Article Text

Abstract
Patients who are high risk high cost (HRHC), those with severe or multiple medical issues, and the chronically ill elderly are major drivers of rising health care costs.1 The HRHC patients with complex health conditions and functional limitations may likely go to emergency rooms and hospitals, need more supportive services, and use long-term care facilities.2 As a result, these patient populations are vulnerable to fragmented care and “falling through the cracks”.2 A large county health and hospital system in California, USA introduced evidence-based interventions in accordance with the Triple AIM3 focused on patient-centered health care, prevention, health maintenance, and safe transitions across the care continuum. The pilot program embedded a Transitional Care Manager (TCM) within an outpatient Family Medicine clinic to proactively assist HRHC patients with outreach assistance, problem-solving and facilitating smooth transitions of care. This initiative is supported by a collaborative team that included physicians, nurses, specialists, health educator, and pharmacist. The initial 50 patients showed a decrease in Emergency Department (ED) encounters (pre-vs post intervention: 33 vs 17) and hospital admissions (pre-vs post intervention: 32 vs 11), improved patient outcomes, and cost saving. As an example, one patient had 1 ED visit and 5 hospital admission with total charges of $217,355.75 in the 6 months' pre-intervention with no recurrence of ED or hospital admissions in the 6 months of TCM enrollment. The preliminary findings showed improvement of patient-centered outcomes, quality of care, and resource utilization however more data is required.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Patients with complex medical issues encounter various barriers to health care2 because the health care system is complex that may result in systemic failure and compromised patient safety.4 These barriers to care are at patient, provider, and systems level, involving limited patient knowledge, resource constraints, and communication issues.5 These systemic failures among national and global health institutions are identified in different transitions of care.6
Background
Amongst the major priorities of healthcare are improving individual patient care, improving the health of populations, and reducing overall healthcare costs in accordance to the Triple Aim as described by the Institute for Healthcare Improvement.3 Clients with complex medical and psychosocial issues are the greatest threat to any healthcare system. These factors not only affect health and quality of life, but are also major drivers of health care costs, threatening health care affordability.7 These concerns have led to a public focus and an increase in research studies. The topics searched related to this program were on risk screening tools, risk assessment factors, case management models, interventions aimed at avoiding readmission, advanced care planning, and team communication and collaboration. Many institutions have been unsuccessful in implementing these models because of the complexity and barriers to implementation. A large county health and hospital system in California, USA introduced evidence-based interventions focused on patient-centered health care, prevention, health maintenance, and safe transitions across the care continuum. The health care system is the community's health care safety net providing medical services to the county residents regardless to their inability to pay. It has ten (10) Primary Care clinics distributed in different locations. The pilot program embedded a Transitional Care Manager (TCM) within an outpatient family medicine clinic to proactively assist HRHC patients with outreach assistance, problem-solving and facilitating smooth transitions of care. Clearly, the need for evidence -based solutions must be aligned with the organization's mission and vision in providing high quality care to ensure success.
Baseline measurement
Avoidable readmissions and frequent use of the Emergency Rooms are major problems facing the U.S. healthcare system. A high rate of readmission reflects low quality care, increase costs, and decreased patient satisfaction. The USA Medicare federal health insurance for >65 y.o. began fining hospitals with high rates of avoidable admissions starting 2012. Medicare's 30-day hospital readmission rate in 2013 was 17.5%20. On the other hand, the healthcare institution's readmission rate is 13.54% for Quarter 3 of 2014 according to the internal tracking. The organization initiative is to downtrend the readmission rates. To address this issue, the pilot program tracked patient-centered outcomes, quality of care, and resource utilization. The feasibility of the interventions was also investigated. The baseline measurements included Emergency Department (ED) encounter frequencies, hospital admission frequencies, cost, and qualitative measurements. The initial baseline measurements included Emergency Department (ED) encounters and hospital admission frequencies. The six-month pre-implementation time-period included 50 patient referrals from 8/1/2014 to 3/24/2015. The 50-patient chart review from 2/1/2014 to 9/24/2014 showed 29 patients had 33 ED encounters and 18 patients had a total of 32 hospital admissions.
Design
The aim of this project is to incorporate a Transitional Care Manager (TCM) within an outpatient family medicine clinic to proactively assist HRHC patients with outreach assistance, problem-solving and facilitating smooth transitions of care. Extensive literature reviews were done during the development of this project. Different theories were explored to determine the best evidence on improving outcomes of HRHC patients.
