Article Text

Abstract
Dementia is a common condition, and people with dementia occupy around 25% of hospital beds. Commissioning for Quality and Innovation (CQUIN) is an NHS payment framework that links part of English healthcare providers' income to quality improvement. The dementia CQUIN goals are designed to encourage the recognition of dementia in hospital. The Royal Surrey County Hospital, Guildford, introduced new procedures to meet the dementia CQUIN targets. Adherence to the changes was a problem. This project aimed to improve hospital's implementation strategy. At baseline, completion rates for dementia CQUIN assessments were just 27%. Interventions were informed by semi-structured interviews with junior doctors and dementia leads in neighbouring trusts. Progress was measured by regular audits and interventions were made over several months. Changes suggested by junior doctors and nurses proved very effective, and involving the multidisciplinary team produced the most significant improvement. Gradual progress was made until we achieved and maintained 90% completion for dementia assessments. In conclusion, we made changes to working practices to achieve the CQUIN targets and promoted quality care for older adults. Our experience highlighted the importance of involving multidisciplinary frontline staff in the design of service changes.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Dementias are common neurodegenerative conditions affecting older people. People with dementia currently occupy 25% of hospital beds.1 They remain in hospital for significantly longer than people without dementia.1 Commissioning for Quality and Innovation (CQUIN) is an NHS payment framework launched by the Department of Health in 2009. It links part of English healthcare providers' income to specific quality improvement goals.2 The dementia CQUIN, introduced for in 2012/13, was designed to encourage the recognition of dementia in hospital. The framework is also intended to promote appropriate follow-up for people with dementia after discharge from hospital.3 The remuneration for the dementia CQUIN is significant. It is an additional 2.5% of outturn value of a Trust's contract or 0.125% of the actual contract value, provided all of the goals are attained.3
The Royal Surrey County Hospital NHS Foundation Trust is based in Guildford. It provides district general hospital services to a population of 330,000 people in Guildford and the surrounding area. It has 520 inpatient beds and 14 operating theatres, and employs 2,800 staff. Each year, the hospital sees approximately 336,000 outpatients, admits 90,000 patients and sees 73,000 patients in Accident and Emergency.4 The trust introduced new procedures to meet the CQUIN targets. However, adherence to the changes was a problem. This project aimed to improve hospital's implementation strategy, standardising dementia care and gaining additional revenue.
Our SMART goals were as follows:
Specific target – to assess >90% of older adult inpatients in accordance with CQUIN criteria
Measurable indicators of progress – results from audit of medical notes
Assigned tasks – Junior doctors, with support from the Clinical Audit Department, the Clinical Lead for Dementia and the Dementia Nurse Specialist
Realistic ambition – The hospital was willing to provide significant resources from the Clinical Audit Department to implement the CQUIN, therefore the target was realistic.
Time-bound – From the beginning of this project, the hospital had almost a year before the CQUIN took effect.
Background
Since the introduction of dementia CQUIN, hospital trusts in England have gathered specific data on all patients admitted as an emergency aged 75 years or older. The hospital must assess 90% of older patients to gain the additional money.
The CQUIN targets, known as indicators, are as follows:3
Indicator 1: Dementia case finding
The following question must be asked of all patients aged 75 and above within 72 hours of admission to hospital, excluding day cases, transfers, elective admissions and patients with a length of stay of less than 72 hours.
“Has the person been more forgetful in the last 12 months to the extent that it has significantly affected their daily life?”
Indicator 2: Diagnostic assessment for dementia
Those who scored positively on the question must be assessed for delirium and dementia, including relevant investigations.
Indicator 3: Referral for specialist diagnosis
If the outcome of the assessment suggests dementia or inconclusive, appropriate follow-up should be arranged. This could include feedback to the GP or referral to specialist services.
King's College Hospital published their experience of delivering the venous thromboembolism CQUIN goal.5 Staff engagement was crucial, and embedding change took several months. University Hospitals of Leicester NHS Trust reported introducing the dementia CQUIN.6 Interventions targeted and significantly improved adherence to the new practice.
