Article Text

Abstract
Peripheral blood stem cell (PBSC) collection from donors through apheresis has become the main source of stem cells for hematopoietic stem cell transplantation. This procedure requires a high blood flow venous access. A peripheral venous catheter (PVC), compared to a central venous catheter (CVC), is considered to provide safer venous access. However, initially at our institution, King Abdul-Aziz Medical City - Riyadh, a CVC was frequently used (72%). A quality improvement multidisciplinary team has been formed to conduct a systematic quality performance analysis to evaluate the current process of collecting donor PBSCs with the aim to reduce CVC use to less than the international benchmark (20%). A quality improvement methodology, rapid cycles of plan-do-study-act (PDSA), was used to test a set of initiatives. An Intravenous (IV) team assessed the donor's venous access and inserted an appropriate PVC when feasible. This project ran over 16 months with 42 adult donors undergoing PBSC collection. During the first PDSA cycle, 1 CVC was inserted for every 4 donors. In the second PDSA cycle, 1 CVC was inserted for every 8 apheresis donations. In the third PDSA cycle, no CVC was used for 30 apheresis donations. The targeted stem cell dose was collected successfully in one apheresis session in all donors assigned for PVC access with no complications. A significant reduction of CVC use from 72% to 0% was achieved. This quality improvement project demonstrated that a successful apheresis procedure can be achieved easily and safely in the majority of PBSC donors preventing the potential adverse events associated with CVCs. The interdisciplinary collaboration between the IV team, apheresis and clinical hematology teams was paramount to optimize the safe care of donors.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Peripheral Blood Stem Cell (PBSC) collection from donors by leukoapheresis has become the main source of stem cells.1 ,3 Leukoapheresis is a procedure in which peripheral blood passes from the donor through venous access to the apheresis machine which separates the stem cells from the other types of cells and returns the remaining blood contents to the donor.3 The procedure takes approximately four hours and requires high blood flow venous access, contributing to the selection of large pore venous access devises such as central lines. However, using a peripheral venous catheter (PVC) for PBSC collection is considered to be a safer option compared to a central venous catheter (CVC) with the risk of serious adverse events. PBSC collection can be done as an outpatient procedure however if a CVC is required, donors are admitted for the procedure. Thus, reducing CVC use for PBSC collection decreases the risk of adverse events associated with CVC, decreases the admission rate, and lower the cost of the procedure. At our institution, King Abdul-Aziz Medical City – Riyadh (KAMC-R), the use of a CVC was high (72%) compared to the international benchmark of less than 20% 1. Possible reasons were the inability of apheresis nurses to insert a large bore PVC in the majority of stem cells donors and the perception among health care workers that CVC access is more secure and generates steady flow rates.
Background
Hematopoietic stem cell transplantation (HSCT) is a therapeutic option for many malignant and nonmalignant diseases. Around 50,000 HSCT procedures are performed globally every year. Approximately half of these are allogeneic, where stem cells are collected from related or unrelated healthy volunteers either peripherally or through bone marrow harvest. Voluntary donation from related or unrelated donors of bone marrow (BM) or PBSC for HSCT is a well-established and accepted altruistic act, performed by numerous centers all over the world every year. Using CVC access for healthy donors carries inherent risks which could be avoided. The international rate for CVC usage to collect PBSCs collection is around 20% as reported by the International Bone Marrow Transplant Registry (IBMTR) and European Blood and Marrow Transplant (EBMT) databases.1 ,4
The adult stem cell transplant program at KAMC-R was launched in 2010 as part of the hematology section, sharing the same unit and resources. The program aimed to transplant stem cells in patients diagnosed with malignant and non-malignant diseases. At KAMC-R, stem cell donors usually are volunteer siblings or unrelated donors from the Saudi and international stem cell registries.
The PBSC collection process at KAMC-R used to be performed by the apheresis team consisting mainly of nurses. They were responsible of assessing the donor's venous access status and inserting a PVC when feasible. The IV team, however, is part of the anesthesia department and they are more skilled in inserting a PVC. A CVC is only inserted by a medical team as an inpatient procedure.
In general, a targeted stem cell dose of 2-7 million stem cells per kilogram of the recipient's body weight from adult donors is achieved in one apheresis session from healthy adult donor. If not, a second session is done the following day. Requiring a second session depends on multiple factors including the donor's weight, number of peripheral circulating stem cells, and other factors. A CVC is usually a requirement if more than one session of apheresis is needed.
