Article Text

Abstract
Up to 30% of patients who have periorbital trauma will have ocular injury with devastating consequences if missed. All staff working with acutely injured Oral and Maxillofacial Surgery (OMFS) patients should be competent in a basic eye examination with documentation of visual acuity, gross visual fields, eye movements, diplopia, and pupillary responses at a minimum. As a standard we adapted guidance published by the Emergency Care Institute New South Wales to assess the documentation of the eye examination in OMFS patients at King's College Hospital with any periorbital injury. After initial assessment we presented the data in the departmental audit meeting, then gave a detailed teaching session to junior doctors and introduced an ‘eye exam’ proforma sticker designed to act as an aide memoir. At baseline, 38 eye assessments across all clinical environments and by all seniority of clinician were assessed at random. Of these, 41% of these had visual acuity documented, 5% visual fields, 47% pupils, and 83% movements. After presentation of data, reaudit showed progress to 81%, 0%, 94%, and 100% respectively. Following the teaching session reaudit showed final progression to 83%, 46%, 83%, and 100%. Teaching sessions and use of an eye sticker proforma has been shown to improve rates of documentation of the eye exam for those OMFS patients presenting with periorbital injuries.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Patients at risk of occular trauma as a result of periorbital injury were noted to have missing eye examination documentation. This was felt to be due to clinician lack of knowledge and/or training that periorbital trauma is associated with occular injury and how to document a thorough eye examination.
At King's College London Hospital our team of a Core Surgical Trainee Year 1, Dental Foundation Year 2 trainee, Maxillofacial Registrar, and Consultant Maxillofacial Trauma Surgeon set out to to ensure that patients suffering periorbital trauma have documentation of their visual assessment and improve performance by junior doctors by means of a bleep free teaching session on the eye examination and a visual assessment proforma sticker.
Background
Up to 30% of patients who have periorbital trauma will have ocular injury1 with potentially devastating consequences if missed. Rapid assessment and examination following trauma to the eye area is essential and a thorough knowledge of potential injuries is imperative to ensure rapid diagnosis and to preserve visual capacity.
The basic eye examination is a requirement of the undergraduate MB BS curriculum as outlined by the Royal College of Ophthalmologists.2 They specifically state that medical students should aim to have competence and understanding in basic ophthalmic history taking and examination including: visual acuity measurement, pupil assessment, confrontation visual fields, extraocular movement testing, and direct ophthalmoscopy.
This also applies to singly dentally qualified junior doctors working in oral and maxillofacial departments3 where they must be able to perform a complete history and examination of emergency presentations. All staff working with acutely injured oral and maxillofacial patients should be competent in a basic eye examination. Those assessing patients suffering periorbital trauma should document visual acuity, gross visual fields, eye movements, diplopia, and pupillary responses at a minimum.4
Previous studies have shown that almost half of surveyed junior doctors in oral and maxillofacial surgery training posts felt out of depth in their jobs and this was more likely if they did not have bleep free training sessions.5
At the Oral and Maxillofacial department at King's College Hospital we sought to ensure that patients suffering periorbital trauma have documentation of their visual assessment and improve performance by junior doctors by means of a bleep free teaching session on the eye examination and a visual assessment proforma sticker.