We expected that patient-centered outcomes, quality of care, and resource utilization could be improved with this type of program.9 The pilot project adapted the IHI Triple AIM3 Initiative: improve the experience of care (quality and satisfaction), improve the health of populations, and reduce the per capita cost of health care. The setting of the pilot program is a Primary Care Medical Home (PCMH) clinic. The PCMH patient-centered model offers comprehensive care, coordinated care, and accessible services which demonstrates commitment to quality and safety.10 Primary care providers pro-actively identified high risk patients and refer to the TCM. Initial TCM patient referral stratification guidelines included patients readmitted within 30-90 days, hospitalized, multiple ER visits, provider referrals, diagnoses with readmission Centers for Medicare and Medicaid Services penalties such as Congestive Heart Failure, Pneumonia, Acute Myocardial Infarction and high utilizers: sepsis, homeless, chronic diseases: cancer, diabetes, obesity, etc. Risk factors were identified such as principal diagnosis, poor health literacy, polypharmacy, prior hospitalization, physical limitations, psychological co-morbidities, poor social support, and palliative care.11 ED encounters were also included. Language services were offered at first contact. The patient transition contact could be a clinic visit, follow-up phone call, or family conference. The interventions provided included, but were not limited to: medical diagnosis education, noting allergies, diet discussions, medication review, scheduling appointments, following up results, organizing services and Durable Medical Equipment, brainstorming with patient and family on what to do when problems arise,12 and providing their After Visit Summary (AVS) after the clinic visit. In addition, the multi-disciplinary care team assisted with outreach, problem solving and navigation across the care continuum with a goal of improving patient outcomes and avoiding costly use of the ED and inpatient resources. The TCM workflow is shown in Figure 1.

TCM Workflow
Strategy
The pilot setting was in a three-story Medical Home Clinic providing family medical practice, specialty, laboratory, pharmacy, and administrative services. The family practice consisted of nine (9) providers with about 1500 paneled patients. The pilot program aimed to provide Transitional Care Management services to patients with complex medical problems needing moderate or highly complex medical decision making during transitions in care.13 For example, transitions may be made from an acute hospital, rehabilitation hospital, long-term care or skilled nursing facility to a patient's community setting such as home, rest home, or assisted living facility.2
The pilot was executed in two phases, each involved the proposal of the project, testing the proposed process change, studying the effects then acting on the recommendations.14
The first phase explored the effect of incorporating a part-time Transitional Care Manager and new guidelines into the outpatient Family Medicine Clinic to assist with patient transitions of care. The planning phase involved high-level leadership of both inpatient and outpatient services meeting with the assigned TCM to design and introduce the proposed program. The Transitional Care Manager was a part-time registered nurse with multiple roles, including augmenting the clinic staff and piloting this project. Developing the TCM role description took into account TCM patient stratification, risk assessment tool,11 care management models,9 interventions aimed at avoiding readmission,12 ,15 advanced care planning,16 communications, and team collaboration.
The TCM work flow that was developed and implemented is shown in Figure 1. Primary care providers pro-actively identified high-risk patients and referred them to the TCM according to the criteria determined during planning. Then the TCM oversaw the patient transition.
In July 2014, the TCM role was assigned and the referral process began. Table 1 shows the comparison of a control group of 16 active patient encounter before and after the change. In the 6 months prior to their initial encounter under the new procedures, the control group recorded 21 ED encounters and 13 hospital admissions or rate of 21/(6*16) = .219 ED encounters per patient per month and 13/(6*16) = .135 hospitalizations per patient per month.
In the months following their initial encounter with the new process, these patients experienced rates of 12/(52) = .231 ED encounters per patient per month and 4/(52) = .077 hospitalizations per patient per month, respectively.
Studying these results of the first phase suggested additional opportunities to improve the TCM process.
The second phase examined the effects of further revisions to the TCM process. In this second phase, an awareness campaign explained the TCM initiative and reinforcing the original changes along with updated information with the providers, charge nurses, and staff. The pilot program team sought and received buy-in from the health educator and pharmacy resident. The health educator provided classes on healthy eating, stress management, and managing chronic diseases. The resident pharmacist provided medication counselling and reconciled complex medications. The awareness campaign increased the number of patients referred to the TCM by 34.
To facilitate referrals and decrease non-patient care tasks, a TCM charting template was incorporated into the Electronic Medical Record (EMR). This template was reviewed by all major stakeholders, experiencing multiple revisions. Some data, such as, ED encounters and hospitalizations previously required manual reporting, which became time consuming and resulted in inconsistent use of the template. With the template incorporated into the EMR, the data could be extracted automatically extracted and the fields filled in. In addition, using the EMR email system facilitated timely updating and sharing of patient information among the TCM and inpatient providers and specialty cares. The resident pharmacist and health educator could also view TCM documentation in the EMR.
