Article Text

Abstract
Sheikh Khalifa Medical City (SKMC) in Abu Dhabi is the main tertiary care referral hospital in the United Arab Emirates (UAE) with 560 bed capacity with a high occupancy rate. SKMC senior management has made a commitment to make quality and patient safety a top priority. Preventing health care associated infections, including Catheter Associated Urinary Tract Infection (CAUTI), is a high priority for our hospital.
In order to improve CAUTI rates a multidisciplinary task force team was formed and led this performance improvement project. The purpose of this publication is to indicate the quality improvement interventions implemented to reduce CAUTI rates and the outcome of those interventions.
We chose to conduct the pilot study in General Medicine as it is the busiest department in the hospital, with an average of 390 patients admitted per month during the study period. The study period was from March 2015 till April 2016. Our aim was to reduce CAUTI rates per 1000 device days in the medical units. Implemented interventions resulted in a reduction of CAUTI from 6.8 per 1000 device days in March 2015 to zero CAUTI in February through April 2016.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
High CAUTI rates were identified in the medical units in March 2015. Compliance with recommended evidence based infection-prevention practices was a challenge. In order to improve CAUTI rates a multidisciplinary task force team was formed and led this performance improvement project. The focus of this team was to target frontline staff education and training, ownership and accountability as a means to improve compliance with CAUTI prevention measures. The goal was to reduce CAUTI rates per 1000 device days in the medical units (total 170 beds) during the study period (March 2015 till April 2016) by implementing evidence based infection-prevention practices.
The data was extracted from the electronic medical record and validated by the infection control team following the National Healthcare Safety Network Guideline (NHSN, 2015).5
Background
CAUTI is one of the most common healthcare associated infections. It is a leading cause of secondary blood stream infection resulting in increased morbidity and mortality with an estimated 13,000 attributable deaths annually, increased length of stay by 2-4 days and increased healthcare costs with additional cost $1200-2400 per case.1 Overuse of indwelling urinary catheters (15-20% of hospitalized patients) contributes to the frequency of hospital associated urinary tract infections and the duration of urinary catheterization is the single most important risk factor for developing CAUTI (each day an indwelling urinary catheter remains the patient has a 5% increased risk of developing CAUTI). Urinary catheters are commonly placed for inappropriate indications and healthcare providers are often unaware that their patients have catheters leading to prolonged unnecessary use.2 Up to 60% of CAUTI are considered preventable; provided that recommended evidence based infection-prevention practices are implemented. Guidelines for the prevention of CAUTI recommend appropriate catheter use, aseptic insertion, use of closed drainage systems, proper maintenance and timely removal of indwelling urinary catheters, as well as the use of established practices such as hand hygiene. Prevention strategies must focus on clear indications for the insertion of urinary catheter, proper maintenance while in use and early catheter removal.3–4
Baseline measurement
CAUTI rate in the medical units in March 2015 was 6.8 per 1000 device days (3 CAUTI per 441 catheter days). CAUTI cases were identified by the infection control team through active surveillance from the electronic medical record.
Design
Methodology used was prospective study of monthly CAUTI rates per 1000 device days in the medical units during the study period. The data was extracted from the electronic medical record and reported monthly by the infection control team following the National Healthcare Safety Network Guideline (NHSN, 2015).5 In March 2015 high CAUTI rates were identified in the medical units. Senior leadership initiated a performance improvement multidisciplinary taskforce team with representation from physicians, nurses, infection control and quality. Brain storming sessions were conducted and areas for improvement were identified. CAUTI prevention strategies were developed, implemented and evaluated through a series of Performance Improvement cycles.
Strategy
CAUTI prevention improvement efforts were initiated in the medical units. The key performance improvement interventions were tested and their impact on improving the CAUTI rates was as follows:
Cycle 1 (April 2015 till May 2015)
Standardize urinary catheter insertion and maintenance bundles based on established evidence based guidelines.
Monitor compliance with urinary catheter bundles and provide timely feedback to frontline staff on process and outcome measures related to appropriate catheter use and CAUTI rates.
Education awareness campaigns and periodic in-service competency based training of healthcare personnel involved in insertion and maintenance of urinary catheters.
Just in time coaching by clinical resource nurses (CRNs) and infection control links.
This improved CAUTI rates per 1000 catheter days from 6.8 in March to 5.0 in May 2015
Cycle 2 (Jun 2015 till Aug 2015)
Develop facility based criteria for acceptable indications for urinary catheter insertion and empower nursing staff not to proceed with catheter insertion when criteria not met
Build criteria for catheter insertion into computerized order entry systems using physician urinary catheter insertion order with mandated indication.
Daily assessment of urinary catheter necessity by nurses at the start of every shift with the requirement to contact physician if insertion criteria are not met.
Use standardized written reminders on the nursing boards to target opportunities to remove urinary catheter.
This improved CAUTI rates per 1000 catheter days from 5.0 in May to 3.64 in August 2015
Cycle 3 (Sep 2015 till Jan 2016)
Standardize the urinary catheter insertion, maintenance and removal process
Education on the need to avoid clamping and flushing of urinary catheters.
Promote consistent perineal care practices.
Improve availability of portable bladder scans to assess residual urine volume and avoid unnecessary urinary catheter insertion.
This improved CAUTI rates per 1000 catheter days from 3.64 in August 2015 to 2.14 in January 2016.
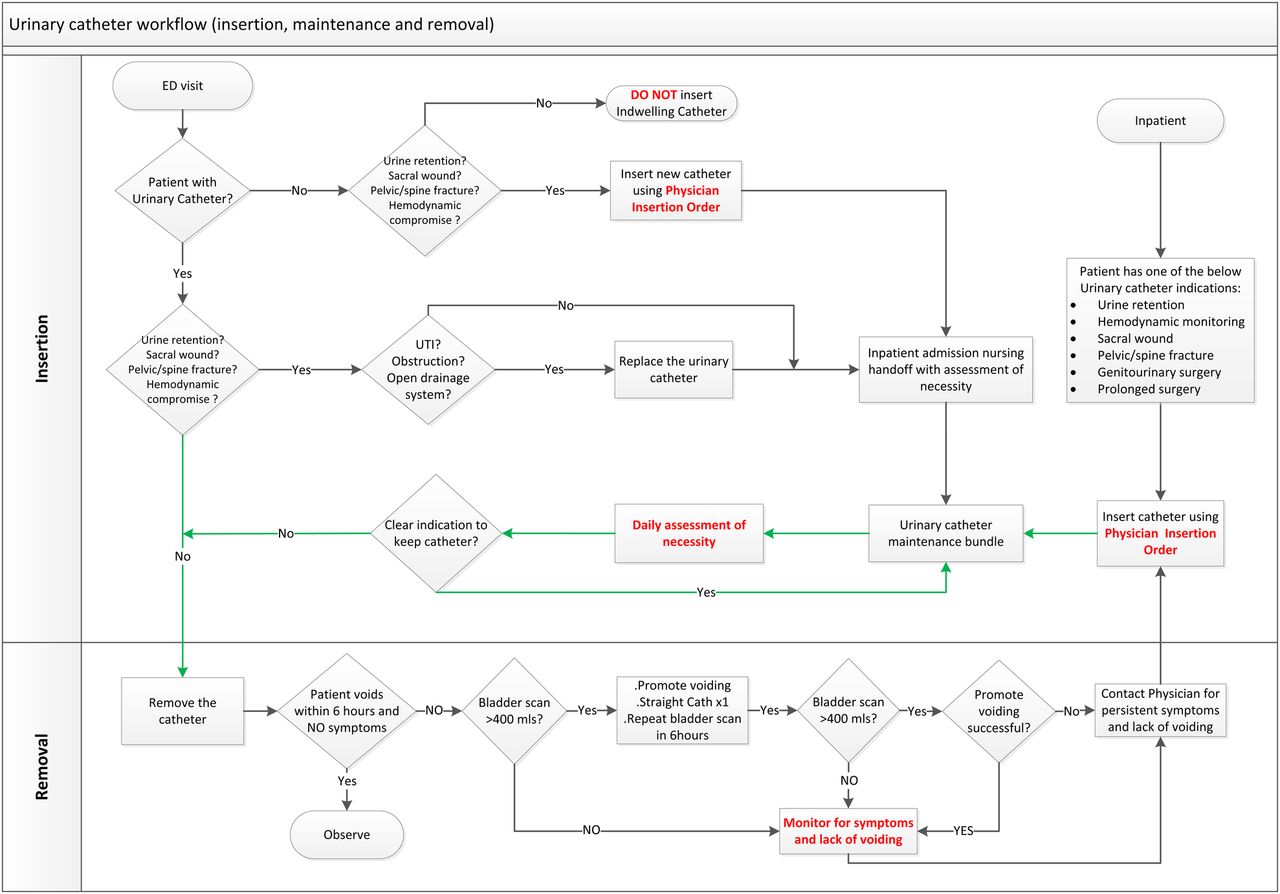
As the result of those interventions Urinary Catheter Workflow was developed and implemented in Feb 2016 and this led to a sustained improvement in CAUTI rates to zero over the last 3 months of the study period (February through April 2016).
Figure 1 Urinary Catheter Workflow

