Article Text

Abstract
Cancer patients are frequently admitted to hospital for many reasons. During their hospitalization they are handled by different physicians and other care providers. Maintaining good communication among physicians is essential to assure patient safety and the delivery of quality patient care. Several incidents of miscommunication issues have been reported due to lack of a standardized communication tool for patients' hand over among physicians at our oncology department. Hence, this improvement project aims at assessing the impact of using a standardized communication tool on improving patients' hand over and quality of patient care. A quality improvement team has been formed to address the issue of cancer patients' hand over. We adopted specific hand over tool to be used by physicians. This tool was developed based on well-known and validated communication tool called ISBAR - Identify, Situation, Background, Assessment and Recommendation, which contains pertinent information about the patient's condition. The form should be shared at a specific point in time during the handover process. We monitored the compliance of physician's with this tool over 16 weeks embedded by four ‘purposive’ and ‘sequential’ Plan-Do-Study-Act (PDSA) cycles; where each PDSA cycle was developed based on the challenges faced and lessons learned in each step and the result of the previous PDSA cycle. Physicians compliance rate of using the tool had improved significantly from 45% (baseline) to 100% after the fourth PDSA cycle. Other process measure was measuring acknowledgment of hand over receipt email at two checkpoints at 8:00 – 9:00 a.m. and 4:00 – 5:00 p.m. The project showed that using a standardized handover form as a daily communication method between physicians is a useful idea and feasible to improve cancer patients handover with positive impact on many aspects of healthcare process and outcomes.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Cancer patients require frequent hospitalization for multiple reasons related to the nature of the disease, complexity of treatment and the wide range of potential adverse events and complications. During their admission, they are handled by multiple physicians. Thus, maintaining good communication among physicians in the team is an important issue to be monitored and improved. We found a miscommunication issue between the on call physicians and the rest of team. This problem was manifested by the noticeable increasing number of unnecessary phone calls between physicians after working hours, which considered a source of dissatisfaction for the physicians, and more importantly this miscommunication may compromise the level of quality of care provided to our patients. Among the possible identified causes of this problem was the absence of a standardized tool to be used by physicians to facilitate the communication and be used as a documentation tool for the communication process and treatment plan.
Background
Patient safety is the primary goal of any healthcare system and it might be affected by many factors, especially communication errors and lack of team work.1 Having effective communication is one of the main recommendations and priorities highlighted by Joint Commission International (JCI).2 Likewise the World Health Organization's (WHO) report (2009) indicated clearly that communication is one of the vital issues that affects patient safety.3 It is a very legitimate reason why these organizations and others are focusing on improving medical staff communication because of its potential adverse effect on patient's safety due to being handed over between different physicians during hospital stay,4 which might be a potential source of communication failure if it is not done properly.5 Improving communication among healthcare providers is a complex process. Therefore, developing and using a standardized communication tool (handover) has shown as effective approach to decrease communication errors and patients harm.6 However, proper use of standardized communication tool “handover” requires staff commitment and changes in policies and procedures governing and managing the overall quality improvement of patient care.7
Baseline measurement
The trigger which highlighted the existence of this problem was the increase in the number of calls between physicians asking about missing information that was not provided during the regular handover. In addition, this potential source of miscommunication was one of the findings reported in the Joint Commission International (JCI) mock survey. As a result, the Oncology Department identified that adherence to proper hand over system among physicians was poor and should be improved by having a standardized tool and systematic approach.
Design
The Departmental Quality Leadership Committee (DQLC) evaluated various communication methods and tools which are used in patient care setting. The most comprehensive method of communication was a standardized form of hand over stressing on specific information that is called ISBAR (Identify, Situation, Background, Assessment and Recommendation) which is routinely used by nurses in our hospital. Thus, we adopted the (ISBAR) as electronic form to be shared via email among physicians at specific point of time during the day (morning 8-9 a.m. and afternoon 4-5 p.m.), when the physicians must acknowledge receiving the handover email to assure proper communication.
Strategy
We used rapid cycle improvement Plan-Do-Study and Act (PDSA) methodology to test and evaluate the new handover process. We executed 4 PDSA cycles; each cycle duration was 1 month. Data were separated on biweekly basis.
PDSA #1
Plan
Developing electronic hand over form based on the ISBAR tool.
Piloting the form with the adult medical oncology physicians.
Monitoring the compliance hand over among physicians monthly.
Do:
The electronic handover form was developed by the quality team and then physicians feedback was obtained.
Modifying the form based on the physicians feedback.
