Article Text

Abstract
A high incidence of hypokalaemia was noted in Trauma and Orthopaedics of Ninewells Hospital. We sought to establish the reason behind this and implemented three PDSA cycles via questionnaires to 30 ward staff, both doctors and nurses over a 1 week period in December, February and July 2016. Key baseline measures include availability of IV fluids with 40mmol potassium on the wards, confidence prescribing or administering IV fluids with 40mmol potassium, necessity for cardiac monitoring during slow IV potassium replacement and recognition of confusion and learning need in this area. Interventions made include awareness and education session, departmental guideline, improving stock of IV fluids and hypokalaemia management pathway for mild, moderate and severe hypokalaemia. Post-intervention results showed 70% from 33% who said 40mmol IV potassium was available, 87% from 67% were confident prescribing or administering IV potassium and 70% from 27% were aware that cardiac monitoring was not necessary.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
In Ninewells Hospital, Dundee, Scotland, a high incidence of hypokalaemic patients was noted in the 78 bed trauma and orthopaedic wards. These were appropriately identified and acted on by the junior doctors, however it was reported that the prescriptions of IV potassium infusions were frequently not being administered for patients based on worsening electrolyte derangement. We wanted to find out why correction of this electrolyte derangement and appropriate treatment was delayed.
The reason for inefficient electrolyte replacement was multi-factorial. Preparations of 40mmol potassium in either 0.9% normal saline or 5% dextrose were frequently not available on the 3 wards. Junior doctors were also incorrectly informed by nursing staff that it was not appropriate to prescribe IV fluids with 40mmol potassium which were often prescribed at a slow rate due to the number of elderly patients with cardiac failure on the wards. There was much confusion due to uncertainty and current education and misinformation regarding administration of IV fluids with potassium with a lack of a departmental protocol to refer to. To add to the confusion, there was also a pharmacy stock list in the treatment room, which was frequently referred to and misinterpreted as the only accepted prescription on the wards as it did not include IV fluids with 40mmol potassium.
This issue posed a vicious cycle as hypokalaemic patients ended up getting IV fluids without potassium replacement, which caused further derangement of hypokalaemia. The enteral route was not an option for many trauma and orthopaedic patients, some of whom were fasting for theatre and many others with advanced dementia unable to eat or drink therefore efficient IV potassium was essential in correcting hypokalaemia via peripheral venous cannulae in these patients.
Our aim was to improve the availability of IV fluids with 40mmols potassium and staff awareness and confidence of safe, accurate and efficient prescription or administration of IV potassium within a seven month period in trauma and orthopaedics, in Ninewells Hospital.
Background
The normal range of plasma potassium is 3.5 −5.0 mmol/l. Hypokalaemia is defined as a serum potassium < 3.5 mmol/l. Severe hypokalaemia is defined as a K+ < 2.5 mmol/l.1
Hypokalaemia is one of the most common electrolyte abnormalities and has an incidence of 17-20% in hospitalised patients.2 ,3 Hypokalaemia is most frequently asymptomatic and identified on routine screening. Mild to moderate hypokalaemia if ignored may progress to life threatening severe hypokalaemia. Literature shows severe hypokalaemia is associated with potential life threatening complications such as cardiac arrhythmias, paralysis, rhabdomyolysis, diaphragmatic weakness resulting in cardiac or respiratory arrests.1 ,4–7
Causes of hypokalaemia include drugs such as diuretics, laxatives or steroids, gastrointestinal loss such as diarrhoea, renal loss such as renal tubular disorders or diabetes insipidus, endocrine disorders such as Cushing's syndrome, metabolic alkalosis, hypomagnesaemia, poor dietary intake and treatment strategies used for hyperkalaemia.1
A study by Jensen et el found that hypokalaemia <2.9 mmol/l at admission were associated with an increased 7-day and 8-30 day mortality. Whether this association is causal or associative, hypokalaemia is an interesting prognostic marker of fatal outcome.3
There are limited reported projects trying to solve this problem. One similar project is reported in the BMJ Quality Improvement Reports journal in which there was an uncertainty of appropriate investigation and management of hypokalaemia including lack of medication review, ECG assessments, and blood monitoring leading to hyperkalaemia.8 This was not an issue in our study however the interventions made and improvement outcomes were similar.
