Article Text

Abstract
Use of vitamin K antagonists creates a risk for patient health and safety. The Dutch framework “Nationwide Standard Integrated Care of Anticoagulation” propagates a shared plan and responsibility by surgeon and anesthesiologist together in the preoperative setting. In our institution, this framework had not been implemented. Therefore, a quality-improvement project was started at the Anesthesia Department to improve perioperative safety.
After exploration of barriers, multiple interventions were carried out to encourage co-workers at the preoperative screening department to take shared responsibility: distribution of prints, adjustments in electronic patient records, introduction of a protocol and education sessions. Efficacy was measured retrospectively performing a before-after study collecting perioperative data of patients using vitamin K antagonists. The primary outcome measure was the percentage of predefined safe preoperative plans. Secondary outcome measures were (1) incidence of postoperative bleeding and thrombo-embolic events within the first 24 hours after intervention and (2) necessity to preoperative correction of anticoagulation.
Before intervention 72 (29%) safe, 93 (38%) partially unsafe and 83 (33%) unsafe arrangements were made. After the intervention these numbers were 105 (80%), 23 (17%) en 4 (3%), respectively: a significant 51% increase in safe preoperative plans (P<0.001). We observed no significant difference (P=0.369) regarding bleeding and thrombo-embolic events: pre-intervention 12 (5%) cases of postoperative bleeding were documented, vs. 6 (5%) post intervention and the number of thrombo-embolic events was 5 (2%) vs. 0. Also, no significant differences concerning preoperative correction of anticoagulation were observed: 11 (4%) vs. 8 (6%) (P=0.489).
This quality improvement project demonstrates a major improvement in safer preoperative arrangements in our institution regarding vitamin K antagonists, using the described interventions. A significant effect on bleeding or thrombo-embolic events or necessity to correction of anticoagulation could not be demonstrated.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
In 2014 nearly 470 000 people in the Netherlands were treated with vitamin K antagonists (VKA) to prevent them from suffering a thrombo-embolic event.1 It is well known that the use of anticoagulation causes a risk for patient safety. The Dutch HARM study showed that VKA are responsible for drug-related, but potentially avoidable hospital admissions in 15% of cases.2 The Dutch Health Inspectorate registered 51 VKA-related adverse events from 2007 to 2009 and concluded in 2010 that there was room for optimization in communication between healthcare workers about the VKA use of patients.3 In August 2014, the second version of the framework “Nationwide Standard Integrated Care of Anticoagulation” (NSICA) was published.4 This document provides suggestions how to deliver care for patients with anticoagulants such as VKA in the perioperative phase and states a shared responsibility of surgeon and anesthetist concerning continuing, temporarily discontinuing and/or bridging these drugs in the preoperative phase.
In our academic hospital in the south-west of the Netherlands, we lacked this shared responsibility and a easily found institution-broad protocol for preoperative arrangements for patients using VKA. Patients undergoing elective surgery or intervention, for which anesthetic expertise is necessary, are referred to the Department of Preoperative Screening (POS) of the Anesthesia Department. There, the patients are screened by a daily changing team of 4 persons, coming from a pool of 35 anesthesia consultants, 74 registrars in anesthesia, and 3 Physician Assistants. The total composition of this group is variable and depends on individual career planning and training and education schedules.
In order to improve the preoperative plans regarding patients using VKA a quality improvement project was started in our institution aiming at >75% safe preoperative arrangements. Although there is a shared responsibility with the surgeons, we chose to focus on the group of the Anesthesia Department, because the group of surgeons is too large and too heterogeneous (> 14 different specialties). Moreover, the Anesthesia Department was faced with the biggest change in their work: the introduction of shared responsibility with regard to the pre-operative plan concerning VKA use.
