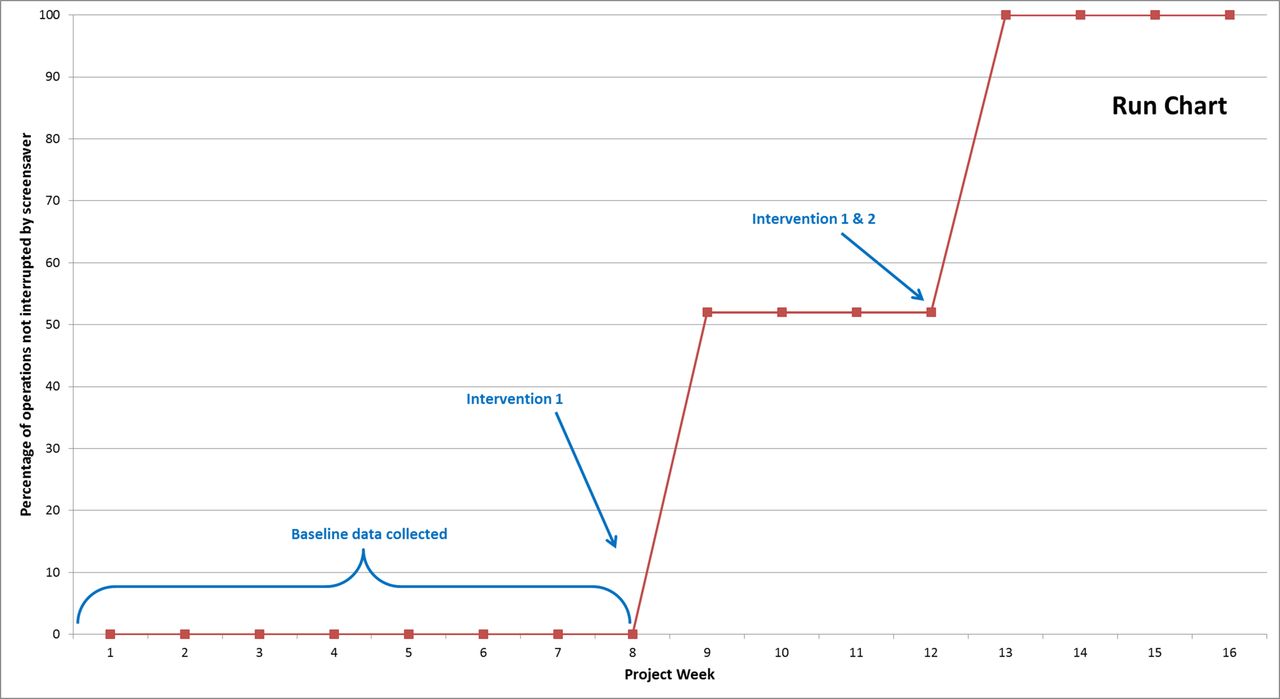
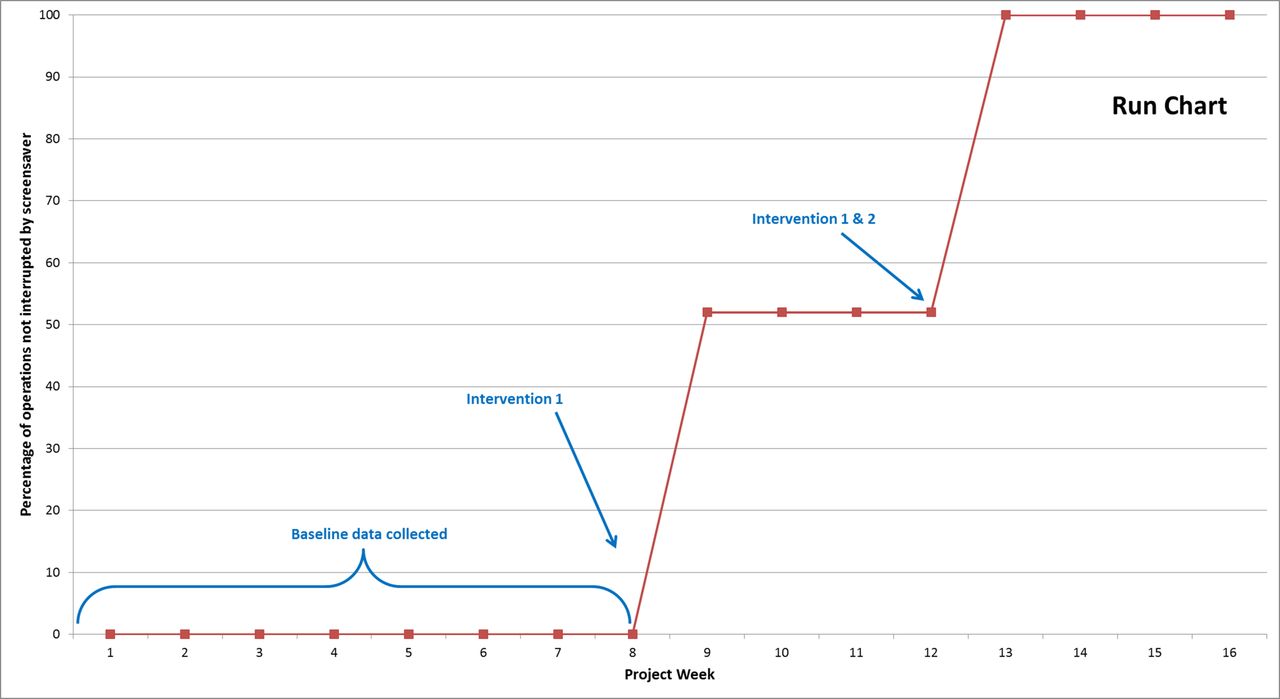
Data were recorded at the start of the project for baseline measurement and also continuously through the project with analysis of the data collected during each PDSA cycle. The frequency of preoperative radiographs not interrupted during an operation was originally 0% (0/50) at baseline. These data were collected continuously over a 2-month period. This improved after the first cycle to 52% (14/27). At the end of the second cycle, 100% (26/26) of radiographs were not interrupted for the duration of the operation. Data in the two cycles were collected over a 1-month period each.
From the results collected, the interventions made improvements at each cycle (figure 3).
{kind=link}
{kind=link}
{kind=link}
Run chart.
Lessons and limitations
The main lesson from this project and likely many improvement projects is that of the importance of communication and persistence in achieving the desired goal. Communication is known to be more effective when talking face-to-face than through electronic means such as email.1 This lesson was evidenced in this project and is most likely due to the ability of face-to-face to persuade others and communicate your enthusiasm for positive change. It is also much easier to ignore a faceless email. This lesson was learnt during the first cycle of the project and would be implemented from the start if the project was undertaken again.
This project was originally planned to be a 3-month project but was extended to 4 months due to slow progression initially in the first cycle. Once lessons had been learnt as described above, the project moved much quicker and progress was made. Initial data collection was over 2 months; however, due to time pressures only a maximum of 4 months for the project could be achieved. Therefore