Dundee, with a population of around 170,000 is the fourth principal city in Scotland. Ninewells Hospital is the main teaching hospital associated with the University of Dundee and the major acute service provider in the area. The hospital was opened in 1974 and with 810 acute beds is one of the largest units of its kind in the British Isles, and was specifically designed with the medical school and hospital integrated in a way that provides for growth and change in future years. Trauma surgery is concentrated on the Ninewells site where complex trauma, multiple injuries , hand trauma and urgent paediatric trauma is carried out as well as elective cases. Our quality improvement project was carried out across three wards initially until the fourth ward was re-opened over the winter bed crisis in Trauma and Orthopaedics, Ninewells Hospital. In the first two improvement cycles, this study was conducted in three wards, which had a total of 66 beds. The final improvement cycle occurred after an additional ward was reopened involving a total of 92 beds in the Trauma and Orthopaedic wards. With regards to the staff, the same total number of staff were working across these wards.
Baseline measurement
We collected data via questionnaires targeted at foundation doctors and nurses on the three trauma and orthopaedic wards in Ninewells Hospital. Data was collected over a one week period in February 2016. Ten questionnaires were distributed to each ward and we had a 100% response rate as thirty questionnaires were completed and analysed. Four key measurements collected were used in subsequent questionnaires to compare the results. These were as follows:
Availability of IV fluids with 40mmol potassium on the wards
Confidence prescribing or administering a bag of IV fluids with 40mmol potassium
Necessity for cardiac monitoring during slow IV potassium replacement
Recognition of confusion and need for continuous education in this area
The questionnaire had “yes”, “no” or “do not know” as answers with a free text box for additional information. The questionnaires were repeated in June and September 2016 after interventions(outlined below) were made to assess improvement in knowledge and awareness of the four key measurements.
Design
Baseline data showed there was a significant problem with IV potassium replacement and an improvement was necessary. A series of interventions were made including developing a guideline approved by the department on hypokalaemia management. Posters were laminated and put up in all wards. Education sessions were held explaining the poster. Junior doctors and nurses were targeted at the handover. Emails were sent to update all members of staff. Discussions were held with the departmental pharmacist and IV fluid bags (0.9% sodium chloride and 5% dextorse) with potassium were made available on all wards.
Strategy
PDSA Cycle 1: Discussions were held involving a consultant Orthopaedic surgeon and lead pharmacists for trauma and orthopaedics regarding this issue and the quality improvement project was designed. To address this issue, education and awareness talks were held targeting all junior doctors and nursing staff of all three wards. Teaching sessions were held before or after nursing handover. Email update on hypokalaemia management was circulated to all staff. With the involvement of the pharmacist, all wards were stocked with fluid bags of 40mmol potassium in saline and dextrose. A survey was carried out in February 2016 to determine the underlying cause and baseline knowledge, skills and confidence of prescribing and administering IV potassium in trauma and orthopaedic department. This confirmed that there was a need to further address IV potassium replacement.
PDSA Cycle 2: To aid the educational sessions, a departmental hypokalaemia guideline was designed and created into a simple poster with the input of the pharmacist, consultants, nursing staff and junior doctors which was available in all three wards in the doctors' room, treatment rooms and nursing handover room. After a four month period of implementing change, we re-audited the junior doctors and nursing staff and found an overall improvement in awareness and confidence in prescribing and administration of IV potassium for hypokaleamic patients. These findings were presented at the Trauma and Orthopaedic Clinical Effectiveness meeting in June 2016 to increase the awareness of this issue to staff of all levels including consultant surgeons, trainees, senior charge nurses and foundation doctors. It was recognised that this project was a simple intervention that would potentially improve patient care and safety.
