Article Text

Abstract
Stroke thrombolysis is an important treatment in the management of acute strokes. Its' effectiveness is reliant on prompt administration after stroke onset. Disability free survival at 3-6 months increases by 10% when administered within 3 hours. There is also an economic benefit from early administration with reduced institutional care. New Scottish care standards have been introduced which suggest a target that 50% of suitable patients should receive thrombolysis within 30 minutes, and 80% within one hour 6.
Processes in the Emergency Department play a key role in determining the time a patient waits between arrival and reaching the CT scanner. The project team looked at Ninewells Emergency Department times to CT scanner between May and August 2015 and found that only 20% of patients had their scan within 20 minutes, and 70% within 45 minutes. The team went on to conduct a quality improvement project. This involved initial patient mapping and short interviews with staff. A multi action approach was developed involving education in the form of emails, presentations and visual charts, and the final step was to simplify the paperwork involved. The project was conducted over 11 months and successfully reduced the times to CT, with 60% having had their CT scan within 20 minutes, and 100% within 45 minutes, with a very noticeable reduction in variation around the mean. It is hoped to take this approach forward and apply it to other processes in the department.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Stroke thrombolysis has been shown to improve patients morbidity several months post stroke.1 This has added benefit the sooner it is administered. Scottish stroke standards are continually aiming to achieve tighter targets. To achieve these standards, the Emergency Department (ED) needs to have a slick process to get patients from presentation to the CT scanner. The aim for this project was to, within a year, achieve a target of 50% of potential stroke thrombolysis patients completing a CT head within 20 minutes, and 80% of patients to have had a CT scan by 45 minutes from arrival to allow for radiology interpretation in time to meet the Scottish Stroke Standards.
Background
Stroke is the third leading cause of death in Scotland, and is the leading cause of disability.2 The aim of stroke thrombolysis is to restore blood supply to an ischaemic part of the brain before permanent damage has occurred. In theory the quicker the medication is given, the chance of rescuing more neural tissue is increased, and the better the outcome. This theory is supported by a literature review funded by the Medicine and Healthcare products Regulatory Agency (MHRA) in 2014.1 Evidence suggests that thrombolysis increases disability free survival by 3-6 months by 5 percent when administered within 4.5 hours of stroke onset, and by 10 percent when administered within 3 hours.3 Stroke is estimated to cost the UK £4 billion a year in direct costs as well as at least £1.5 billion productivity losses due to death and disability.4 The cost of staying in a nursing home is on average £570 per week, and a stay in the stroke unit is £164.80 per day. It therefore follows that reducing disability from stroke could lead to financial savings for the NHS. For comparison, the cost per thrombolysis treatment is £750 per patient.5
Ninewells hospital is one of the two acute hospitals in Tayside serving a population of 440,000 people. The Emergency department sees approximately 50,000 new attendances per year. Nine wells has approximately 900 beds. In 2015 Ninewells ED admitted 572 patients with a diagnosis of stroke, 87% of which were ischaemic. 52 patients were thrombolysed, 63% of which were thrombolysed within an hour of arrival at hospital. The ED has a key role to play in ensuring a rapid and safe journey to the CT scanner to facilitate diagnosis. A radiologist or stroke physician will then interpret the scan to ensure there are no radiological findings that would contraindicate thrombolysis. Ninewells Emergency Department is reasonably far away from the CT scanner, involving a lift to get to it and long corridor push. New Scottish Stroke Care Standards set a target for the delivery of thrombolysis of 50% within 30 minutes and 80% within one hour of arrival in hospital.6 The aim of this project was to improve the process of care in the ED in order to ensure improved consistency and speed of transfer to CT.
Baseline measurement
The quality improvement team consisted mainly of Emergency medicine consultant and registrar, with input from the ED team consisting of doctors, nurses and auxiliary nurses. The stroke database for the hospital was used to collect data on those patients who had been through the Emergency Department. This data was collected retrospectively from the start of May 2015 to mid August 2015. The ED assessment cards were then identified for these patients and reviewed.
The project included patients who had been assessed on arrival as being FAST positive strokes (FAST being the rapid assessment protocol acronym developed in 1998 - standing for face weakness, arm weakness and speech impairment testing7), and placed in the stroke assessment room. The team then selected acute stroke patients in whom assessment suggested stroke thrombolysis might be indicated.