The effects of the improvement during the second phase are summarized in Table 2 along with the result from the previous study. The second study showed additional improvement. The sample of 34 patients showed a decrease in ED encounters from 12 to 5 and hospital admissions from 19 to 7 in the 6 months before and after instituting the revised TCM procedure.
This reflects a decrease from 12/ (6*34) = .059 ED encounters per patient per month to an average 5/(6*34) = .025 ED encounters per patient per month. Similarly, average hospitalizations per patient per month, decreased from 19/ (6*34) = .093 before the change to 7/ (6*34) = .034 after the change.
Results
Table 3 illustrates the improvements achieved over each of the two cycles. Both studies show a material reduction in the average number of patient encounter per month.
One patient pre-TCM services with 1 ED visit and 5 hospital admission had total charges of $217,355.75, with 6 months TCM interventions no recurrence of ED and hospital admission. Considering that 38% of charges are actual costs, this represents a cost-savings to the institution of $ 82,595. This is shown in Figure 2⇓.
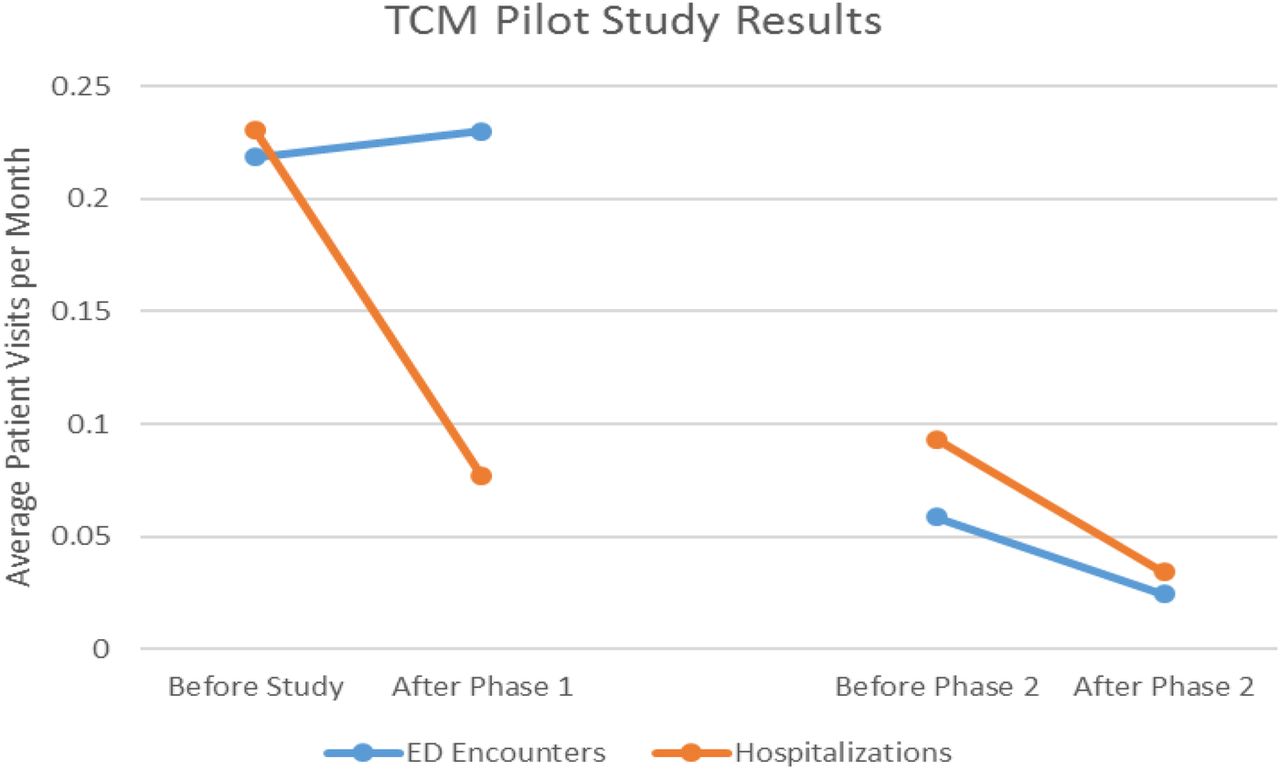
Patient visit rate to ED and hospital

{kind=link}
{kind=link}
{kind=link}
Potential financial changes
Next Steps:
Measurement of patient experience through a patient satisfaction survey which was designed 9/28/15 and will be incorporated. Areas to improve and in progress includes patient experience, engagement of the patients and families, and leveraging technology in transitions of care. Patient experience is associated positively with clinical value and patient safety. Health care organizations sustain endeavors related to improving patient experience and noted as one of the central pillars of quality in healthcare17. The engagement of the patients is imperative to reach optimum outcomes. The challenges of patient willingness, motivation, and ability to engage with the treatment plan can be due to knowledge, attitudes and beliefs. This may include health literacy, cognitive decline, confidence, health care experience, self-efficacy, and even income levels.18 Patient and family engagement was noted to be a challenge in this program especially in patients with chronic diseases. Different patient engagement models will be reviewed and the most appropriate model will be selected and implemented. Leveraging technology is essential in transitions of care. The electronic medical record (EMR) can be enhanced as a platform of communication between various providers and specialties within the healthcare system19 and in the medical community partners. A superior and adaptable technology will provide the means to electronically transmit medical information in real-time. Also, technology tools can be of use in identifying HRHC patients, automate TCM templates, and monitoring outcomes.