Baseline measurement
Retrospective data analysis revealed that the majority of venous access devices (72%; 36 of 50) used for PBSCs collection from the adult donors was a CVC (Table 1). Fifty PBSCs collection procedures from adult donors have been performed since launching the program until the date of data analysis on 27th November 2014 (Table 1). All donors needing a CVC were admitted to the hospital for at least two days and the CVC was removed upon completion of the procedure. The site of CVC insertion was a femoral line and no major complications, thrombosis, infection or bleeding, were observed.
Baseline data of PVC and CVC usage (frequency and percentage)
Design
A multidisciplinary quality improvement (QI) team was constituted to conduct a systematic situational analysis and evaluate the processes of collecting donor's PBSCs to reduce CVC use to less than 20%. The team consisted of a hematologist, a QI specialist, an apheresis nurse, an IV specialist, a representative from interventional radiology (IR), a HSCT nurse coordinator, and a representative from the stem cell laboratory. After conducting a cause-effect analysis and generating a fishbone diagram, it became clear that the underlying cause of failing to insert a PVC was the proficiency of the aphaeresis team to assess and insert a PVC line. A decision was taken that the IV team will perform the assessment and insertion of the PVC in the donors. As a contingency plan in case of failure of insertion or collapse of a PVC, the donor would be moved directly to the IR department for CVC insertion. The IV team has been trained as a part of the Anesthesia Department and are proficient and experienced in inserting large bore PVC.
Strategy
A quality improvement methodology, rapid cycles of improvement method plan-do-study-act (PDSA), was used to test the efficacy of the interventions. Three PDSA cycles were implemented.
PDSA Cycle 1: The lesson learned from the baseline measurement and cause-effect analysis was that the apheresis team was not proficient in inserting appropriate PVCs in the PBSC donors. Based on that, and after discussion with our multidisciplinary team, the IV team was assigned to replace the apheresis team in assessing the venous access status of donors and inserting PVCs when feasible. The first PDSA cycle aimed to decrease the usage of CVC to less than 50%. This cycle was tested for one month (December 2014). Donors were booked for CVC insertion in the IR department on the day of the procedure as a contingency plan for PVC insertion failure or PVC collapse. Four donors was assessed by the IV team during this cycle and PVC was recommended for all. The stem cell collection using PVCs was successful in three donors with one donor needing subsequent CVC insertion due to low blood flow from PVC (Table 2). The team decided that increasing the peripheral cannula size would improve the blood flow and reduce the need of CVC insertion leading to PDSA cycle 2.
PVC and CVC usage in frequency and percentage during the PDSA cycles
PDSA cycle 2: The second cycle started immediately after first cycle lasting three months. Based on the lessons learned from the first PDSA cycle, the team suggested using a larger bore PVC to improve the blood flow. The second PDSA cycle aimed to decrease the usage of CVC to less than 25%. The IV team used a larger bore size PVC (gauge 14-16 instead of 18) to improve the blood flow to the machine. Donors were booked for CVC insertion in the IR department in case of procedure failure. In PDSA cycle 2, 1 CVC was inserted of 8 stem cell collections due to PVC collapse (Table 2). Reducing the percentage of CVC usage to 12.5% was promising and the team decided that this could be improved if metallic cannula were used in case of PVC collapse. The team gained more confidence and decided to perform a third PDSA cycle on a larger scale with changing the type of peripheral cannula if the initial PVC collapsed.
PDSA Cycle 3: From the second PDSA cycle, we learned that the PVCs could collapse due to high blood demand from the machine and a decision was taken to use a metallic peripheral cannula as second option if the initial PVC collapsed. The third PDSA cycle started immediately after the second cycle and lasted for 12 months aiming to decrease the usage of CVC to less than the international benchmark of 20%. During this cycle, the IV team used metallic peripheral cannula as planned. At the end of this cycle, no CVC was inserted in 30 peripheral stem cell donations (0%) (Table 2). The stem cells of all PBSC donors were collected successfully and safely utilizing PVCs. Based on these results, we decided to implement a sustainability plan to maintain the improved result by standardizing the practice and revising the departmental policy and procedures.