The Royal Surrey County Hospital produced a two-sided ‘Dementia CQUIN form’ to ensure that relevant assessments were clearly documented. This was completed by the clerking junior doctor and filed with admission notes. Completion was electronically recorded using a tick-box on the electronic discharge summary (confusion/dementia assessment completed: yes/no). If the user said no, a small free-text space appeared to record reasons why not. Junior doctors were emailed about the changes, and presentations were made at Journal Club and junior doctors’ teaching sessions.
Baseline measurement
Two baseline snapshot audits were conducted in April and May 2012. These assessed adherence to the paper dementia CQUIN form. The April audit sampled inpatient case notes from five general medical wards with approximately 24 patients on each ward. The May audit included all inpatient wards except paediatrics: the number of patients per ward ranged from 8 to 25.
All patients aged 75 years or older were included. Patients were excluded is they had been an elective admission or admitted before the CQUIN came into effect, in accordance with the CQUIN guidelines. The audit counted:
the number of correctly completed CQUIN forms in medical notes
the number of notes that were not available
the number excluded according to the CQUIN guidelines
Data was analysed using Microsoft Excel.
April 2012 results (Supplementary chart 1):
A third of case notes were unavailable at the time of the audit. Across the five wards audited, 27% of those over 75 had a completed Dementia CQUIN form in the notes.
May 2012 results (Supplementary chart 2):
The May audit was conducted later in the day to increase the number of notes available: 4% of notes were unavailable to audit or were excluded. Among the wards included in the April audit, completion rates had increased from 27% to 38%. However, the average across all wards was unchanged at 27%. There was considerable variation between wards.
supplementary data
Design
A series of interventions were designed and tested over 18-28 months. The Clinical Lead for Dementia, the Dementia Nurse Specialist and a junior doctor made the interventions.
We explored doctors’ views using semi-structured interviews. We also consulted dementia care leads from neighbouring NHS Trusts using semi-structured interviews. Suggestions for improvement chiefly came from the junior doctors involved. Audits were conducted by the trust audit department in collaboration with junior doctors. They included all inpatient wards except paediatrics. They were conducted monthly during the first 12 months and quarterly thereafter. Our target was to assess 90% of older patients, as specified by the CQUIN criteria.
Strategy
Our strategy developed continuously. Numerous small interventions were made in response to audit and suggestions from colleagues. Here, we present these in three improvement cycles.
Improvement Cycle 1, April 2012 - August 2012:
Emails were sent to all medical staff introducing the CQUIN. Presentations were made by senior clinicians at Journal Club, doctors’ teaching sessions and consultant meetings. Results of monthly data collection after this did not show a significant improvement in recording of CQUIN information. As the emails were not felt to be helpful, this strategy was dropped. We explored junior doctors’ views of the dementia CQUIN in semi-structured interviews. A number of people raised problems with the paper CQUIN form: it was long, and much of the information was repeated elsewhere in the notes. Themes included opposition to targets with financial incentives, the burden of paperwork, and concern that they were being asked to diagnose dementia. Comments included:
“It's just another tick box exercise.”
“I think the hospital should opt of it. It gets in the way of clinical work.”
“Dementia assessments shouldn't be part of an acute admission. We don't have time.”
“If it was about good patient care it would be different.”
Interviews with clinical leads in other organisations showed a range a different strategies to deal with the same issues. Some trusts had junior doctors and other healthcare staff involved in designing changes. The audit and semi-structured interview results were presented by junior doctors at the trust audit day, during which the importance of holistic assessment of older adults was emphasised.
Improvement Cycle 2, September 2012 – January 2013:
The paper form was simplified to minimise repetition and fit it onto one A4 page: the word ‘CQUIN’ was removed. At the suggestion of ward nurses, the dementia form was included in the nurses’ checklist of items to be completed before a patient could transfer between wards. The changes were communicated to all nursing staff team through presentations and emails. This prompted the nurses to help the junior doctors by checking all the assessments were completed. The results of monthly data collection improved significantly after this, attaining the 90% required for the CQUIN. The paper form was further simplified and the electronic discharge summary was amended on the advice of junior doctors.