Case study
T.C 61 yo female with complex medical history including CHF, HTN, COPD, DM type II, chronic Hepatitis, anemia, and chronic kidney disease. She was seen in the clinic and referred to the TCM for medication and diet reinforcement especially with her uncontrolled diabetes. She lives with her daughter which is her primary support. At that time of referral, her blood sugars were high. The PCP referred the case and a family conference was organized. The family conference involved the patient, daughter, and the outpatient care team (PCP, Nurse Practitioner, Diabetes Educator/Pharmacist, and the TCM). The discussions included 1) medication, insulin specific instructions, monitoring and safety, 2) meal planning and access to food, 3) appointments with specialists, 4) transportation options, and 5) low cost or free cell phone. This conference was designed to be patient centered with specific goals in discussing complicated medical care. After the conference, the patient and daughter relayed how the family conference was beneficial and they relayed appreciation. Below were quotes from the Providers as well.
“I was very appreciative of the team approach to this patient and the steps taken to date to help the family with resources. I hope we can do much more of this in the future” Nurse Practitioner.
“The family conference was really effective at bringing the medical team together (so we are all on the same page) and helping the family troubleshoot some of the barriers they are facing at home.” Director Ambulatory Outpatient Services.
Lessons and limitations
The TCM model will be disseminated system-wide, expanding to other outlying clinics. In addition, a post hospital discharge call was developed using a modified model from this pilot program. The different interventions were simplified and translated into an automated template which is more efficient. The projected call of 10-15 patients per staff/day is expected. In Phase 1 challenges include identifying/prioritizing the variety of clients' health needs and measuring outcomes comparable to the literature. In phase 2 there was a wane in momentum hence the need to increase awareness. The amount of time in documentation and implementation posed a barrier and limiting patient contact hence the development of a template that was integrated to our EMR. The major challenge is the complexity of our patients' situation and the need for more resources. The limitations are identifying and prioritizing patients, determining the process flow of the TCM, the appropriateness of interventions, and measurement of outcomes data. Also, determining different strategies to enhance the sustainability of the project are challenging. On the other hand, the major successes include engagement of major stakeholders in supporting a change in practice.
The TCM pilot programs will be duplicated in the ambulatory care settings supported by the Public Hospital Redesign and Incentives in Medi-Cal (PRIME) program. The PRIME program has foundational delivery system to a coordinated Primary Care with varied payment/funding models20. The PRIME initial work includes performance baseline, target setting, implementation, and ongoing evaluation of quality improvement interventions. The TCM pilot projects was included to the PRIME program submission and hiring of staff is ongoing. The system-wide implementation of the TCM projects with funding may address the above limitations of this pilot program.
Conclusion
Patients face extremely complex medical systems and challenges in navigating the transitions across health care settings. There is no standardized intervention that fits all patients, it is essential to “think outside the box” and customize the needs of every patient. Hence, the need for varied Evidence Based Practices to deliver a patient centered care. Particularly challenging is the transition from hospitalization to outpatient clinical care. This intervention sought to minimize the use of the ED and hospitalizations via a multi-disciplinary approach with longitudinal clinic-based care management. The intervention was able to demonstrate a decrease in ED visits, hospitalization and a cost-savings. However, more data is required to compare results to the literature currently being structured for a system wide implementation. This model is going to be duplicated in this hospital system's other outlying clinics.
Acknowledgments
The authors want to acknowledge the following:
Marcie Levine MD
Bridget Harrison MD
Francis Capili BA
Footnotes
Declaration of interests No conflicts of interest.
Ethical approval This project is considered as Quality Improvement project by the organization's IRB.