PDSA Cycle 3: Six months following implementations of PDSA Cycles 1-2, a third survey was held over a one week period in September 2016 with a new set of foundation doctors and nurses. This was held over 4 wards as the department had at that time gained another 26-bed ward. It was evident from feedback received that while staff had now gained the knowledge and awareness that potassium replacement was necessary, a simple hypokalaemia flowchart was requested to guide the replacement of potassium for the different levels of severity and this was designed for the replacement of mild, moderate and severe hypokalaemia on trauma and orthopaedics (See supplementary - IV potassium replacement guide).
supplementary - IV potassium replacement guide
Results
A total of 30 surveys were completed in the 1 week period in February, June and September 2016. The response rates were 100% for all cycles. We did not discriminate between staff who had already responded on previous surveys as we were more interested to see an improvement in awareness and confidence among staff however, there were also new staff who were included and this includes new bank nurses and foundation doctors due to changeover of rotation.
Twenty four nurses and six foundation doctors completed the initial survey. Of these 47% (n=14) said 40mmol IV potassium in 0.9% sodium chloride or 5% dextrose was not available on the wards. Only 33%(n=10) said it was available and 20%(n=6) did not know if it was available. Sixty seven percent(n=20) were confident prescribing or administering IV fluids with 40mmol potassium. When asked if cardiac monitoring was necessary during slow IV replacement of potassium, 56% (n=17) said yes and 17%(n=5) did not know. Only 27%(n=8) were aware that cardiac monitoring was not necessary. A majority surveyed, 93% (n=28) felt there was a need for further learning around this issue.
