Article Text

Abstract
The National Confidential Enquiry into Patient Outcomes and Death (NCEPOD) report ‘Time to Intervene’ (2012) stated that in a substantial number of cases, resuscitation is attempted when it was thought a ‘do not attempt cardiopulmonary resuscitation’ (DNACPR) decision should have been in place. Early decisions about CPR status and advance planning about limits of care now form part of national recommendations by the UK Resuscitation Council (2016).
Treatment escalation plans (TEP) document what level of treatment intervention would be appropriate if a patient were to become acutely unwell and were not previously formally in place at King's College Hospital. A unifying paper based form was successfully piloted in the Acute Medical Unit, introducing the TEP and bringing together decision making around both treatment escalation and CPR status. Subsequently an electronic order-set for CPR status and treatment escalation was launched in April 2015 which led to a highly visible CPR and escalation status banner on the main screen at the top of the patient's electronic record.
Ultimately due to further iterations in the electronic process by December 2016, all escalation decisions for acutely admitted patients now have high quality supporting, explanatory documentation with 100% having TEPs in place.
There is now widespread multidisciplinary engagement in the process of defining limits of care for acutely admitted medical patients within the first 14 hours of admission and a strategy for rolling this process out across all the divisions of the hospital through our Deteriorating Patient Group (DPG).
The collaborative design with acute medical, palliative and intensive care teams and the high visibility provided by the electronic process in the Electronic Patient Record (EPR) has enhanced communication with these teams, patients, nursing staff and the multidisciplinary team by ensuring clarity through a universally understood process about escalation and CPR.
Clarity and openness about these discussions have been welcomed by patient focus groups facilitated via our acute medicine patient experience committee. There has been a shift in medical culture where transparency about limits of care has contributed to improving patient safety and quality of care through reducing unnecessary CPR supported by focus groups of staff.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The project took place at King's College Hospital NHS Foundation Trust, London, UK. It serves an inner city population of 700,000 but also serves as a tertiary referral centre. The Acute Medical Unit (AMU), has 60 beds and admits approximately 15,500 medical patients each year. Multidisciplinary care is provided for all adult medical admissions with a wide range of presenting pathology. The unit is staffed by 12 Consultants and a 6 monthly-rotating team of 24 junior doctors, and a nursing staff of approximately 100. Key supporting members of the multidisciplinary care team include unit-based Pharmacists, Dieticians, Social Workers, Occupational Therapists and Physiotherapists.
The Deteriorating Patient Group is a King's College Hospital Trust board group which evaluates a number of key processes relating to prevention of deteriorating patients across the hospital in line with up-to-date evidence to ensure patient safety is optimised. It particularly explores the interface with critical care and emergency medicine to ensure the best outcomes for patients.
CPR is too often an instinctive result of an unforeseen emergency and survival to discharge from an in-hospital cardiac arrest is less than 20% in all age groups, and even in survivors there is significant morbidity. Inappropriate CPR is when the situation is considered futile reflecting both a low chance of survival and likely poorer quality of life afterwards if spontaneous circulation is returned.1 The Trust had previously used a DNACPR form that did not incorporate decisions about levels of intervention, which inevitably led to some lack of clarity around decisions for out-of-hours teams. From a retrospective analysis conducted by our resuscitation department, the DPG highlighted that 10% of patients received what was considered to be inappropriate CPR during 2013-2014 (i.e. 75/750 patients) and this was the chief trigger for our wide-scale collaborative quality improvement endeavour.
The overall aim of this project was to improve the quality of recording CPR status and treatment escalation plans with a view to reducing the risk of inappropriate CPR through early transparent patient engagement and multidisciplinary decision making. This would ultimately contribute towards optimising quality of care. The primary objective was to develop and embed a Trust-wide intervention to promote early collaborative decisions about limits of care and CPR status simultaneously, with standardised supporting documentation.