Background
In the perioperative phase a balance should be found between the risk of bleeding and the risk of a thrombo-embolic complication.5 In the Netherlands, the guideline “antithrombotic therapy” has recently been updated.6 This guideline has partially been based upon the 9th edition of the ACCP guideline Antithrombotic Therapy and Prevention of Thrombosis.7 It provides recommendations how to deal with VKA in the preoperative phase. The risk of arterial thromboembolism is defined as high when the risk is >10% per year; for a venous thrombo-embolism it is a monthly risk of >10%. Patients at high risk of a thrombo-embolic event, such as a patient with a mechanical heart valve prosthesis in the mitral position, have to be bridged after the preoperative discontinuation of the VKA with therapeutic doses of Low Molecular Weight Heparins (LMWH) or heparin in order to minimize the risk of a thromboembolic event.6 However, this strategy has recently been questioned, because bridging with LMWH results in an increased risk of perioperative bleeding8 ,9 and the efficacy of bridging with LMWH in patients using VKA because of atrial fibrillation was doubted in the ‘BRIDGE-trial’.10
Baseline measurement
From June 1st 2015 to September 29th 2015 we retrospectively analysed the OR-programme for the pre-intervention group. All patients >18 year and using VKA planned for an elective non-thoracic operation, for which an anesthetic assistance was required, were included in this study. As primary outcome, the preoperative arrangements in the patients electronic medical record (EMR) were evaluated and classified as: ‘safe’ (green in table 2a/b; e.g. assessment by both operator and anesthetist), ‘partly unsafe’ (yellow in table 2a/b; e.g. bridging VKA only considered by anesthetist) and ‘unsafe’ (red in table 2a/b; e.g. nobody made a preoperative plan about VKA use). If the operator was aware of use of VKA and wanted to continue the VKA because of minimal bleeding risk, this was considered safe (green). As secondary outcomes we looked at: (1) incidence of postoperative bleeding or thrombo-embolic complications up to the first day after surgery and (2) need for preoperative optimization of INR by means of consultation of a hematologist, administration of vitamin K or prothrombin complex concentrates. We selected a 24 hour period after surgery, because after this period therapeutic anticoagulation medication is usually resumed and complications can no longer be attributed to the pre-operative plans. In this 4-month period, 248 patients were included and 72 (29%) safe, 93 (38%) partially unsafe and 83 (33%) unsafe preoperative plans were made.12 (5%) cases of postoperative bleeding were documented, and 5 (2%) thrombo-embolic events. In 11 patients (4%), preoperative correction of INR was necessary.
Design
Barriers may be present in a target population and might influence implementation of guidelines and innovations 11. A survey was conducted (Surveymonkey®) among the pool of anesthetic co-workers with questions about the NSICA, its joint responsibility and how to deal with it in order to better identify these possible factors. After sending a reminder, 55 (49%) responses were collected. The group found it particularly important (80%) that a protocol should be available in the EMR and that the proposed plan of the operator should be easily found in EMR. Not being motivated (15%) did not seem to be a problem, but almost 60% of the respondents did not know of the existence of the NSICA. Although it is not unambiguously shown that studies with multiple interventions are more effective than with single interventions, we chose a multicomponent intervention strategy.12 Efficacy of this improvement strategy was measured retrospectively performing a before-after study with outcome measures as described above. We did not test every single intervention, because evidence of efficacy for each intervention was available. Categorical variables were analysed using a Chi squared or Fisher exact test; continuous variables were analysed with a paired t-test. P<0.05 was considered significant.
