Article Text

Abstract
Patients with mental illnesses have a high rate of physical comorbidity, and specifically, those with psychosis are at an increased risk of cardiometabolic disease and shortened lifespans, due to medication, lifestyle and illness factors. There are recognised challenges with physical health care in this group.
At baseline, no patients on the Bath and North East Somerset Early Intervention in Psychosis caseload had a fully completed physical health assessment. Our aim was to offer a physical health check, blood tests, and ECG for all patients, trialling four phases of interventions. The four phases were (1) increased awareness, education and data collection tools; (2) mobile physical health clinics; (3) letters sent to patients and GPs to request health checks be conducted, (4) a combination of the above approaches, as well as regular caseload reviews and prompts to professionals. At the time of our study (2015-16), many of the above parameters were also incentivised nationally by Commissioning for Quality and Innovation (CQUIN) payments. The mobile physical health clinic offered patient choice of home visits or clinic checks, to increase engagement and provide flexible care.
The most successful approach overall was the combination approach, resulting in 48% of all patients having fully completed physical health checks, bloods and ECGs. The mobile clinic resulted in physical health checks completion rates of 60%, and blood tests in 65-70%. 92% of patients undertook ECG's, following letter requests to GPs and patients.
Combining mobile physical health clinics, GP letters, financial incentives and managerial engagement produced much improved results, but was very time consuming, and in our case was inefficient due to using multiple professionals. We recommend embedding such approaches within the team, using sustainable systems, and would encourage teams to trial dedicated trained clinicians to establish sustainable systems to improve the physical health care of this vulnerable group.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The World Health Organisation Report in 2001 identified that psychosis in young people, including schizophrenia, was a very significant cause of morbidity, disability, and economic cost worldwide.1 In 2005 the Royal College of Psychiatrists published a five-year action plan for the early detection and treatment of psychosis.2
The Bath and Northeast Somerset Early Intervention in Psychosis Service consists of a team of doctors, nurses, occupational therapists, and healthcare support workers, who have access to psychology and family therapy practitioners for referrals, consultancy, and supervision. The service primarily works with people aged between fourteen and thirty-five who are experiencing either psychosis or prodromal symptoms which place them at risk of psychosis. The team complete an initial assessment and then provide rapid and intensive support for patients and their families for up to three years.3
As for all patients with psychosis, there are recommendations in place that patients under the care of Early Intervention in Psychosis Services have a comprehensive physical health assessment at least annually. The responsibility for this lies with secondary mental health services for the first year, or until the patients mental health has stabilised, whichever takes longer.4
We identified there was no system in place to ensure baseline and annual physical health checks were consistently offered to patients on the Early Intervention in Psychosis Team. We quickly identified that the majority of patients did not have up to date physical health checks.
Psychiatric doctors in the team had primarily assumed responsibility for this role. The number of medics on the team varied from a half time consultant to, at full capacity, a half-time consultant and two full-time junior doctors. Many Early Intervention Teams have no dedicated medical input, with the majority of clinicians having minimal physical health training.
Our aim was to implement a robust, reliable system which enabled all patients on the caseload to have the opportunity for relevant health checks at baseline and annually, ideally one which was not dependent on medical staff, the availability of which was highly variable. This would not only lead to an improvement in quality of care for patients, but during the time of our project, would also result in increased payments via national CQUIN scheme5 enabling further improvements in patient care.
In SMART terms, our aim was to improve compliance with recommended physical health monitoring for all patients on the Bath and Northeast Somerset Early Intervention in Psychosis caseload, as measured against national and local guidelines (detailed below). This would be the responsibility of the entire multidisciplinary team, with Care Coordinators responsible for their own caseloads but led by the project authors. Given the protected and specific caseload with expertise in psychosis, we felt that it was realistic to aim for 100% compliance. The project was expected to run from February 2015 to August 2015.