Baseline measurement
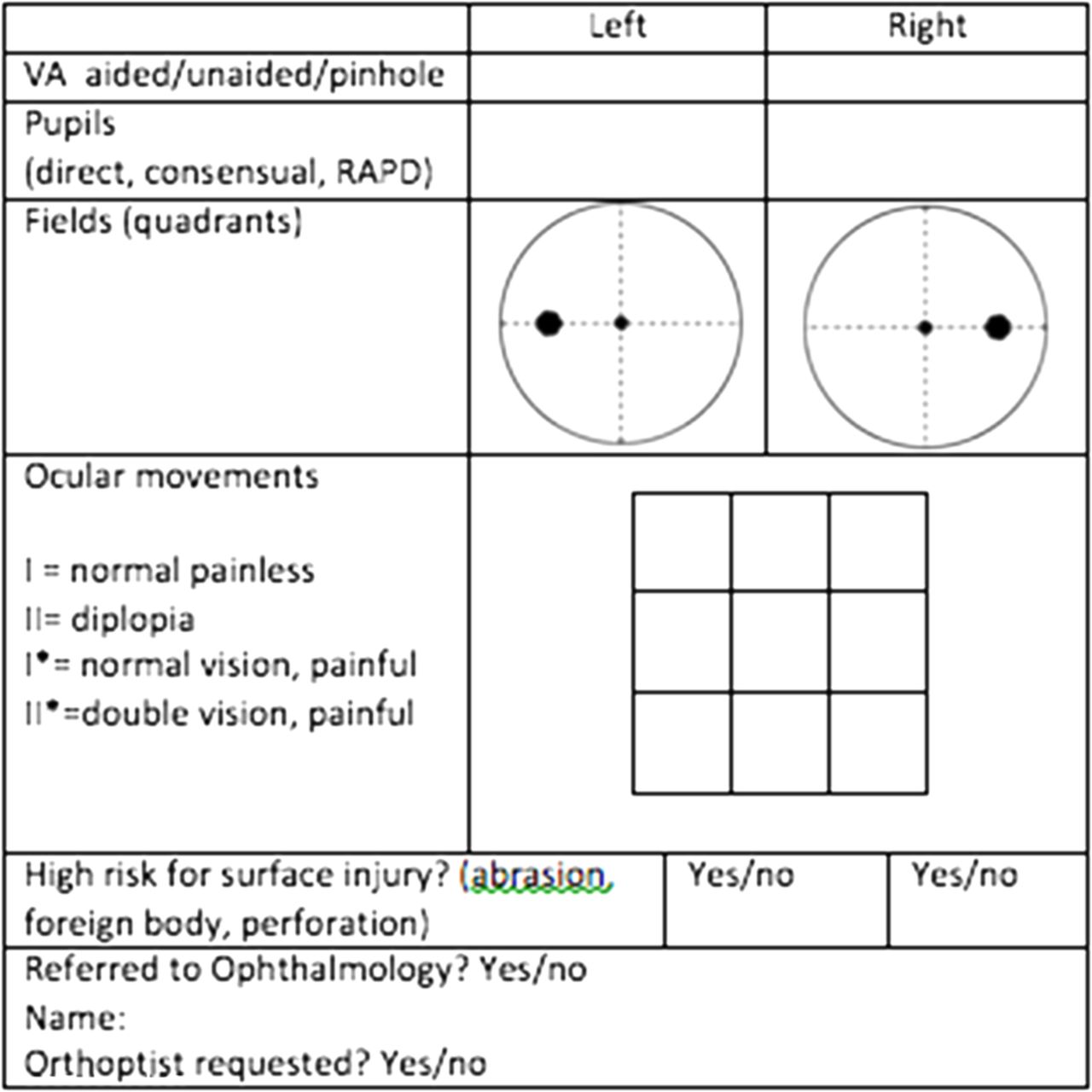
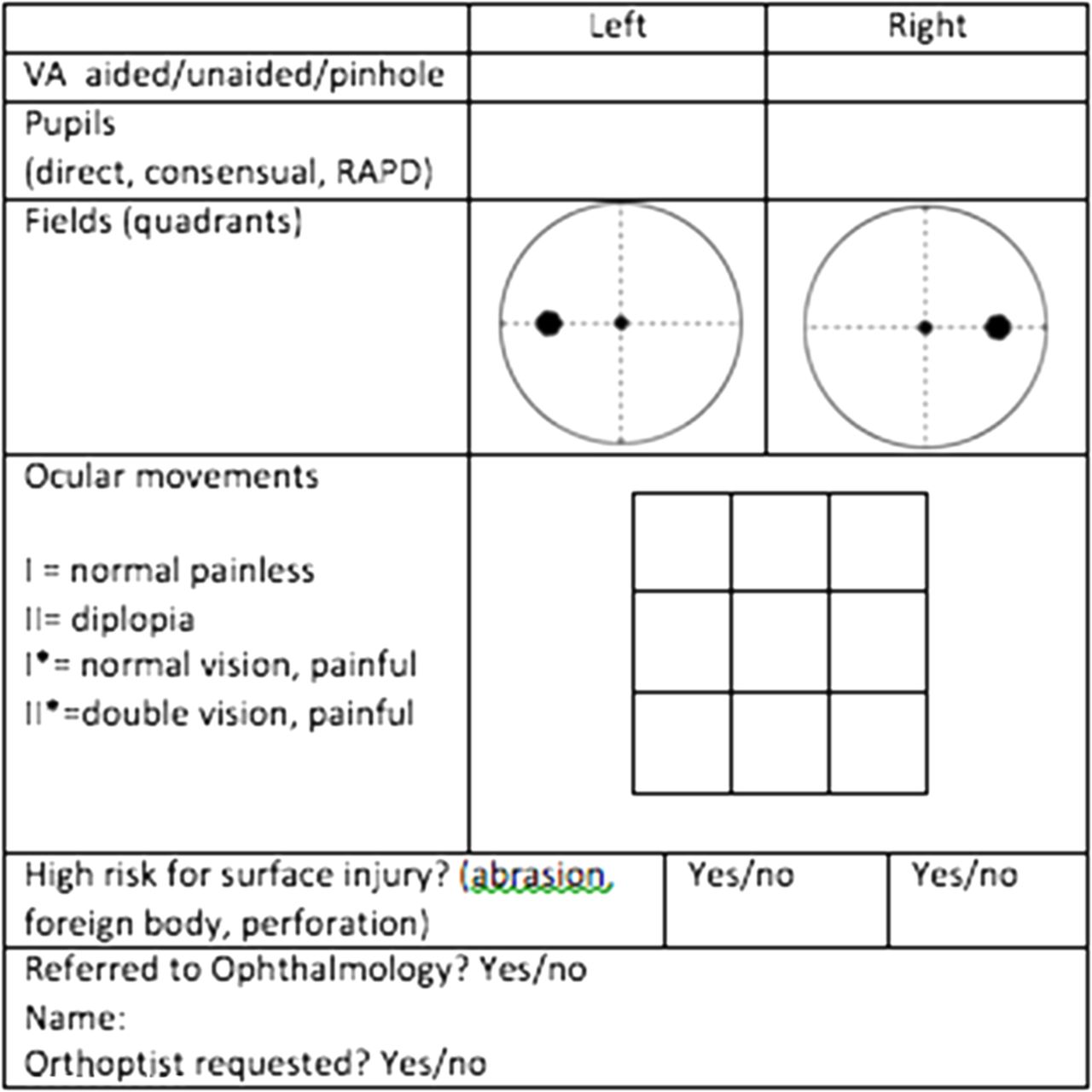
As a standard we adapted guidance published by the Emergency Care Institute New South Wales4 to undertake an audit on the documentation of the eye examination in OMFS patients with any periorbital injury. The audit criteria included documentation of visual acuity, visual fields, pupillary assessment, and eye movements.
The baseline measurement was a retrospective case notes analysis involving random case note selection of patients suffering periorbital trauma over the preceding two years. The cases were randomly selected from a database of patients having visual acuity assessments done in clinic. Approximately 150 patients were recorded in pages of a periorbital trauma/visual acuity book kept in clinic by nursing staff – pages from this book were selected randomly and resulted in 24 patients being selected for baseline measurement. 38 eye assessments across all clinical environments and by all seniority of clinician were done for these 24 patients and were assessed according to our proposed audit criteria. Of these, 41% of these had visual acuity documented, 47% pupils, 83% movements, and 5% visual fields.
Design
The baseline data was presented in the departmental audit meeting in order to inform and generate discussion amongst stakeholders. The stakeholders were: consultant OMFS surgeons, registrars, dental OMFS SHO's, and medical OMFS SHO's. It was unanimously agreed that a teaching session should be given on the eye examination for periorbital trauma and how this should be documented. The authors suggested the addition of a proforma sticker at the meeting and this was well received.