Strategy
The multicomponent strategy consisted of: (1) distribution of educational materials, (2) adjustments in EMR, (3) develeopment of an guideline based protocol and (4) education meetings. A timeline clarifying the different steps and granting an overview of the quality improvement project can be found in figure 1. As distributing educational materials can have modest positive effects on process measures, the improvement project was started in june 2015 by putting up posters at designated places within the Anaesthesia Department in order to create awareness about NSICA and stimulate interest in shared responsibilty.13 Given the fact that concealment in the EMR of the proposed preoperative plan of the operator seemed to be a major barrier, adjustments were made in EMR: (1) removing the “use of anticoagulative medication unknown” option in EMR on the OR-application of the operator (2) creating a more clearly defined plan regarding continuing, temporarily discontinue and requirement of bridging therapy (3) visualisation of the proposed plan in the anesthetic part of the OR-application, so the plan could be adopted or adapted as necessary. As decision support can lead to improved clinical care, we designed a preoperative protocol containing decision rules whether VKA should be bridged.14 This protocol was discussed within education meetings and optimised on the basis of given feedback, thereby improving it through a PDSA-cycle. Finally, it was made accessible in EMR for both the operator and the anesthetist. Whether or not combined with other interventions, education meetings contribute to improvement of professional practice and outcomes in health care.15 The meetings (45-60 minutes) were scheduled in a way the majority of the target population of the Anesthesia Department was reached (see figure 1). Three meetings were given for all doctors and PA's present during morning roll call. In addition to information transfer to the group, these moments were also used to brainstorm on optimal implementation of the shared responsibility. Also, adaptations were made to the preoperative protocol concerning VKA use, based upon the input of the people attending the meeting. In this way, we also tried to change any negative attitudes regarding the process of change. The first and last session were filmed, so absent doctors and PA's were also able to learn about the process via an easy accessible weblink. Three meetings were also given during regular education for the registrars.

{kind=link}
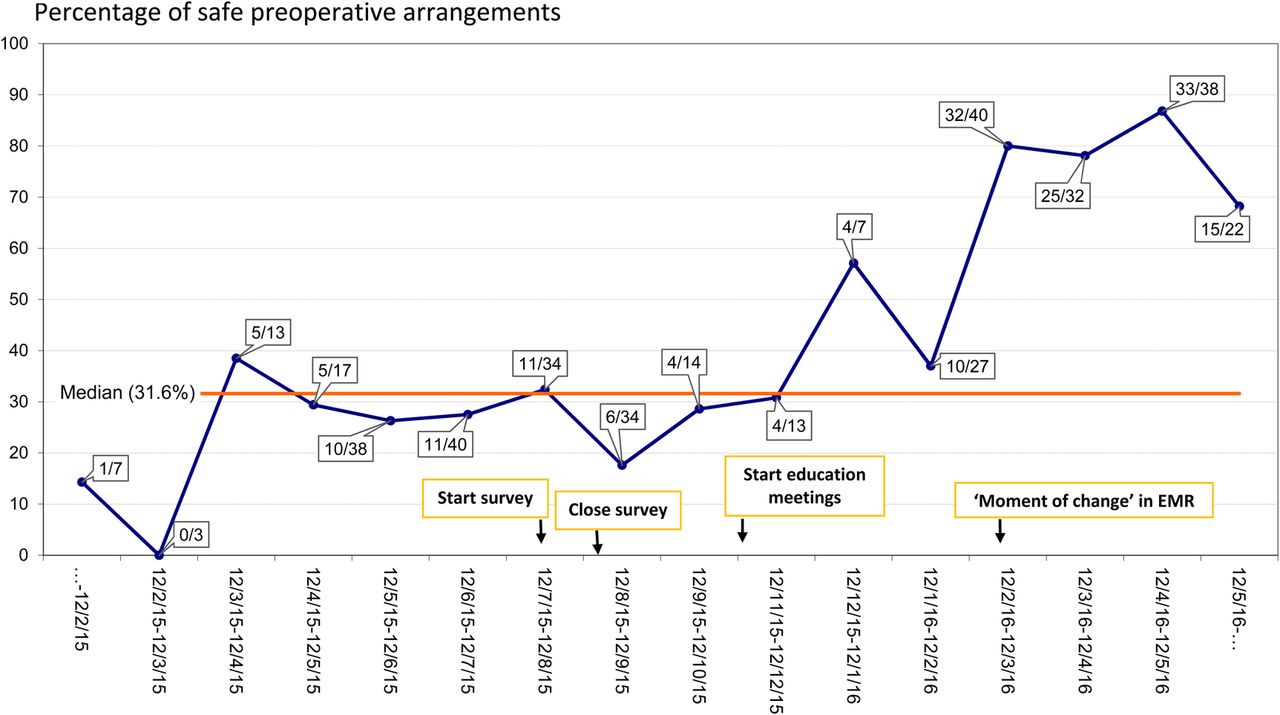
Run-chart describing the percentage of safe preoperative arrangements as part of the total arrangements per monthly period. The absolute numbers (‘x/y’) are also visualised. Too few runs across the median and the shift (6 data points above the median since 12/12/15) indicate change has occured.