Background
Repeated studies have demonstrated that the lifespan of people with severe mental illness (SMI) is shorter compared to the general population, equating to a 13-30 year shortening in life span, mostly due to physical illness.6 Many physical disorders such as cardiometabolic and nutritional, have been identified as being more prevalent in individuals with serious mental illness compared to the general population. This excess mortality and morbidity is multifactorial,7 but primarily due to increased prevalence of cardiovascular disease associated with antipsychotic drugs and with modifiable risk factors, including weight gain, low exercise, poor diet, and high prevalence of cigarette smoking.8 Some atypical (second-generation) antipsychotics are associated with significant weight gain (<7% of baseline), dyslipidaemia, and hyperglycaemia (metabolic adverse effects). Individual atypical antipsychotics differ in their propensity for metabolic adverse effects: available data suggest that clozapine, olanzapine, and quetiapine are especially implicated.9 Increased access to physical health monitoring and effective interventions (such as smoking cessation services) for patients suffering from severe mental illness, especially those receiving antipsychotics, is vital. Recent studies suggest that weight loss programmes targeting those already overweight can be achieved, but sustainability may be problematic, and early intervention to prevent deterioration of physical health is likely to be more successful.8
The Lester Resource, was co-produced by NHS England, NHS Improving Quality, Public Health England and the National Audit of Schizophrenia Team to assist physical health care for patients with mental health problems.10 The same parameters are now linked to a Commissioning for Quality and Innovation (CQUIN) payment, aiming to improve the assessment, documentation and actions taken on cardiometabolic risk factors in patients with psychosis. CQUIN Mental Health Indicator 4A was first rolled out across inpatient services, and then for Early Intervention (EI) in Psychosis Teams in 2015-16.5 Building on the success of this scheme, the CQUIN has now been extended in 2016-17 to include all patients with psychosis, so adding the requirement to be extended for those patients treated not only as inpatients and in EI teams, but also in community mental health teams.11
We aimed to develop a system to improve physical health checks, reduce cardiometabolic risk and develop consistent recording of this information in our electronic patient record system (Rio). We included more stringent checks than those required by the CQUIN; namely ECG, additional blood tests (FBC, U&E, LFT, TFT, prolactin and CK) in accordance with local policy12 and supported by national guidelines13 and drug manufacturers Information (Summary of Product Chacteristic's). Some teams have relied on psychiatric doctors' input and struggled to produce sustained improvements.14 Common barriers to management of physical illness in patients with severe mental illness are poor engagement and lack of training of mental health professionals.15 Some suggestions to improve care include using algorithms and monitoring tools, educating and training staff, and bridging the gap between physical and mental health to promote a policy of coordinated and integrated health care for persons with serious mental illness. There is evidence that co-locating physical and mental healthcare is beneficial. It has been shown that the most successful systems for improving physical health care of patients with serious mental illness are those where physical and mental health care is integrated.16 Findings to date are that the key determinant of success in integrated systems is clear accountability of care, over and above who and which service provides the care.17
Baseline measurement
A pre-intervention audit was carried out in order to assess the scale of the problem, to establish whether patients on the Early Intervention for Psychosis Caseload were being correctly monitored in accordance with guidelines. These standards were derived from the Royal College of Psychiatrists adaptation of the Lester Guidance,10 as well as the inclusion of additional blood tests and ECG's recommended in local12 and national guidelines13 and drug manufacturers recommendations.
Since different health checks require specific skill sets, operators and equipment, we grouped the checks into the following 3 distinct domains – physical health check, blood tests and ECG (Table 1).
Table showing the three domains of physical health checks performed.
The data was collected by the authors by review of the patient electronic record (RiO). The authors reviewed the progress notes, uploaded documents, core assessment, and care plan sections of RiO. Progress notes were reviewed using the search function. Additionally, the blood result reporting system (ICE) was reviewed for blood results if these were not available on RiO. In order for domains to be scored as completed the authors accepted results documented anywhere in these sections of the electronic systems. The capacitous refusal by a patient for a check was also recorded as completed. Results were documented in an excel spreadsheet.
All patients on the caseload at that point in time were included as it was assumed that their diagnosis was of psychosis, regardless of whether they were being treated with psychotropic medication or not.
We planned to collect the same data after each subsequent intervention phase using the same method of reviewing the RiO and ICE systems.
Baseline measurement:
Baseline data was taken on 18 March 2015 (N = 79). No patients (0%) had a completed physical health check, 6.3% of patients had blood tests, and 3.8% of patients had an ECG, with none having more than one of these three areas completed.
Design
Having identified a lack of physical health checks, we decided to offer the following interventions and evaluate the success of each phase.
Phase 1: Tools and awareness:
19 March 2015 - May 2015
The intervention during phase one was the addition of two junior doctors to the team, where previously there were none. Both junior doctors had previous experience of promoting and auditing physical health monitoring of patients with psychosis and were aware of the inpatient CQUIN. We designed a comprehensive physical health monitoring tool adapted from the Lester Guidance that could be printed onto one side of A4 paper. This ensured that all appropriate checks were included, and offered guidance about normal ranges and appropriate interventions if any abnormalities were found. We also raised awareness of the need for physical health monitoring for all patients on the caseload and encouraged team members to use the tool. There was no other specific intervention performed during this time. Please refer to supplementary file Figure 1: Physical Health Monitoring Tool for details of the tool.
supplementary Figure 1: Physical Health Monitoring Tool for details of the tool
Phase 2: Mobile physical health clinic:
May 2015 - 22 June 2015
A clinic in the outpatient department had been trialed within the team previously with little success, as patients had struggled to attend for appointments. Therefore, a mobile physical health clinic was established to allow patients the choice of being seen either at the outpatient base or in their own home. Clinics ran as dedicated half-days with one doctor and one nurse. The necessary equipment was purchased and stocked in a portable bag. This included blood taking equipment and a sharps bin, weighing scales, tape measures, BMI charts, an automatic blood pressure machine, and our physical health monitoring tool. Since the cost and practicality of including an ECG machine in this mobile clinic was prohibitive, ECG's were requested from GP surgeries.