Improvement Cycle 3, February 2013 – August 2013:
Information about the CQUIN, written by junior doctors, was included in induction packs. Junior doctors suggested and designed a new clerking proforma which incorporated information on the CQUIN form, making it redundant. This was successfully piloted in geriatric medicine. It reduced the burden of paper forms and facilitated audit. It also made clerking notes clearer. Results of data collection showed further improvement.
Improvement Cycle 4, September 2013 – August 2014:
The clerking proforma was developed and adopted for all medical admissions. A simplified version of the dementia CQUIN form continued for surgical admissions. The nursing checklist intervention was continued as it was felt to be highly successful. Results for quarterly data audits show adherence remains above the threshold of 90%.
Results
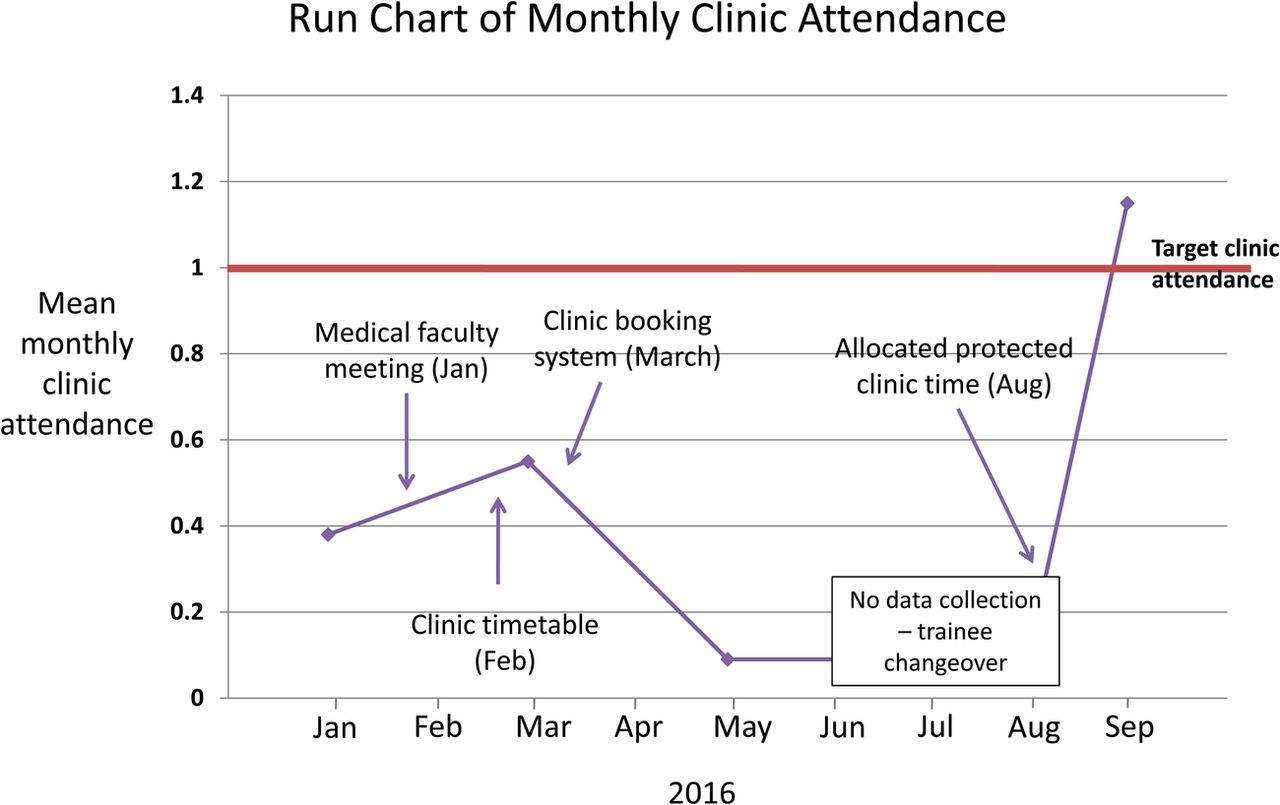
Data was collected monthly for the first year and quarterly thereafter. The exact number of notes audited varied from month to month, depending on bed occupancy, but averaged around 280. The results were analysed by the audit department and by junior doctors and they were shared with staff through presentations. The audit measured our progress in developing a strategy to deliver the dementia CQUIN goals. The uptake of interventions varied considerably by ward: elderly care wards showed the fastest uptake and surgical wards showed the slowest progress. In the early stages of the project, some surgical wards had no CQUIN data recorded for successive months. Charts were produced which showed the progress achieved (figure 1).