The project was sanctioned by the DPG to ensure a standardized approach to our recording of CPR and escalation decisions on the front line. Our team consisted of representative Consultants from Acute Medicine, General Internal Medicine, Palliative Care, and Intensive Care, Nursing leads from the care group, IT representation from the Head of our EPR system and a project manager. Implementation was carried out by the AMU multidisciplinary teams including attending Consultants, junior doctors, nursing staff and with support from Management and Information technology.
We aimed for 100% compliance with a documented CPR decision and TEP within 14 hours of admission for all medical patients. We were aware that in the long term an electronic process would be more likely to ensure visibility and sustainability. A one year time-line of the process planned for the project to allow the development from paper to electronic records is outlined with the qualitative and quantitative impacts described, the first 6-months refer to the development phase and the second 6-months to the period after institution and re-audit.
Background
The General Medical Council (GMC), British Medical Association (BMA) and UK Resuscitation Council all advocate early patient engagement and negotiation towards shared decision making about resuscitation.2 Decisions about CPR are frequently omitted, and even if decided upon poorly documented and communicated.3–6 Palliative care teams in hospital are under utilised and often contacted late in the patient pathway for end of life care.7–9 The NCEPOD, report ‘Time to Intervene’ (2012) stated that in a substantial number of cases resuscitation was attempted when a DNACPR decision should have been made earlier: only 10% of cases had a documented decision, on admission, as to the resuscitation status. This was due to a failure to formulate an appropriate risk assessment regarding potential to deteriorate and or detailing the escalation plan on admission. This can lead to adverse medicolegal outcomes, especially if decisions are then determined by ‘out-of-hours‘ junior medical teams without detailed understanding of the situation or clinical background10. Healthcare professionals do not find it easy to raise the issue of treatment escalation or de-escalation or discuss CPR with their patients.4
For patients who are unlikely to benefit from CPR, quality of care can be improved by documenting a management guide in the event of clinical deterioration i.e. a TEP. This subsequently minimises the risk of on-call teams commencing treatments with limited benefit and that are not aligned with the patient's pre-stated wishes. TEPs can therefore ensure the treatments given are in the best interests of the patient documenting what treatment options would be appropriate if that patient were to become acutely unwell. TEPs are increasingly being used in acute hospital trusts to outline limits of care, however these are often paper based and inconsistently adopted, with wide variability at implementation.11–13
The DPG aligned with the London Commissioning Standards in agreeing that all acutely admitted medical patients were to have TEPs established and CPR decisions made and both clearly documented in a standardised format within 14 hours of admission onto the acute medical take i.e. this was advocated by the point of the first post-take consultant review.
Baseline measurement
A baseline audit of practice on the AMU was undertaken for two weeks for all acute admissions in November 2014. All electronic notes and paper notes for each of the 382 patients included were screened for the presence or absence of a documented CPR status or any reference to an escalation plan in the event of deterioration. At this time electronic notes were considered inpatient notes whilst accident and emergency notes remained paper based and were subsequently scanned into the electronic record. At baseline, the prevalence of documentation for reference to CPR status was 11.8% (n=45) and for reference to treatment escalation or limits of care was 11.2% (n=42) for patients admitted to the AMU. These were mostly weekend plans or specific overnight instructions based on outstanding results and investigations and did not pertain to the holistic outcomes for the patient overall.
Design
The initial pilot intervention was an easy-to-use two-sided paper based form, comprising a CPR section and a TEP section (Figure 1). This was initially piloted on paper and then incorporated into an electronic orderset for CPR and TEP. The design of the TEP form was a collaborative endeavour based upon expertise of Consultants and contributions from junior doctors and frontline multidisciplinary nursing staff and allied health professionals within acute medicine, intensive care, palliative care. There was additional input from the resuscitation and IT departments regarding viability. The basic structure of the original DNACPR form was maintained.