Our objective was to increase the proportion of patients with completed physical health assessments, highlight unaddressed health needs, offer interventions where appropriate, and improve the recording of physical health on RiO.
Phase 3 consisted of postal requests sent on 23 June 2015 and was evaluated in 2 groups:
Part 3A: Postal requests to patients and GP for new referrals:
23 June 2015
For patients newly referred to the Early Intervention in Psychosis Service, letters were sent to both the patient and their GP requesting the full baseline physical health assessment. 5 patients were included in this phase, which represented all patients undergoing an initial assessment with the team at that time.
Part 3B: Postal requests to existing patients:
23 June 2015
Letters were sent directly to 16 other patients (but not their GP's) already on the caseload who had not been part of the mobile physical health clinic in Phase 2. Attempts would have been made to contact these patients during Phase 2, however, it would have not been possible to arrange a mutually agreed appointment with them. By definition, therefore, these patients were likely to be the more difficult to engage.
Phase 4: GP letter, nurse-led clinic, manager reviews & prompts to care coordinators
2 August 2015- 18 March 2016
Following the authors' departure from the team in August 2015, the team manager was keen to keep up the momentum for physical health monitoring, with the added incentive of pending CQUIN monitoring. All patients' GPs were sent a physical health check request letter, and the physical health mobile clinic continued led by a permanent psychiatric nurse on the team who was phlebotomy trained. The team manager and administrator performed regular reviews of the caseload with reminders to care coordinators where checks or care plans were not completed.
Strategy
We collected data in line with “Plan Do Study Act“ approach to establish the number of patients included in each phase who had each domain completed.
We studied the entire caseload at baseline, after phases 1 and 3, and for Phase 4. We studied the intervention groups after phases 2, and 3.
Results
Baseline data was taken on 18 March 2015 (N = 79). No patients (0%) had a completed physical health check, 6.3% of patients had blood tests, and 3.8% of patients had an ECG, with none having more than one of these three areas completed.
Phase 1: Tools and awareness
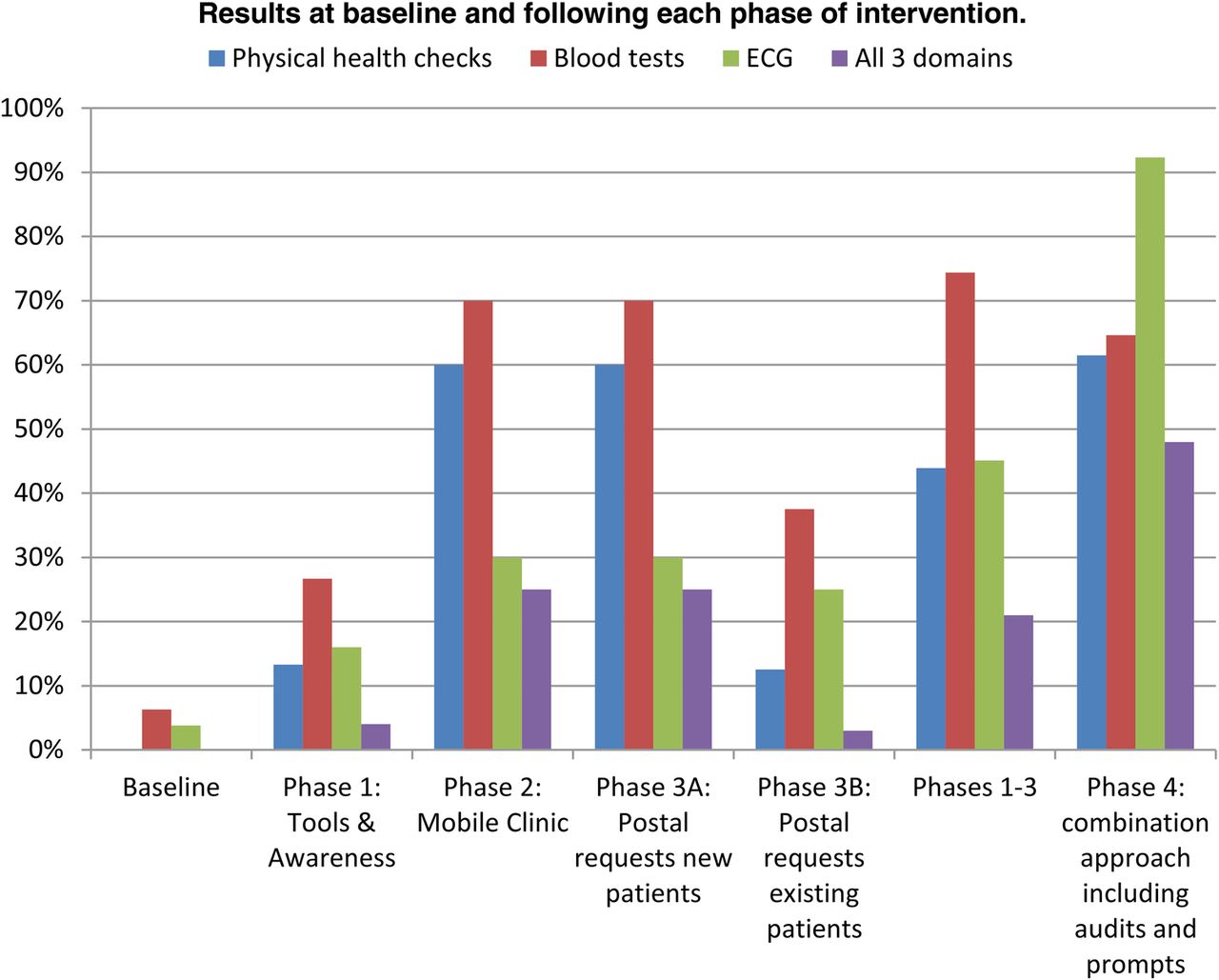
A review of the caseload in May 2015 (N = 75) revealed that increased awareness, tools and increased medical input to the team had improved results. Patients with fully completed physical health checks improved from 0 to 13%; fully completed blood tests 6% to 27%; ECG 4% to 16%, with all 3 domains completed 0 to 4%. Despite this improvement, we felt that these results remained inadequate for an Early Intervention in Psychosis Service, given the protected caseload (low ratios of patients to professionals compared with standard mental health teams) and specific client group.