Twenty patients met inclusion criteria, 11 male and 9 female. Those patients who met inclusion criteria then had their admission time recorded, their time of CT scan (taken from the time of scan on national radiographic archive) and any cause for delay recorded. It was also noted whether the time they presented was in hours, classed as Monday to Friday 9am to 5pm, or out of hours (weekdays 5pm – 9am, or weekends). Finally outcome was measured by calculating average time from arrival to CT and the percentage of patients who received their CT scan within 20 minutes, 30 minutes and 45 minutes.
A patient journey was mapped early in the project [appendix 1]. A project team member followed a patient who arrived FAST positive and required a CT scan prior to stroke thrombolysis, and stayed with the patient until thrombolysis administration. Due to staffing constraints and unpredictable arrival of suitable stroke patients, this was only conducted for one patient. This highlighted a main delay in waiting for a porter, but also highlighted that lots of small periods of time doing short tasks all added up.
There were a total of 20 patients included before the project commenced. Results showed a mean time to CT of 45 minutes, with a large range between 13 and 112 minutes. 20% of patients had completed scan by 20 minutes of arrival, 40% within 30 minutes and 70% within 45 minutes (see figure 4) There did not seem to be a correlation between time to scan the in hours or out of hours period of the week. Documentation was not always detailed and quite often it was not clear from the notes why a delay had occurred. The number of patients meeting inclusion criteria from baseline measurements led to a plan on how to collect measures throughout the project. Data was collected every 6-8 weeks including approximately 8-10 patients in each analysis. Data collected included electronic arrival time for each patient, and electronic time of CT from national archive.
After baseline measurements were taken, short interviews were carried out with staff. These interviews involved the use of a structured questionnaire with a mixture of open and closed questions [appendix 2]. At this point, staff were informed that this area would be the focus of a quality improvement project. Staff were asked for suggestions of problem areas or areas for improvement.
Problems highlighted from the initial measurements were that there was a large variation in time to CT, suggesting a system that was not reliable. Mean time to CT was too long to allow thrombolysis within the new stroke standards. The patient journey highlighted the importance of streamlining each stage of the journey, mainly initial assessment, nursing interventions and organising a porter to transport the patient to scan.
It was clear from interviews that nursing staff were unsure whether to perform 12 lead ECGs in all patients, and whether to change patients into hospital gowns for scan. There were concerns both from nursing and medical staff in regards to paperwork. Medical staff highlighted the fact that the ED card had to be filled out, but also this had to be duplicated into a specific stroke assessment proforma that was several pages long. Nursing staff felt they had too much paperwork to fill in to get the patient ready for scan such as elderly assessment form, pressure care documentation and a belongings list (see supplementary appendix 1 & 2).
supplementary appendices 1 and 2
Design
The aim for our ED was to perform a CT scan within 20 minutes of arrival in 50% of patients, allowing 10 minutes for radiological interpretation and administration of thrombolysis. We had a secondary aim of 80% of patients to be scanned within 45 minutes of arrival to allow 'door to needle' time of 1 hour. Our aim was to achieve this within 12 months, taking into account the need to embed new processes and understanding that sufficient numbers would be required to demonstrate changes on a run chart.
The interventions included education of nursing staff, a poster to remind staff (senior and junior doctors, and nursing staff) of 'core' jobs involved in managing a stroke patient and we would improve the current paperwork used to assess stroke patients. Staff engagement was needed to help with the interventions involved in the project. Meetings were conducted for joint discussion and decision making to ensure all consultants were happy or aware of changes proposed and had a chance to raise any potential issues. The senior charge nurse was aware of the project from the start and was happy to explain the changes to the nursing staff at regular handover sessions. The stroke team was consulted throughout the process.
Strategy
The project team carried out multiple Plan, Do, Study, Act (PDSA) cycles over an 11 month period from mid August 2015 to mid July 2016. Data was continually collected in the same way as the baseline measurements, allowing for ongoing analysis of interventions. 295 sets of ED assessment cards were reviewed and 53 patients met inclusion criteria (28 male and 25 female). It was decided to focus on the simplest interventions first, such as increased staff awareness of getting stroke thrombolysis patients to the scanner quickly.