The pilot form was made widely available on the AMU supported by education for consultants, junior doctors and the acute medical unit staff. Data was again collected for the presence of a documented TEP/DNACPR decision in the medical notes of each patient, both paper and electronic.
The results of improved documentation rates were presented to the AMU Consultant team, at a quarterly internal audit meeting and to a Hospital wide multidisciplinary audience at the medical Grand Round in October 2015. Further to the pilot success, an identical electronic TEP form and accompanying order-set was designed to encourage recording of CPR status and TEP for all acute admissions. The orderset for CPR status and TEP and the electronic TEP form was designed by the EPR team, discussed at the Documents and Legal Review Panel and subsequently instituted formally as trust protocol to be completed for all acute admissions within the first 14 hours. The electronic CPR form was already in existence but the order-set widely drew attention to compliance with this to ensure CPR status together with TEP was always actively considered and recorded for all patients.
Strategy
Three PDSA cycles were used to develop the final TEP.
PDSA Cycle 1
An Acute Medicine Patient Experience Committee was established in January 2015, with patient representation, to facilitate the discussion and planning process of CPR status and TEP. The committee initiated five patient focus groups. Four out of five groups reported that they would want to be involved in making decisions about their wishes for both CPR status and TEP. Patients were clear that they would not object to these issues being raised in the early stages of an acute hospital admission and valued clarity. Drawbacks highlighted were that some patients felt that raising the topic at all might be considered to be directly linked to their prognosis on that admission, or that those with chronic disability might be selected out for discussion leading to feelings of discrimination or judgement. Transparency was fundamental to all patients and it was strongly felt that such discussions should be a routine policy for all patients upon admission to avoid feeling selected out or that the topic was being raised only because of imminent deterioration. This underpinned our practice going forward in terms of embedding the consideration and documentation of CPR status and escalation for all our patients regardless.
A paper-based TEP, including CPR status, was collaboratively designed between acute medicine, intensive care, elderly medicine and palliative care to ensure that limits of care were clearly documented for the multidisciplinary team. The advice of consultants was sought because they frequently engage in decision making about what treatments would be in an individual's best interests in the event of clinical deterioration and are ultimately responsible for patient care. It was agreed that resuscitative treatment options in order of least invasive to the most invasive were outlined and described in levels of organ support. Level 1 care being defined as ward based care, Level 2 as single organ support including non-invasive ventilation in a high dependency environment and level 3 as multi-organ support or invasive ventilation. A section allowing for de-escalation was included so that dying or terminal patients were recognised early and that end of life care could be instituted. (Figure 1). This version was made available to all medical staff via the weekly protected educational meetings for junior doctors and at the consultant meetings. The form was explained step-by step and case examples discussed, all questions addressed.
Each morning for two consecutive weeks, over one hundred TEP forms were distributed across the emergency department, ambulatory care unit and two acute medical unit ward bases. The forms were carried by the junior doctors to allow completion by the Consultant Physicians after every new patient review and filled with in the paper notes and an entry added to the electronic patient records. All staff were reminded to complete the form at the morning handover meeting.
After two weeks of this pilot (n=150 patients) the documentation of TEP and CPR decisions on AMU had improved from 11.8% to 21.2%.
PDSA Cycle 2
The resulting changes were recognised as a benefit to both patients and clinicians in terms of encouraging early decision making in the interests of patient safety. As Kings College Hospital operates an electronic patient record system (EPR) and the intervention was not sustainable in terms of distributing the volume of paper based forms on a daily basis, an electronic order set was designed for both TEP and CPR status with the EPR team and launched on April 1st 2015. Consultant physicians, identified as clinical champions, helped to embed the use of this order-set for every patient, aiming to encourage clinicians to consider both the possibility of deterioration and the appropriateness of individual treatment modalities when making decisions about CPR.