The number of patients having delirium and dementia assessments, in accordance with the CQUIN, increased slowly from 27% to over >90%. We demonstrated that our interventions produced sustained improvement: quarterly audits since then demonstrate that changes have been embedded in the working practice of the hospital. This promotes quality of care older adults and also promotes the financial security of the Trust.

{kind=link}
Lessons and limitations
Our interventions were simple, but they required communication and negotiation with people at all levels in the organisation. We found that ‘bottom up’ approaches to change management were particularly important. These encourage frontline staff (in this case, junior doctors and nurses) to be actively involved in managing change. The greatest improvement in the data occurred after the nurses were prompted to ensure assessments were completed. This highlighted in importance of multi-disciplinary team working for delivering patient care. It also ensured the sustainability of the changes once the junior doctors involved had moved.
If we were repeat the project, we would include ward nurses earlier in the development of interventions. We did not collect data for other patient outcomes, such as length of stay, which is a limitation: it might have allowed us to demonstrate the benefits to patients from additional assessments. We could have improved the methodology used in this project. More than one change was made in each audit cycle, therefore it was not possible to be certain exactly what was responsible for the improvement. All changes were rolled out across the whole hospital, rather than piloting in a small area first: this could have resulted in wasted resources. Using the Plan, Do, Study, Act (PDSA) would avoid these problems. We did not include measures to reduce bias, such as inter-rater reliability between auditors, or do statistical tests, which would have allowed us to be confident that apparent differences were not due to chance. Strengths of this project include the long study period and continuity within the team making interventions. A further strength is the wide generalisability of the findings, which are relevant to all acute hospitals in England.
Conclusion
This project aimed to improve the implementation of the dementia CQUIN at the Royal Surrey County Hospital for the benefit of patients and the hospital. We involved junior doctors, nurses and clinical leaders to make interventions. These were ultimately successful, but it took several months before the CQUIN goals were achieved and sustained. Our experience is similar to that of King's College Hospital5 and the University Hospitals of Leicester NHS Trust.6
This demonstrates the importance of evaluating the effects of each intervention and amending the strategy in response. The approach taken here could be generalised to other acute hospital settings and applied to other CQUIN goals. Auditing continues to ensure our success is maintained. In future, paper medical records and electronic systems must be combined to produce paperless electronic patient notes. It is vitally important that frontline staff are involved in the design of future healthcare data systems.
Acknowledgments
Dr Hugo Powell, Clinical Lead for Dementia and mentor for this project,
Ms Faye Wright, Dementia Specialist Nurse,
All other staff at the Royal Surrey County Hospital.
Footnotes
Declaration of interests Nothing to declare
Ethical approval According to the policy activities that constitute research at the Royal Surrey County Hospital NHS Foundation Trust, this work met criteria for operational improvement activities exempt from ethics review. Explanation: the work was intended to improve local adherence to national care standards, not provide generalizable knowledge in a field of enquiry. The project was registered as an audit with the Trust Quality Improvement Department.