Attendances were tracked to see which part of the group was effectively reached. Content of the meetings was based on the previously found barriers: existence of NSICA with the resulting joint responsibility of operator and anaesthetist regarding the preoperative agreements concerning use of VKA, current practice and examples of unsafe preoperative arrangements, upcoming changes in EMR and development of a easy accessible protocol.
The educational sessions were organised in the period 29 October 2015 - 1 February 2016. Finally, 26 anesthetists (74%), 3 PA's (100%) and 41 registrars (55%) attended 1 or more education meetings. 30 of the 33 registrars that were not reached were working in another hospital or at the ICU during the project. The moment at which the changes in the EMR were made available (12 February 2016) was chosen as time of change. Prior to this date, an email was sent to the target population to announce the new approach. It also included the protocol and the presentation held on the last joint education meeting, together with the video-link. All surgeons were officially informed via the ‘Council of OR-users’. At the end of the project, a survey within the Anesthesia Department was conducted to evaluate the project and all the used strategies, so we knew which parts of the project we should use in a future project and which parts not.
Results
The characteristics of the patient population in the pre- and post-intervention group are shown in table 1. Patients in the post-intervention group (n=132) were significantly older, but other characteristics showed no significant differences. As can be seen in table 2a and 2b, the percentage safely made, guideline based, pre-operative arrangements regarding VKA use (green fields) increased from 29% (72/248) to 80% (105/132) (P<0.0001), while the partially unsafe (yellow) and unsafe (red) arrangements decreased from 38% (93/248) to 17% (23/132) and 33% (83/248) to 3% 4/132), respectively. As results of a before-after studies can't be used to visualise improvement in time, the percentage safely made preoperative arrangements as a part of the total preoperative plans regarding VKA use per month was put in a run-chart depicted in figure 1. The improvement seems to start when the education meetings started and is eventually confirmed by, as described by Perla et al.16: (1) the fact that there are to few runs across the median (3 instead of 4) and the presence of a shift at the end of the run-chart. The secondary outcomes were collected in table 3 and compared with the pre-intervention data. Post-intervention, there were 6 (5%) bleeding events registered and no thrombo-embolic occurred. In 8 (6%) cases, preoperative correction of anticoagulation was necessary. All secondary outcomes did not differ significantly from baseline measurements.
Patient characteristics of the pre-intervention, post-intervention and the total group of patients
The number of observed safe (green), partially unsafe (yellow) and unsafe (red) preoperative arrangements regarding use of VKA in the pre- intervention group. An arrangement with dual responsibility was considered safe; when a surgeon proposed to continu the VKA (because of low bleeding risk) this was considered safe. If only one of the two specialists made a plan, or plans were different from eachother, this was considered partially unsafe.
The number of observed safe (green), partially unsafe (yellow) and unsafe (red) preoperative arrangements regarding use of VKA in the post- intervention group. An arrangement with dual responsibility was considered safe; when a surgeon proposed to continu the VKA (because of low bleeding risk) this was considered safe. If only one of the two specialists made a plan, or plans were different from eachother, this was considered partially unsafe.