The section head explained to the team the components of the hand over form, purpose behind it, and when and how to use it.
Email was chosen as the communication method to circulate the handover form between the team.
An email distribution list was created.
The quality specialist monitored the care transfer points (the hand over email) daily as a process measure.
Study:
According to physicians' feedback, the form was very helpful in prioritizing patients care.
Based on the feedback from on-call physicians, an acknowledgement of receiving the email as needed.
Some physicians in the outpatient clinic were not familiar with the process at the beginning and they thought that hand over form is related to physicians who are covering inpatient services only.
There was some misunderstanding about the hand over points and acknowledgment between the team.
Some handover forms were sent without updating the date and time fields.
The rate of monthly compliance to hand over form was 77% in the first month.
Act:
The on-call physicians were asked to send an acknowledgement of the receiving email to the rest of the team to assure proper communication.
The Section Head and the team leader of the project clarified to the physicians that the hand over form will not replace verbal communication between physicians and explained to them the following points:
A. When and what are the handover points and acknowledgment times.
B. The process of handover includes the entire team regardless to their services area (inpatient or outpatient).
C. The process of handover is not only to endorse the new patients, but should also to endorse all of our patients.
D. The physicians must complete date and time fields before sending the handover form.
We will retest the idea of electronic Hand over form in other PDSA cycle.
PDSA Cycle #2
Based on the lessons learned form the PDSA cycle 1 we did the second PDSA cycle as follows:
Plan
The Section Head will meet with team to discuss the findings of first (PDSA) cycle to come up with proposed solutions.
Keep monitoring with compliance to hand over.
Do:
The Section Head communicated with staff in writing and in person to adhere to hand over process strictly.
Study:
Monthly endorsement compliance rate was 64%.
The missing update for the date and time fields is still noticeable problem and adding to it the incomplete filling of the patient's active problems section.
A Quality Improvement (QI) specialist was not included in all emails.
Act:
Section head support was needed to emphasize to physicians to complete date, time and active problem parts in the form.
Formulating a unified email list that include all of the physicians in the team and the quality specialist.
Physicians were instructed to adhere to the standard email distribution list that include all of the medical team and the QI specialist will take the responsibility monitoring the compliance.
PDSA cycle #3
Plan
Primarily to monitor the compliance with hand over among physicians and completeness of the handover form.
Do:
QI specialist submitted the report on compliance with the electronic handover form to section head to meet with the team and briefing the team more about the finding of the second (PDSA)cycle.
Study:
Compliance rate of endorsement reached 90%.
We noticed that the physicians still need more clarification about how to report the handover form during the weekends.
Act:
Need to reemphasize sending handover form during weekend as scheduled.
PDSA Cycle #4
Plan
Give special attention to hand over process during the weekends
Keep monitoring the compliance among physicians biweekly then study the impact of hand over improvement on the length of stay to all patients involved in the handover process.
Do:
Data were collected for handover form compliance among physicians biweekly.
To calculate the average (LOS) on biweekly and linked it with compliance rate of handover.
Study:
The Compliance rate biweekly endorsement by hand over form and reached up to 100%
Increase hand over form compliance rate showed positive impact on decreasing the length of stay (LOS) involved in the hand over process.
Act:
Continue monitoring the hand over compliance rate and link it to length of stay.
Standardize the handover process among oncology physicians and try to make it consistent and part of the daily practice even during official holidays and to include all of the new physicians, residents or medical students.