After four months of various interventions outlined above, the same survey was carried out and showed a significant improvement in knowledge and confidence in prescribing and administering IV potassium replacement. Over a 1 week period in June 2016, twenty two nurses and eight doctors completed the survey. Sixty percent(n=18) were aware that 40mmol IV potassium fluid bags were available on the ward, 33%(n=10) said no, and 7%(n=2) did not know if it was available. Almost all surveyed, 97% (n=29) were confident prescribing or administering IV potassium. Eighty three percent of those asked were aware that cardiac monitoring was not necessary when running a slow bag of IV fluids with 40mmol of potassium, 10%(n=3) said it was necessary and 7%(n=2) did not know. Eighty three percent(n=25) of those surveyed this time, felt there was still a learning need over hypokalaemia management.
The third survey was conducted in September 2016, and had twenty three nurses and seven doctors complete the survey. Seventy percent (n=21) were aware of the new guidelines on hypokalaemina. Seventy percent (n=21) also said 40mmol IV potassium fluid bags were available on the ward, 10% (n=3) said no, and 20% (n=6) did not know. Confidence was still high with 87%(n=26) stating confidence and only 13%(n=4) not confident prescribing or administering IV potassium. Seventy percent (n=21) were also aware that cardiac monitoring was not necessary, 27%(n=8) said it was necessary and 3%(n=1) did not know. When asked if there was still a need for continuous education, 83% (n=25) said yes, and 17% (n=5) said no.
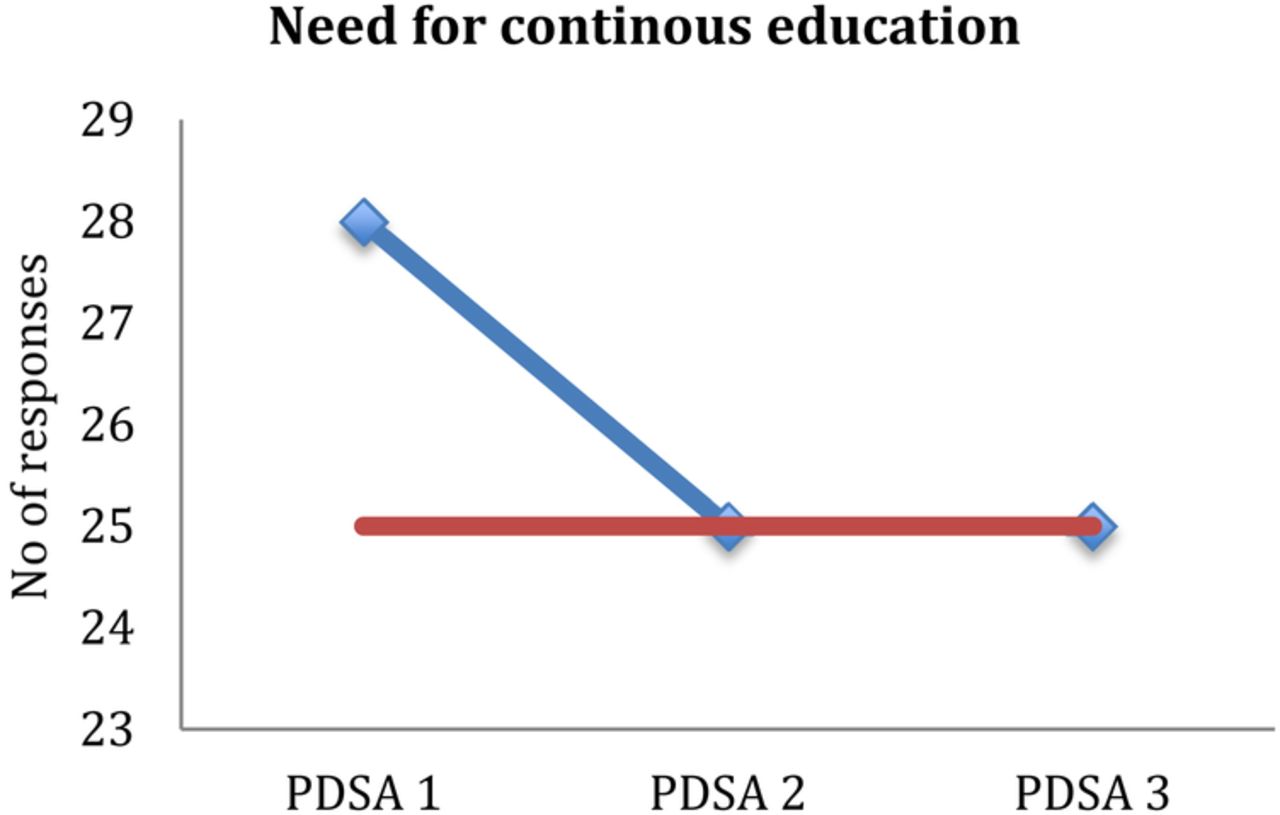
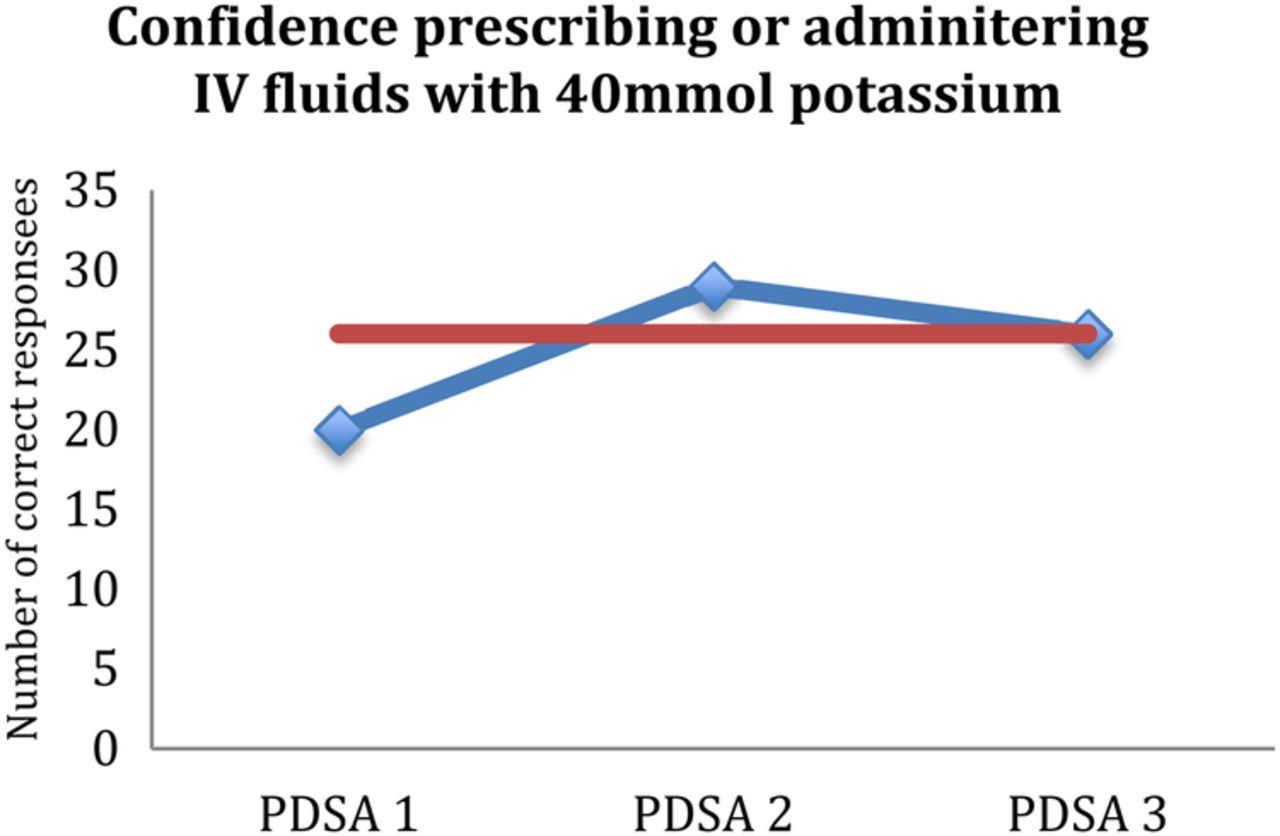
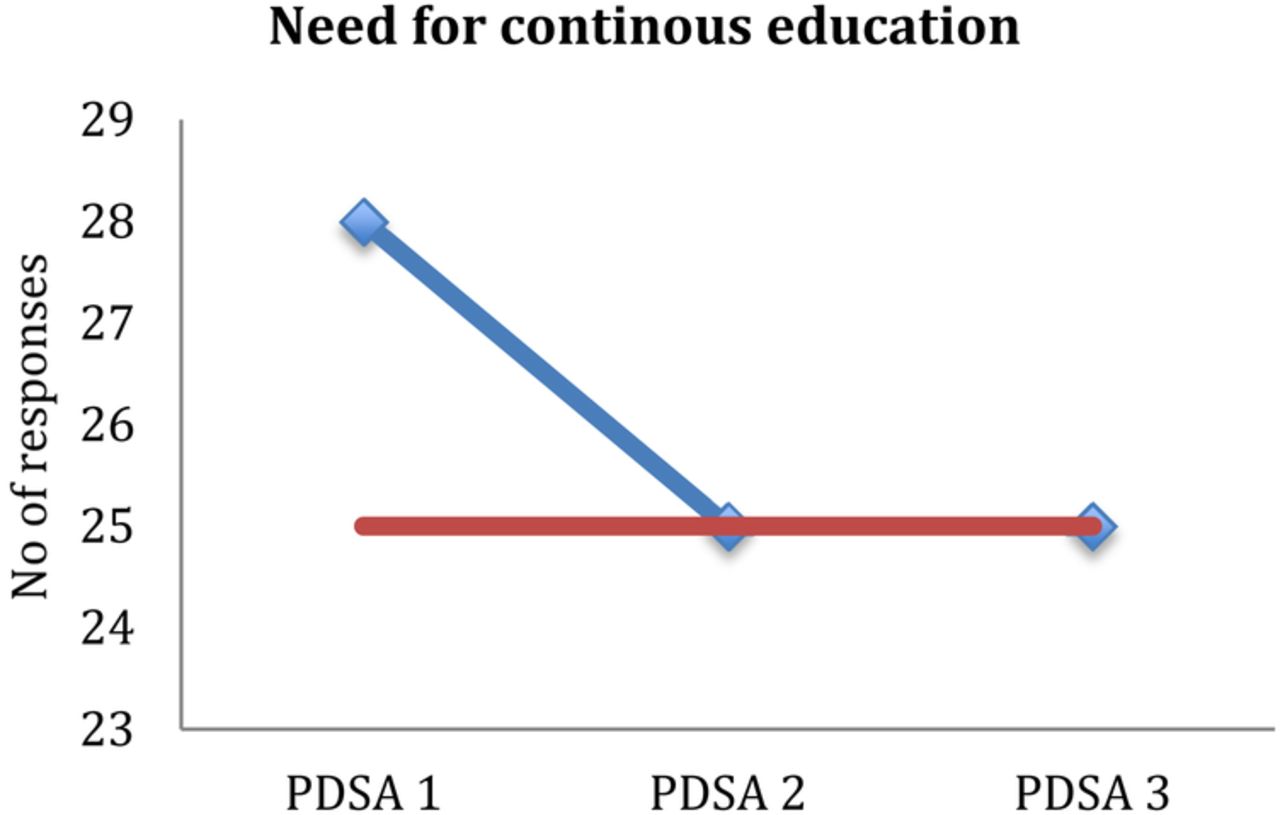
Overall, availability (figure 1) and confidence (figure 2) prescribing or administering IV fluids with 40mmol potassium improved as a result of this project. Staff were also aware that cardiac monitoring was not required while IV fluid with 40mmol potassium was administered (figure 3). Figure 4 shows that there is always a need for continuous medical education, despite staff feeling they are now aware and confident with IV potassium replacement.