The trust progressed with support from the DPG and legal team to formally launch the TEP electronically on EPR. This was published as trust protocol for recording CPR status and TEP on the intranet. The EPR was linked to ‘ward-view’ screens in staff-only areas so that escalation and CPR status could clearly be seen, for all AMU patients, by the nursing & medical staff. The changes in TEP and CPR status are easily reflected electronically and ceilings of care and DNACPR decisions are highlighted for each patient at midday board rounds to ensure the discussion is up to date and all teams are made fully aware to ensure good communication and patient safety.
Based upon the monthly percentage of CPR decisions recorded, on paper forms, from January to March 2015 (18.8±2.1%), the study had 90% power, at alpha level of 0.01, to detect an improvement to 24%, or greater, of CPR status recorded with electronic documentation with 6-months or more of follow-up data.
PDSA Cycle 3
To ensure the legally binding UK Resuscitation Council national form was electronically completed in addition to completion of the order-set fields alone, a further iteration to the electronic process incorporating a direct link to the CPR form was successfully launched on 1st December 2016.
Results
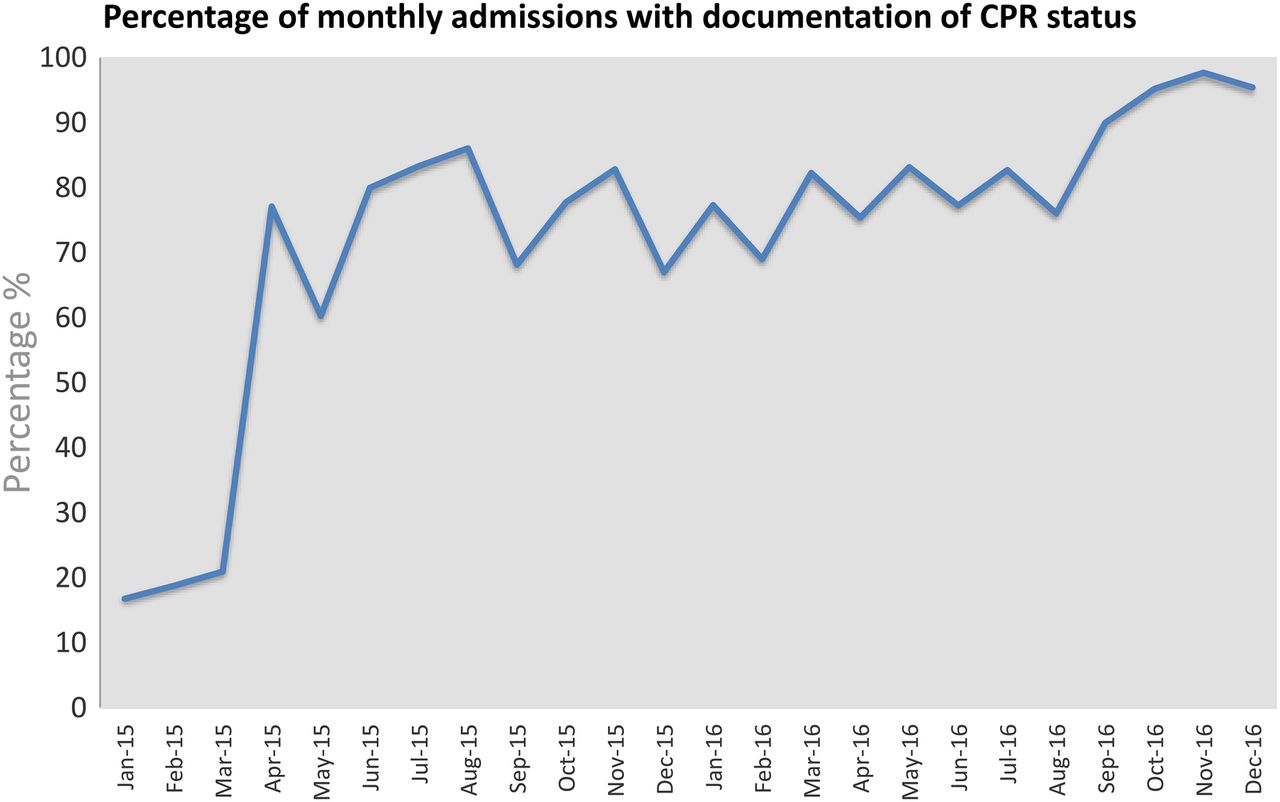
The documentation of CPR decisions (within 14 hours of acute admission) increased from 18.8±2.1% Jan 2015 to March 2015 (paper-based order forms) to 80.2±9.6 April 2015 to December 2016 (electronic order forms); two-tailed independent t-test, P<0.0001. (Figure 2)
{kind=link}
{kind=link}
After just six months, feedback from practising divisions indicated that clinicians felt empowered to make early TEP/CPR decisions and were involving the multidisciplinary team. Nurses felt increasingly confident in efficiently escalating care and involving critical care outreach to ensure the most effective outcomes for patients.