Results
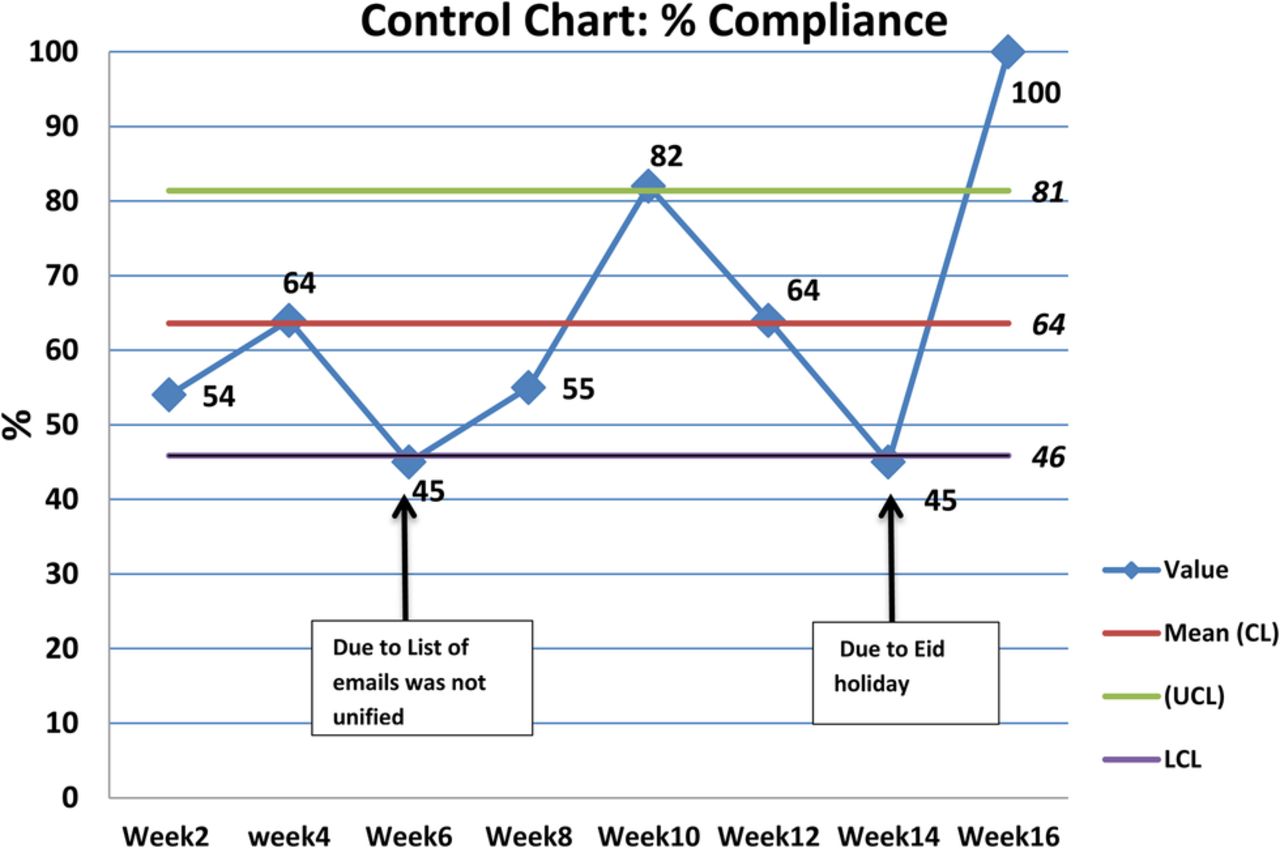
After testing and measuring the idea of using ISBAR as a standardized tool for communication among adult oncology physicians for 16 weeks, the monitoring of daily compliance as a process measures showed significant variation over the four cycles; however, as shown in Shewhart control chart the process is stable under statistical control within ±1SD limit (Figure 1). Biweekly analysis of compliance showed noticeable and steady Improvement of compliance rate reaching 100% at the end of the 4 PDSA cycle; however, there was lower compliance of 45% as a result of special cause during Eid holidays (figure 1). The association analysis of compliance rate with LOS showed that the higher compliance with the hand over had positive impact on shortening the length of stay. (Figure 2, table 1). We also looked at the process measures addressing physicians' acknowledgment of receipt the electronic hand over form by email. There were two check points in the morning and afternoon at 8:32 a.m. and 4:45 p.m. respectively. Maximum acknowledgment of receipt reached was 65% ( 17 out of 26 days), missed days per cycle (0 – 23%).