Availability of IV fluid with 40mmol potassium

Confidence prescribing or administering IV fluids with 40mmol potassium

Necessity for cardiac monitoring during IV fluid replacement
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Need for continuous education
Lessons and limitations
Foundation doctors are very good at identifying areas of department weakness and opportunities for quality improvement however they are open to difficulties in sustaining changes with time as doctors rotate every four months. It is also beneficial to have senior and pharmacy support and input into foundation doctor led quality improvement project for continuity of the project. Through this quality improvement project we have learnt that it would be useful to design a hypokalaemia protocol and flowchart to help provide opportunities to junior doctors and nursing staff for their continuous professional development.
This is a preliminary study and a larger sample is needed to be able to apply quantitative statistics. However, despite this, the survey does show that improvements can be achieved by simple measures of educating and updating staff thus improving patient care.
One of the limitations identified is the small sample size of this project. It was difficult obtaining more than 30 doctors and nurses in a one week period as the same staff were on most day or night shifts for the week. It may be a better idea to conduct the survey over a longer period of time with more frequent data collection to capture more staff. Our improvement cycles were also conducted over long time periods with multiple interventions made. In hindsight, we could have used the PDSA cycles to test single changes on a smaller scale. A more objective measure of improvement would be to identify hypokalaemic blood results and the time taken to act and repeat blood samples. This is best studied once education is provided to staff and misconceptions addressed.