A further iteration to the electronic process was launched on 1st December 2016. This involves a (mandatory) direct link to be completed after entering the CPR status on the home page of the patient's notes, to the supporting documentation.
Lessons and limitations
Undertaking a new trust wide initiative regarding treatment escalation plans for patients requires engagement of all the key stake holders from the outset including intensive care to palliative care, all acute specialties, nursing teams, allied health professionals, IT and the hospital board.
An important limitation to this work is a lack of feedback about the qualitative personal impact upon patients in practice. While patient focus groups from the first PDSA cycle suggested that it would potentially reduce patient anxiety and ease decision making for doctors, there were also concerns raised that patients' may link these discussions to assuming their prognosis was poor, or that they were being targeted due to age or disability. This study did not collect further feedback from the patients' perspective after the form was introduced and therefore it is not clear at this point whether the advent of the TEP/CPR acute admissions process improved the patient and family experience. This would be valuable to evaluate in a further improvement study.
Ensuring compliance from senior health care professionals in utilising the electronic order-set to record CPR status/TEP upon admission for every patient involved a huge cultural shift and active championing on a daily basis and is a limitation in that there was variable engagement. This was mitigated through actively making this a question highlighted for every patient in AMU and geriatrics at board rounds by our clinical administrators, so this practice was increasingly adhered to.
Quality of discussions among clinicians remains variable and is a further limitation, with many reluctant to undertake the task in acute or outpatient settings. Implementing trust-wide training on the recording process and improving quality of discussions has been a challenging process with our palliative care team driving this work and requires engagement and support of all clinical and nursing leads to support implementation and practice.
As this is resource intensive sustainability of training is another limitation as consistent encouragement and continuous training across the trust is required. This is particularly crucial as these discussions may be challenging in those acute admissions lacking capacity to this particular issue for reasons such as delirium, dementia, fluctuating consciousness, acute alcohol withdrawal etc to name but a few. As such the default position would be to ensure the decision is recorded as full escalation unless a previous established decision has been clearly identified with evidence of previous patient involvement. All healthcare professionals would ideally be up to date on the process, legal and multidisciplinary aspects and there are now further discussions taking place about potentially embedding this within trust mandatory training. For now, it has been made part of the EPR lesson plan for all new users to ensure familiarity with the process.
As the electronic CPR form originally lay out-with the order-set until December 2016, we found up to 20% of patients with DNACPR selected on the order-set did not have an accompanying explanatory legal CPR form, although there was often evidence of patient discussions on the EPR clinical notes. This would mean a legal obligation to perform CPR unless the situation could be rapidly evaluated with a consensus agreement by the crash team in real time. We have since launched a new unifying electronic process in December 2016 that ensures the selection of DNACPR within the orderset automatically opens the electronic CPR form to promote completion of this essential legal documentation.
In the longer term, we hope to evaluate the potential statistical impact upon inappropriate cardiac arrest and while preliminary data suggests that there is already significant improvement, it is acknowledged this may be multifactorial.