Results
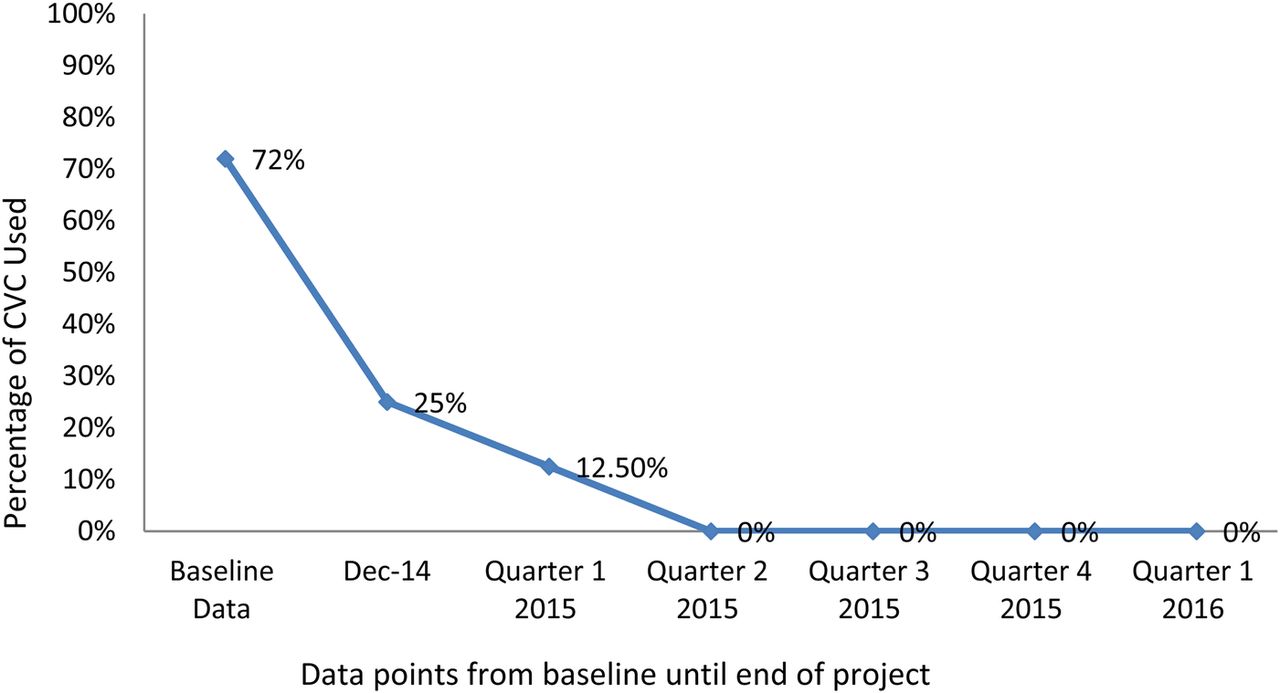
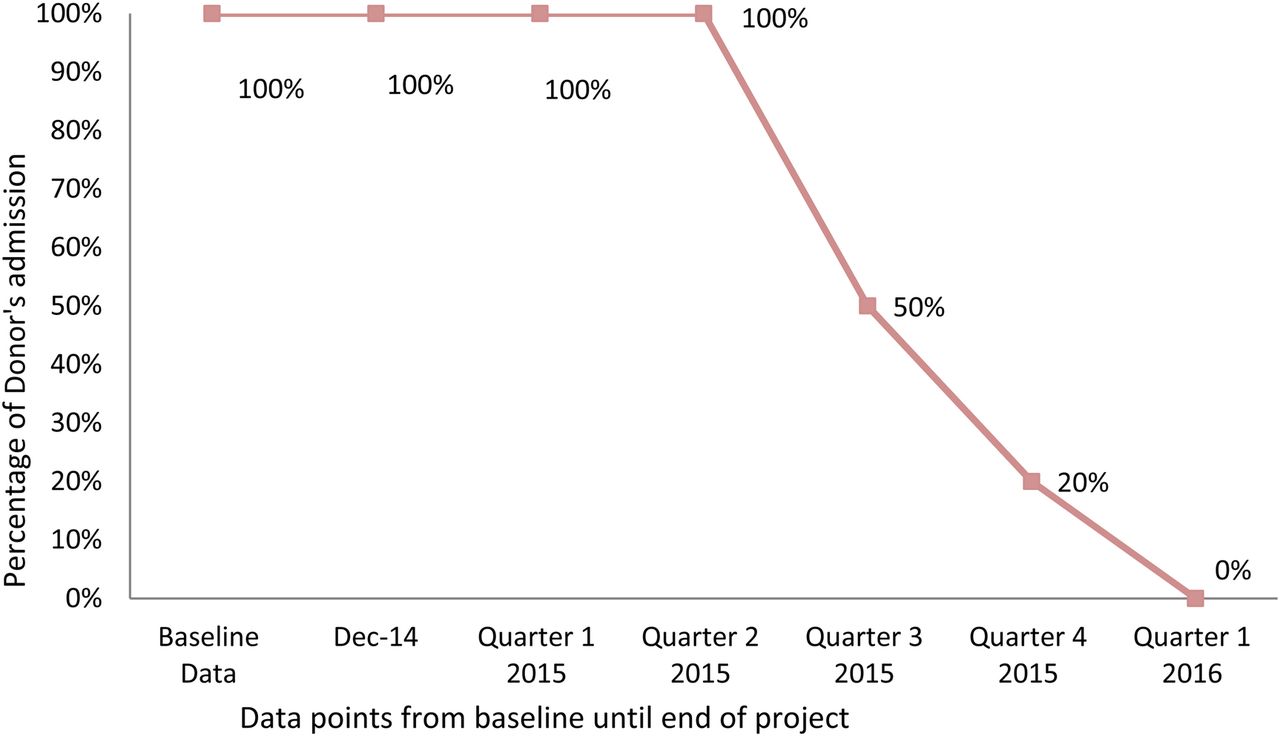
The objectives of this QI project were met through reducing the usage of CVC for donor's PBSC collection from 72% to 0% (Graph 1) and the improvement was sustained for a year. In addition, the targeted stem cell dose was achieved in one apheresis session with all donors and there were no major complications such as phlebitis or hematoma. Consequently, the interventions reduced the admission of donors from 100 to 0% (Graph 2) thus reducing potential risks and health care costs from PBSC collections.

Percentage of CVC used throughout the QI project

{kind=link}
{kind=link}
Percentage of Donor's Admission throughout the QI project
To maintain the achieved result of less than 20% CVC for PBSCs collection, we shared our results and sustainability plan with the leadership of the apheresis unit, IV team, and stem cell transplantation program. Guidelines were developed and shared with all the involved parties to standardize the process. Ongoing monitoring of data will continue for one year followed by random evaluation for two donors every three months. If any variation is noticed, the team will meet to investigate the causes and take appropriate actions. The result of this project were also disseminated through internal memoranda, staff education, and written guidelines. The achievements of the project were also spread through multiple posters and presentations such as “MNGHA Patient Safety Forum”, “Saudi Society of Blood and Bone Marrow Transplant meeting”, “KAMC-R Oncology Research Day” and the Nursing day celebration.
Lessons and limitations
The most important lesson is that simple interventions can significantly impact PBSC donor safety. Moreover, using a multidisciplinary team to conduct a systematic situational analysis assisted in defining the problem and lead to a set of improvement interventions. A major barrier to implement the changes came from the aphaeresis team in shifting their task of assessing and inserting the PVCs to the IV team. This was overcome by emphasizing the benefits and need for changes highlighting the safety of the donors.