The proforma sticker required approval from the consultants and production therefore the teaching session including teaching on documentation using the sticker was implemented two weeks after initial audit presentation.
Strategy
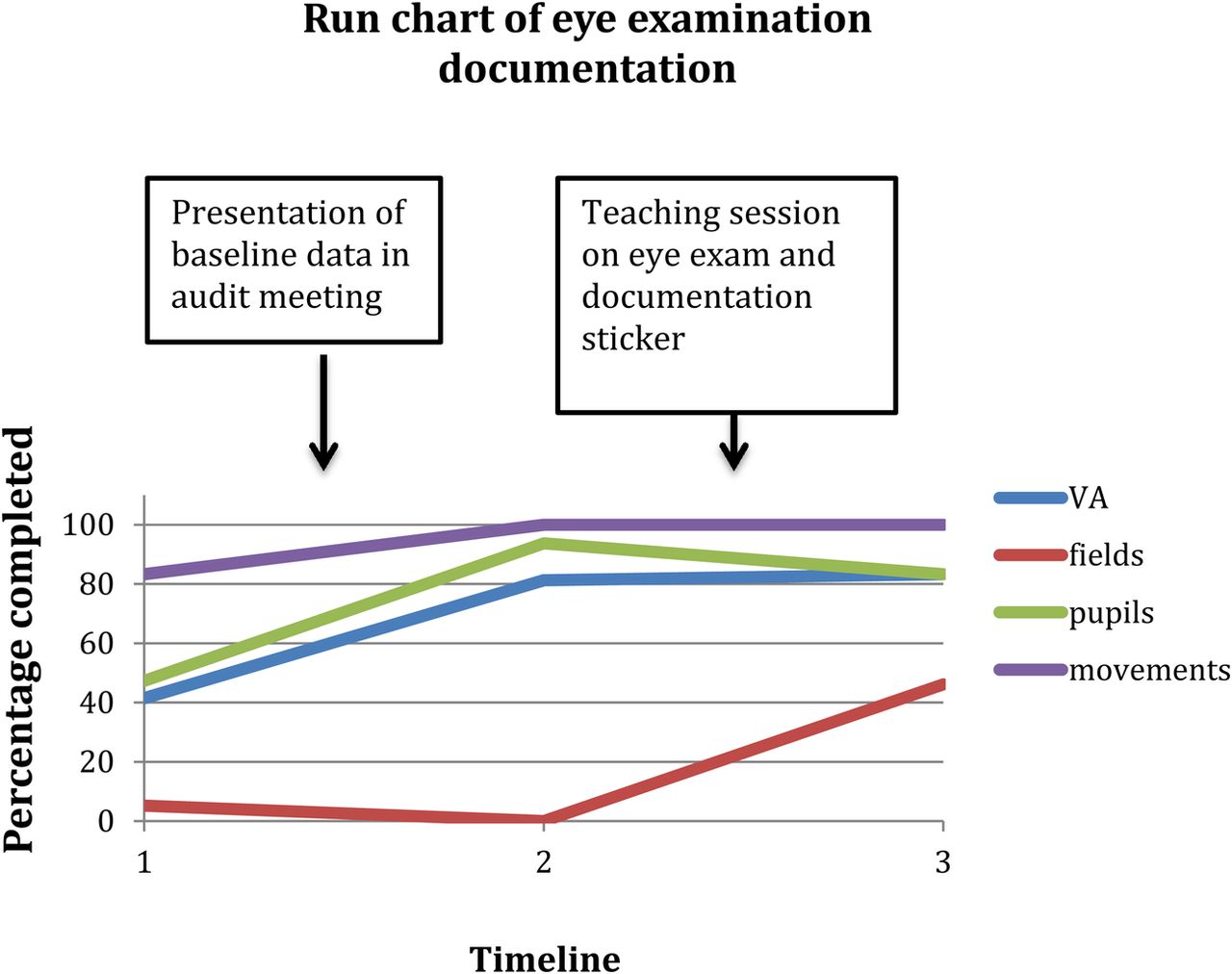
PDSA 1 – Having noticed instances of poor documentation, the baseline measurement of visual acuity, fields, pupils, and movements was done. This revealed 41% of cases had visual acuity documented, 5% visual fields, 47% pupils, and 83% movements. These audit standards and results were presented in the departmental audit meeting to raise awareness. Following this, 16 consecutive eye exam notes were reaudited, showing 81% of cases had visual acuity documented, 0% visual fields, 94% pupils, and 100% movements. The improvements were attributed to increasing knowledge of the importance of the eye examination, but there remained a knowledge gap in terms of performing the actual examination and documenting this.