Next steps
Although we have demonstrated an improvement in the documentation of CPR status and TEP within the acute care setting, the question remains as to whether this is the most appropriate time and place to discuss limits of care and patient wishes.
Patients may feel uncomfortable hearing about the subject for the first time from a frontline hospital doctor they may have never met, especially when they are already under significant stress having been admitted with a potentially critical illness. Clinical responsibility may be repeatedly transferred in an acute care setting, which also compromises the continuity of the discussion if it is held for the first time in this forum. Patients presenting acutely may lack capacity to discuss their thoughts, feelings and concerns due to delirium, dementia, withdrawal from alcohol, reduced consciousness due to head injury or sepsis, exacerbation of mental illness
In future, improvement goals could explore understanding how much discussion of CPR status and TEP is taking place in the community setting and how to ensure this information is transferred across the primary/secondary care interface.
Our experience with rolling out the TEP suggests that by ensuring this is discussed transparently with all our patients, it avoids any patient feeling like they are being singled out, isolated or targeted because of their medical condition. Another alternative, therefore, is for the trust to explore implementing these discussions in the outpatient clinic. Being able to dedicate time to discussing this in detail when the patient is well might enable patients to have confidence that even if they are in an obtunded state, everything possible will be done to their satisfaction and they have been involved in the decision making about their care and understand any limits and reasons for this in advance.
Supplying written information in leaflet form for patients and families when they are admitted to acute admissions units regarding CPR decision-making, media displays in areas with screens and electronic pages for patients with evidence based extractions from key reports may be useful complements to raise awareness and transparency that these crucial conversations are mandatory in the interests of optimising patient safety and delivering high quality care. We are currently exploring this further through our Acute Medicine Patient Experience Committee.
Conclusion
The evolution of a TEP form is not specific to Kings College Hospital and many trusts in the UK are now adopting similar approaches11–12, however the translation to an electronic mandatory process has increased visibility of this important part of patient management and embedded it in local culture ensuring it is a key consideration for all acute admissions. The approach and findings of this project are therefore widely applicable to other UK trusts.
By tailoring the individual patient's clinical management and documenting it clearly upon admission in a standardized universally understood trust-wide format, ambiguity in critical cases is systematically avoiding, especially where patients may deteriorate out of hours. The concept was that treatment modalities are ideally discussed with the patient early in their illness while capacity to make specific decisions about future life sustaining treatments is still preserved. This was considered especially important in patients at high risk of deterioration determined by any or a combination of multiple co-morbidities, pre-morbid performance status, physiological reserve and organ failures. In addition it was considered vital that there would be clear communication documented in the clinical notes with the patient and their next-of-kin, or legal power of attorney where relevant and reference to any advanced directive could be reviewed.
The aim of establishing a trust-wide Treatment Escalation Plan has optimised multidisciplinary communication, particularly that with our critical care outreach team and intensive care colleagues regarding rapid escalation of treatment. It has also enhanced communication with our palliative care colleagues in recognising the need for appropriate de-escalation of treatment in terminal cases and encouraging their early involvement. Clearly defining any limits of treatment for each patient upon admission gives both clinical multidisciplinary teams and patients' confidence in the delivery of high quality medical care, especially out-of-hours — when senior decision-makers may not be available.
The sophisticated and streamlined supporting electronic process has enhanced the dissemination of this information effectively to the multidisciplinary team and encourages early collaborative decision making and good record keeping in line with GMC good medical practice. It has also ensured high rates of compliance with the process which encourages visibility and transparency and is sustainable for the future.
Acknowledgments
Dr Zohra Khattak, Dr Geraldine Walters, Jennifer Karno, Dr Jane Evans
Footnotes
Declaration of interests Nothing to declare
Ethical approval According to the policy activities that constitute research at Kings College Hospital, London, as guided by the HRA this project met criteria for operational improvement exempt from ethics review as it is categorised as a service evaluation.