As far as the sampling error is concerned, there was no bias of selecting the donors as a census sample with all adult donors were included since the start of the project. The stem cells of 42 donors have been collected during the three PDSA cycles. We are confident the project interventions are practical and could be replicated with any HSCT project. However, it might be advisable to replicate this project in a larger study population in different settings. The sustainability of the project impact is clear and promising and the hospital management showed interest in the empirical evidence generated during the project, moving from testing to implementation making this evidenced based safe practice part of the daily operation of the HSCT project.
Conclusion
This project highlighted the value of the science of quality improvement to constantly improve delivery of safer care. Introducing interventions has significantly reduced the use of CVCs achieving 0% CVC use for PBSC collection from adult donors compared to a baseline of 72% and an international benchmark of 20%. The outcome demonstrates that a successful apheresis procedure can be achieved easily and safely in the majority of PBSC donors through PVC usage, minimizing the potential adverse events associated with CVC, increasing donor safety. PBSC collection using PVCs can be done safely in an outpatient setting eliminating the cost related to the CVC insertion and hospital admission. An important part of our improvement journey was to sustain our improvement efforts through multiple steps. The positive outcome encouraged the team to disseminate the findings to other transplant centers.
Acknowledgments
Director Clinical Nursing: Andrea Doherty
SCT Nurse Coordinators: Eman AlAnizi , Isam Almahasneh, and Inaam Shehabeddine
Aphaeresis Team
Footnotes
Declaration of interests Nothing to declare.
Ethical approval The work was primarily intended to improve care of stem cell donors, and not to provide generalizable knowledge in a field of inquiry, therefore, it was exempted from ethical review and was considered an operational improvement activity.