Secondary outcome measures in the pre- and post-intervention group
Lessons and limitations
The quality improvement project ran from 1 June 2015 to 1 July 2016 Initially, we expected that the changes in the EMR could be implemented in December 2015, but this was postponed until 12 February 2016, because the Anticoagulant Committee of our hospital considered it important that all upcoming changes in EMR first had to be communicated more profoundly with stakeholders in order to obtain sufficient support for the procedural changes. Based on given feedback, in April 2016 standard medication orders were created in collaboration with the Pharmacy Department to make prescribing bridging therapy at the POS less time consuming. A survey conducted in May 2016 to evaluate the project was completed by 25 (22%) persons. Although 17 responders had been able to see the posters, only 9 persons noticed them, of which 5 declared that the posters did have any effect (e.g. were stimulated to learn more about VKA). 19 responders attended educational meeting(s) and believed this was useful, though only 2 persons had used the opportunity to look back to the presentation via the web link. The other interventions were considered to be positive contributing according to 80% of the respondents. 21 out of 25 were using the protocol and 24 people felt that the subject is more appropriate addressed than before the intervention. Although the run chart shows a shift, indicating a moment of change 16, we do not know for certain if this improvements will be sustained. The sustainability of the intervention, in our opinion, particularly depends on continuing the education meetings in a structured manner. Within the Anesthesia Department the subject has to be addressed at the existing educational structures on a regularly basis. It is also the intention to randomly check how the shared responsibility is performed and, if necessary, individual feedback will be given and maybe some aspects may be optimised. Hopefully, by using this kind of PDCA cycle, the initiated change will be permanent. This will particularly be a challenge, because our hospital will get an new EMR in June 2017. Therefore, it is of high importance that the results of this study are also perpetuated in this new digital working environment. In order to achieve this, members of the anticoagulation committee of our hospital are currently involved in the development of this new EMR, trying to perpetuate a continuous level of patient safety regarding VKA use.
Within the Anesthesia Department this kind of quality improvement can also be used for implementation of other pre- and perioperative topics like perioperative regulation of diabetes or perioperative corticosteroid-‘stress’ scheme. In the future, the possibility of including other groups of professionals like surgeons in a quality improvement project has to be considered, because results might even more improve.
As this quality improvement project's main objective was to effectuate a change within a group of professionals, we chose a process measure as primary outcome. However, outcome measures are more of use describing effects on mortality and morbidity and therefore we chose them as secondary outcome measures.17 Safe pre-operative agreements concerning VKA use could result in fewer bleeding or thrombo-embolic complications and less need for correction of anticoagulation just before surgery. However, these pre-operative arrangements are just a part of the chain in the peri-operative process for this patient group. Safe arrangements can be made, but are ineffective and inefficient when, for example, patient compliance is inadequate. This was not evaluated in this project, this study was probably under-powered for the secondary outcomes. Outcome bias might exist, because of the, for ethical reasons, retrospective character of this study. We were not able to track patients that were removed from the OR-program due to problems with anticoagulation. The interval of 24 hours after surgery is arbitrary, but justifiable because after this time-frame therapeutic anticoagulation is usually reinforced, possibly affecting the secondary outcome measures. The percentages of secondary bleeding and thromboembolic complications in our institution are consistent with what is known from the literature on postoperative complications regarding VKA use. (9, 18), but may be higher at longer post-operative follow up measurements. In the post-intervention group patients were older, but this fact unlikely will have contributed to the secondary outcomes.
Conclusion
Because use of VKA is a known threat to patient safety, it is necessary to make safe preoperative arrangements regarding this VKA. (1-5) Shared responsibility of surgeon and anesthetist regarding this plan should result in safer preoperative arrangements.
This quality improvement study, executed at the Anesthesia Department of our institution, shows a major improvement in safe, guideline based, preoperative plans for patients using VKA, although there might be concern about sustainability in the future. Education meetings, adjustments in the EMR and the presence of a protocol contributed to this improvement. A clinically significant effect on bleeding or thrombo-embolic events could not be assessed. Neither a significant effect on the need for pre-operative correction of anticoagulation was determined.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval The Daily Board of the Medical Ethics Committee of our institution had reviewed the research protocol and concluded that the rules laid down in the Medical Research Involving Human Subjects Act did not apply to this project and therefore waived ethical approval.