PDSA cycle 1: The aim of the first cycle was simply to increase staff awareness and evaluate problem areas that may not have been apparent to team members previously. It was hoped that increased staff awareness would perhaps make staff pay more attention to timing on future thrombolysis potential patients. Conducting staff interviews in the department and discussing the project that was to be undertaken increased staff awareness. There were ten patients included in the project over this period. This simple intervention itself of increased awareness reduced the mean time to stroke to 27 minutes.
PDSA cycle 2: From PDSA cycle 1 we learned that nursing staff had previously been unaware that they did not need to carry out routine ECG's on patients who were deemed suitable for thrombolysis, and that they could go up to scan in their own clothing if not soiled, rather than routine change into a hospital gown. The aim of the 2nd PDSA cycle was to use the information that was attained from cycle 1 to ensure nursing staff had equal knowledge of procedures for stroke thrombolysis patients, and to streamline the issues brought up from the staff interviews that were causing a delay from a nursing perspective. The change hypothesis was that targeting the nursing related delays in transit would improve the time to CT and reduce inconsistency.
These issues were discussed with the senior charge nurse, along with paperwork issues, and the charge nurse emailed all nursing staff educating them about these issues and giving them reassurance that they would not be reprimanded for not filling out pressure sore care/ belongings list as long as it was documented that was not done due to urgency of presentation, and this would instead be completed by the stroke nurses after scan. There was also encouragement to push patients up to scan if there were no porters available. There were 11 patients in this stage of the cycle. This stage of the intervention showed a reduction in the mean time to CT to 18 minutes.
PDSA cycle 3: Following the reduction in time to CT from simple education, the aim of cycle 3 was to educate further through more formal presentations. The change hypothesis was that the time taken to get to CT scanner would reduce further. Presentations were held with small groups of nursing staff using lecture slides. The presentations lasted between five and ten minutes and were held over a few days to try and involve as many nursing staff as possible that were on shift. This stage included 10 consecutive patients. The mean time to scan increased to 28 minutes. Reasons for this increase in time were hypothesised and one of the reasons could be that with presentations and interviews only nurses on shift at the time were targeted. We learned that we had to come up with a strategy to encompass all members of staff that might be involved in the process of care for stroke thrombolysis patients.
PDSA cycle 4: The aim of cycle 4 was to produce a memory aid that could be seen by all members of staff in the hope that this would create a more streamlined and standardised approach to seeing stroke thrombolysis patients through the department. An A3 poster was designed and put up in the stroke assessment room [appendix 1]. This included relevant bleep numbers for the stroke team as well as radiographers to aid senior doctors. The junior doctors were reminded of which blood tubes to take and their role in requesting the CT on the electronic system. Nursing staff had a written reiteration of their role and essential jobs.
Nine patients were included in this cycle and mean time to CT reduced to 25 minutes.
PDSA cycle 5: The final PDSA cycle aim was to simplify the paperwork required to be filled out by senior doctors for potential stroke thrombolysis patients. It was hypothesised that this change would reduce the time taken to reach CT scanner if duplication of paperwork was not required. This was discussed at a consultant meeting to see if there were any suggestions or objections to changing paperwork. Discussion also took place with the stroke team to ensure essential information was collected to inform ongoing patient care. Two simplified A4 stickers [appendix 3] were designed and were stuck in blank ED cards ready for use in the stroke assessment room. The previous paperwork had included contraindication checklist, advice for consenting patients/ families, protocols for the management of hypertension, bleeding anaphylaxis and alteplase dosing. These sheets were not printed out for each patient, but instead turned into a laminated pack, which was kept in stroke room and then transported with patient to scan. Several copies were made in case of accidental misplacement. This cycle included 10 patients and showed a reduction in mean time to CT to 22 minutes.
Any outliers were reviewed and reasons collected for any longer than expected time to scan (see supplementary appendices 3 & 4)
supplementary supplementary appendices 3 and 4
Results
A total of 73 patients were included in the project. 20 prior to project, and 53 throughout the PDSA cycles. The mean time to CT had reduced from 45 minutes to 22 minutes from start to end of project. There was an improvement from 20 to 45% in patients reaching the CT scanner within 20 minutes, after education, and this improved further to 60% after new paperwork was brought in [see Figure 2]. There was also an improvement in the percentage of patients reaching the scanner within 45 minutes from 70% pre-project, to 94% post education, and 100% post paperwork introduction. This improvement could potentially then allow Ninewells hospital to meet the new Scottish stroke care standard targets for time to thrombolysis within the 30 minutes and 1 hour windows.