Other limitations include the addition of a fourth ward to trauma and orthopaedics during the seven months of this quality improvement project. It was in the third cycle that it was evident that the additional ward did not have the new hypokalaemia guideline on the ward. The large number of wards and staff increases the time and effort needed to disseminate information among staff. There were also a large number of bank nurses working in these wards and it is difficult to disseminate information to these nurses as they are not always based on the orthopaedic wards. During changeover of foundation doctors, information on hypokalaemia guidance and the departmental protocol needs to be delivered during the induction period to ensure continuity in improvement of hypokalaemia management. This could have been done between the second and third survey when the new foundation doctors started the Trauma and Orthopaedic rotation.
Conclusion
This was a simple reproducible quality improvement project that has managed to address some misconceptions surrounding hypokalaemia management. Our results have shown an improvement in the awareness, and confidence in prescribing and administering IV potassium replacement as well as improving the availability of these IV fluid bags on all trauma and orthopaedic wards. This will inevitably lead to safe and improved patient care however continued work is needed to ensure changes are sustainable. We are in the process of developing the hypokalamia flow chart for guidance on management of hypokalaemia and will need to continue to audit the progress with time.
Acknowledgments
Special mention to Emma Clark, Pharmacist on Trauma and Orthopaedics for her input and support with this quality improvement project.
Footnotes
Declaration of interests Nothing to declare
Ethical approval This project was deemed an improvement study and not a study on human subjects. Local policy meant that ethical approval was not required.