Results
With the implemented performance improvement interventions CAUTI rates were reduced from 6.8 per 1000 device days in March 2015 to zero in February through April 2016
Figure 2 CAUTI per 1000 catheter days in the medical units

{kind=link}
{kind=link}
Lessons and limitations
Senior management support and empowerment was one of the critical success factors. However, it took time to get buy in and engagement from frontline staff due to different background education and training. The sustainability of this improvement will need continued frontline engagement and maintaining leadership support.
Conclusion
The multidisciplinary taskforce team managed to implement quality improvement interventions and change management strategies6 that resulted in significant sustained reduction in CAUTI rates in the medical units. Implemented interventions are generalizable and can be replicated in the other wards. Lessons learned were disseminated throughout the organization. This improvement project will enhance patient safety and reduce preventable harm from CAUTI. Commitment and support from senior leadership was critical to the success of this project.
This performance improvement project shows that performance improvement teams should engage frontline staff in order to overcome resistance to change and implement sustainable systems.
Acknowledgments
Thanks to SKMC senior management for all their support and empowerment and to frontline staff in the medical units for their engagement. Special thanks to the infection control team.
Footnotes
Declaration of interests None of the authors have any declared conflict of interest.
Ethical approval This was a performance improvement project hence it is exempt from ethical approval requirement.