data collection for the first and second cycles was performed over a month each, resulting in a smaller number of data points taken after each cycle compared with baseline measurement. However, due to the significant change in results compared with baseline, it is not thought to have affected the conclusions made from these measurements.
Conclusion
Although not within the literature, it is generally known that radiographs are essential to the care given to trauma and orthopaedic patients within the theatre environment. Having preoperative imaging available, for example, of an anteroposterior pelvis radiograph when performing a total hip replacement is crucial for the operating surgeon to adjust the surgical procedure to provide the patient with the optimum postoperative outcome. This project identified a problem whereby the radiographs displayed on theatre computer monitors were continuously interrupted during the operation, preventing the operating surgeon from being able to assess the radiographs, resulting in a slowing of the theatre list and potentially causing negative care to the patient.
Methods to improve this problem were to alter the IT systems in place across two hospital sites and education of theatre staff. The project had a positive impact on the availability of radiographs intraoperatively, eventually resulting in 100% of radiographs being available to review throughout the surgical procedure, thereby achieving its primary aim. Through the use of notices and education of permanent theatre staff which has resulted in a change in day-to-day practice, it is expected that the level of improvement achieved during this project will continue.
Acknowledgments
Thank you to all the staff at Lancashire Teaching Hospitals for their help with the project.
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.