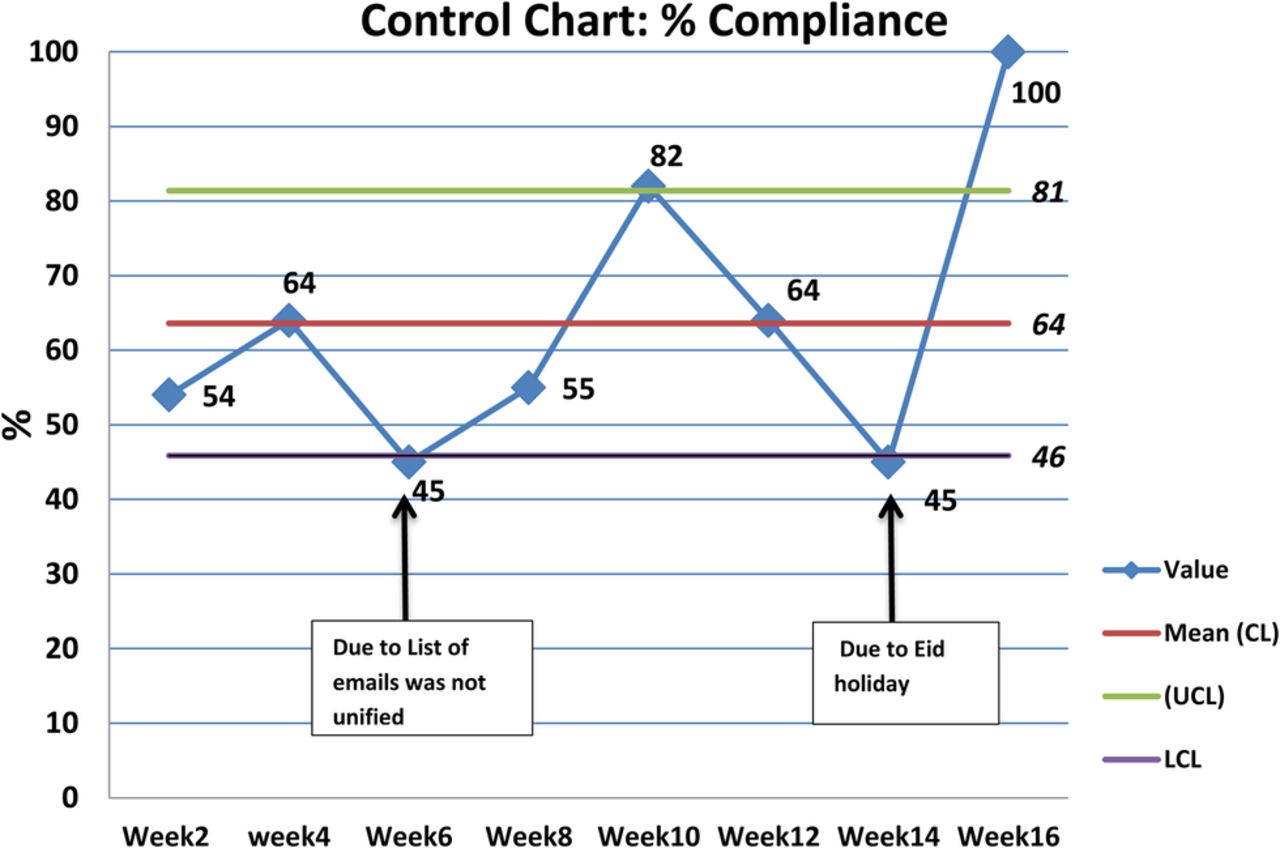
Shewhart control chart: Biweekly compliance rate

{kind=link}
{kind=link}
Biweekly analysis: correlation between handover compliance and average LOS
Handover compliance and average LOS
Lessons and limitations
Several lessons were learned from this project. For example, simple idea with good implementation will lead to noticeable improvement. The implementation was challenged by the physicians who were not sending the handover email to the entire physicians list. Thus, some of the team members remained uninformed about the recent patients' changes. Some physicians asked not to send them the handover email as long as the handover list did not contain any patient under their direct care, this issue was solved by explaining to them the importance of receiving this email as part of a unified list. Some of the physicians were not checking their email regularly and as a result they were unable to send the read notification to sender. Some physicians in the outpatient clinic were not familiar with process of hand over and asked for some clarification regarding hands over points and timing. These challenges were addressed by addressing them with the team by the Section Head. The sustainability of the project requires standardization of the handover process among all oncology physicians in the department and making sure that the process is consistent and part of the physicians daily practice. Having a policy and procedures in place regarding the handover process is an important as well.
Conclusion
By using a well-structured form and method of handover we were able to improve the communication process among oncology physicians. Although as expected, we encountered resistance from physicians, they eventually became convinced and satisfied with the project and its outcome at the end. One physician stated: “the handover form is a very good idea and it's helpful in prioritizing patients' care”. Though it's not statistically proven, we believe that the higher adherence to (ISBAR) communication tool among physicians will have a positive impact in decreasing length of stay (LOS) for our patients and save valuable resources. In summary, developing a handover form to be used as communication tool is a useful approach and will be reflected positively in many aspects of the healthcare process such as improving patients' safety, increasing physicians' satisfaction and it may decrease the length of stay.
Acknowledgments
This work was made possible by the generous cooperation from the physicians in the section of adult medical oncology.
Footnotes
Declaration of interests None declared.
Ethical approval This is a quality improvement project which was approved by the oncology department, the authors believes that there no harm could result from this project neither for the patients' healthcare workers and not revealing any confidential information or identifiers