Percentage of patients completing scan within 20, 30 and 45 minutes of arrival in the department
To aid interpretation of the results a run chart was plotted [see Figure 1]. This showed that the biggest shift in the process was with increased staff awareness at PDSA1. There were fewer runs as the project went on, and few enough to suggest a statistically significant change. All of the astronomical points had their notes reviewed and found to have valid reasons for increased time such as hypertensive patients requiring management, or seizure management, and one case was when junior doctors first stepped up to the senior doctor role, and were unfamiliar with the process/ paperwork. Perhaps this is an area for review, to ensure they have shadowed established senior members of staff more often prior to taking on initial stroke assessment in thrombolysis cases.

Run chart of results
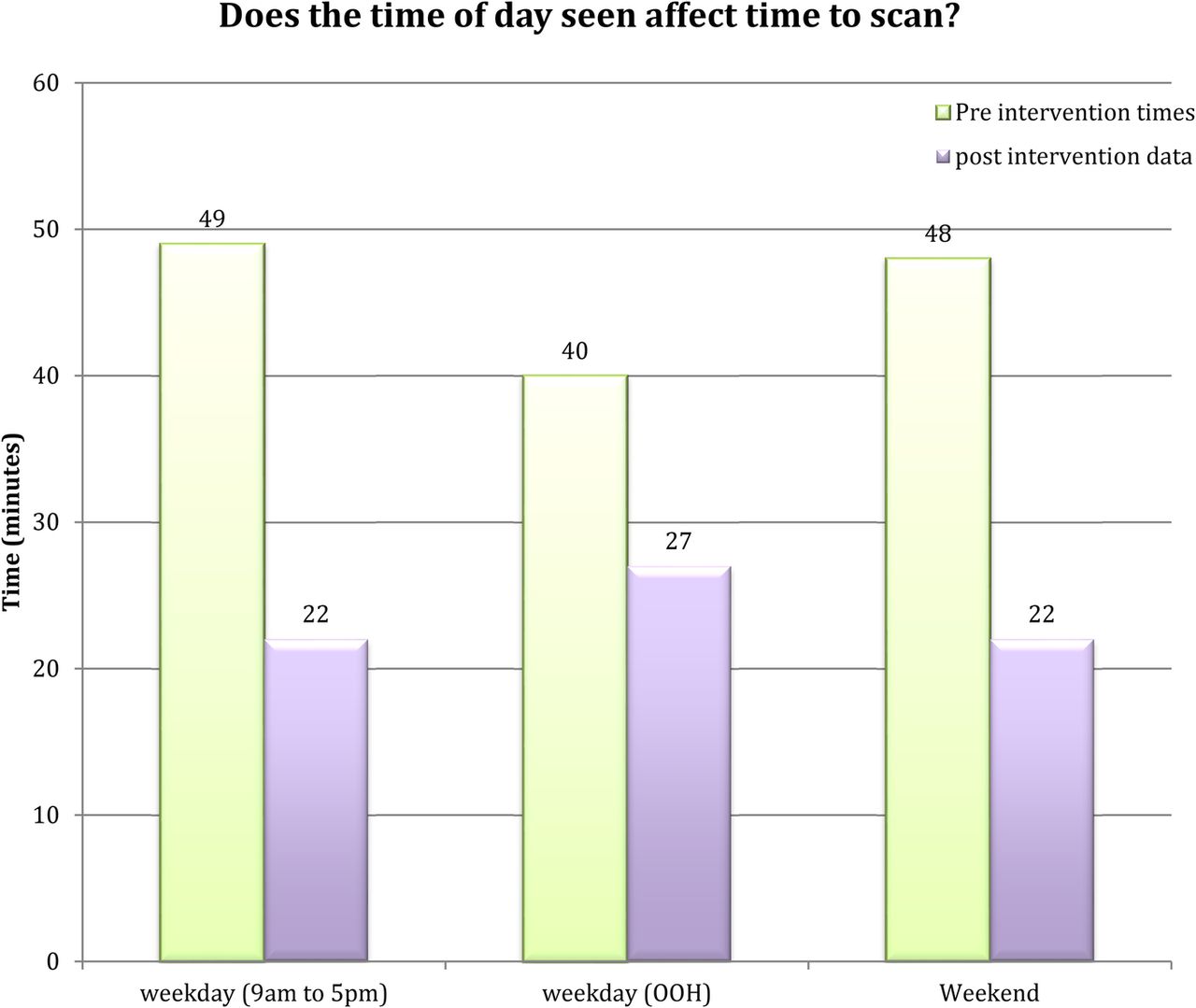
The data would suggest that there was no significant difference between patients seen at weekends, overnight or within normal working hours, and all time periods saw an improvement [see Figure 3].