The action for this was to provide the eye assessment sticker to act as an aide memoir for the eye examination and make completing documentation easier. There was a detailed bleep free teaching session on components of the eye examination – with a focus on visual fields as this was the area of worst performance. It was highlighted that Visual Acuity must be assessed as mandatory in patients with periorbital trauma and that barriers such as Snellen chart availability could be overcome by using a smartphone app, or the eye treatment room in A&E, or printed copies available on the ward and in clinic. A further 12 consecutive eye exam notes were reaudited, showing 83% of cases had visual acuity documented, 46% visual fields, 83% pupils, and 100% movements.⇓
Results
Visual acuity showed a consistent increase from 41% to 81% to 83% of case notes having documentation. Documentation of visual fields showed an overall improvement from 5% to 46% but had a dip to 0% prior to the teaching session. Documentation of pupils also showed an overall increase from 47% to 83%. Eye movement documentation showed a consistent increase from 83% to 100% and 100% (see fig 1 – run chart of eye assessment documentation rates).⇓

{kind=link}
{kind=link}
Lessons and limitations
Although there was an overall increase in documentation rates for visual acuity, visual fields, and pupil assessment; there was decline in performance of visual fields documentation before a rise. Similarly there was a small decline in pupil documentation following the teaching session. These fluctuations were attributed to be due to small sample sizes of the reaudits.
There was a more marked jump in visual acuity, pupils, and movements documentation following presentation in the departmental audit meeting alone than with the teaching session. This is suggestive that awareness of the need for this documentation, rather than how to perform and document was the problem. The increase in awareness of Snellen chart availability may also have contributed to the improvement in Visual Acuity documentation.
Documentation rates still do not approach 100% and the area of visual fields remains weak. This may be impacted by the short time intervals between measurements and resultant small sample sizes. This was largely due to the fact that the project lead had only a four month rotation in the specialty, handover of the project to a dental trainee to lead may allow greater time intervals and as a result greater sample sizes since their placement is 12 months long.
Further evaluation will be undertaken in order to identify remaining barriers for documentation of visual assessment and how to improve this further. This will include analysis of utility of the proforma sticker and critique of the proforma sticker itself.
We hope to repeat measurements in the near future to assess sustainability of improvements as a result of the proforma sticker. It will be interesting to see if the measurements improve or decline with the changeover of junior doctors and dentists, as well as assess the impact of the eye assessment teaching session for the new group.
Conclusion
Departmental audit and a teaching session for junior doctors on eye examination together with use of an eye sticker proforma have been shown to considerably improve rates of documentation of the eye exam in patients presenting with periorbital injuries. Snapshot audit shows fluctuating levels of eye assessment documentation but an overall increase from baseline. We hope that this quality improvement project will be replicated in other trauma centres that have significant numbers of patients with periorbital trauma.
Acknowledgments
Mehual Tailor – Dental Foundation Year 2 Trainee
Ambika Chadha – Oral and Maxillofacial Surgery Specialist Registrar
Miss Kathleen Fan – Consultant Oral and Maxillofacial Surgeon (supervisor)
Footnotes
Declaration of interests Nothing to declare
Ethical approval Ethical approval not required.