{kind=link}
{kind=link}
{kind=link}
Effect of time of day on timing to scan
Lessons and limitations
Potential problems of engagement with staff were noted at an early stage, with nursing staff questioning the suggestion that nursing and medical staff pushes patients themselves to scan if a porter was not immediately available. Similarly, not all consultants in the department felt that a change in paperwork was needed. Engagement with doctors and nurses was essential. This was achieved by having meetings for joint discussion and decision making to ensure all consultants were happy or aware of changes proposed, and the project had support from the senior charge nurse who helped to explain changes to nursing staff, and the team listened to their views before implementing any change.
An issue noted in the PDSA cycles was that documentation was limited (probably due to the necessity for speed). This made it more difficult to decipher reasons for delay in many cases. This prompted a change in the paperwork to include a reason for delay section. It was felt that this did not add too much time to complete but add valuable collection data to the project.
Consideration to balancing measures was given. More staff were not being pulled into thrombolysis management than had previously been used, so the team did not feel it affected staffing levels/ care elsewhere. Through speaking to nursing staff, and medical staff, both were happy with the changes brought about by the project, and particularly with the paperwork. Through informal discussions, nursing staff fed back that the educational interventions were useful making the steps/ processes clearer. There was also helpful negative feedback in respect to the recommendation we had made that nurses should push patients to scan if porters were unavailable, some nursing staff pointing out that this was not in their job remit and they were not happy to push patients the long distance to the scanner. This feedback was taken on board and not pushed further and was removed from educational interventions. The stroke team did not give any negative feedback from their point of view about the change in paperwork they were receiving.
It is appreciated that all of the interventions in the project may not work in every Emergency Department. Every department works differently and not all departments have thrombolysis on site. It is hoped though that whatever the process the cycles in this project, however, have been simple and with analysis of events/ cases, education based on these findings and simplification of paperwork involved may help reduce times involved in thrombolysis in any hospital even if the overall times cannot meet similar time targets.
This project is sustainable through regular presentations and ongoing collection of data on a two monthly interval to ensure any shift in trend is analysed and addressed. This does not involve too much time, or too many staff members to make it a difficult task. The paperwork has been simplified rather than added to, so should not be any more of an undertaking for staff.
Conclusion
The Emergency Department has an important role to play in the stroke patient's journey to thrombolysis. This project has shown a large reduction in time taken to transport patients to the CT scanner, reducing mean time to CT from 45 minutes to 22 minutes and therefore increased the chance of receiving thrombolysis within a shorter window of time, and increasing the chance of success, as shorter time frames to scan have been associated with better outcomes.3 The improved timings in the department are also in keeping with potentially meeting the most recent Scottish Stroke Care Standards of stroke thrombolysis door to needle time of less than 30 minutes in 50% of patients, and less than an hour in 80% of patients.6 This improvement was achieved through a gradually implemented combination of increased awareness, staff education about the essential and non-essential tasks prior to getting patient to the scanner, and by simplifying paperwork. This could potentially be easily replicated in other Emergency Departments, particularly as the largest significant change in time to scan was achieved through increased awareness only. The team hope to maintain the improvement by continual reiteration of education, this can be achieved through updates about performance in the staff base, and regular emails and presentations. Next steps for this project would be discussions with the Scottish Ambulance service to improve pre alerts. That may allow usage of time before the patient arrives to source some background information about the patient that may reduce the decision making time during assessment on patients suitability for thrombolysis. With time, the project team would hope that the overall PDSA cycle approach taken with this project might be used to streamline other department processes.
Acknowledgments
Moira Raitt for her help in distributing emails to nursing staff and for organising times when presentations could be given to nursing staff. Lisa Maloney for helping with the organisation of printing out poster and ordering/ printing stickers.
Declaration of interests
Nothing to Declare
Ethical approval
Ethical approval not required as work was for quality improvement purposes and exempt by local policy