This demonstrates that an increased awareness and education does lead to some improvement, but is insufficient in producing adequate improvements.
Phase 2: Mobile Physical Health Clinic:
20 patients were given mutually-agreed appointments in the physical health clinic. 4 patients did not attend for their appointment, and 1 patient attended but declined the assessments. This phase was labour intensive, but for the 16 who attended or were visited there were high rates of completed physical health monitoring.
Of the patients who attended mobile physical health clinics, 60% had fully completed physical health checks; 70% had fully completed blood tests; and 30% had an ECG performed. 25% of patients had all 3 domains completed.
If the patients who did not attend are included in the data analysis, then this lowers the completion rate of physical health assessments to 48% for physical checks, 56% for bloods, and 24% for ECGs.
The reliance on GP surgeries to perform ECGs may explain their relatively low completion rate. One might expect for the completion rates of physical health checks and blood tests for the patients who did attend to be 100%. Evidently this was not so, and the authors propose that this reflects that even clinicians involved in this project with their high awareness of the required checks were liable to forget some of the many fields.
Phase 3- Postal requests
Part 3A: Postal requests to patients and GPs for new referrals for this small sample of 5, produced good results for blood tests (80%), but poor results for ECGs (20%) and physical health checks (0%).
Part 3B: Postal requests to 16 existing patients yielded improved monitoring compared to baseline, but failed to reach even half the sample in any domain (13%, 38% and 25%).
Cumulative end results (post phases 1-3)
The entire caseload of 82 patients was reviewed on 1 August 2015 to evaluate the cumulative effect of phases 1-3. This showed an improvement in physical health care overall, with an improvement from 0% to 43.9% of the caseload having fully completed physical health checks; an improvement from 6.3 % to 74.4 % of the caseload having fully completed blood tests, and an improvement from 3.8 % to 45.1 % of the caseload having ECGs. Overall, 21% of patients had all three domains completed. The most successful area of intervention appeared to be around blood tests, with ECGs and physical health checks remaining at less than half the caseload.
Phase 4 – GP letter, nurse-led clinic, manager reviews & prompts to care coordinators
On the 18th of March 2016, the entire caseload of 65 patients revealed the most successful results, with 48% of all patients having fully completed health checks (assessment, bloods and ECGs). 61.5% of patients had fully completed physical health checks, 64.6% had full blood tests, and 92.3% had ECGs. This represented sustained improvement. 12.3% had no domains completed, 24.6% had one domain completed, 27.7% had two domains completed, and 47.7% had all three domains completed.
Please see,Figure 1 Figure 2 and supplementary file Table 2.
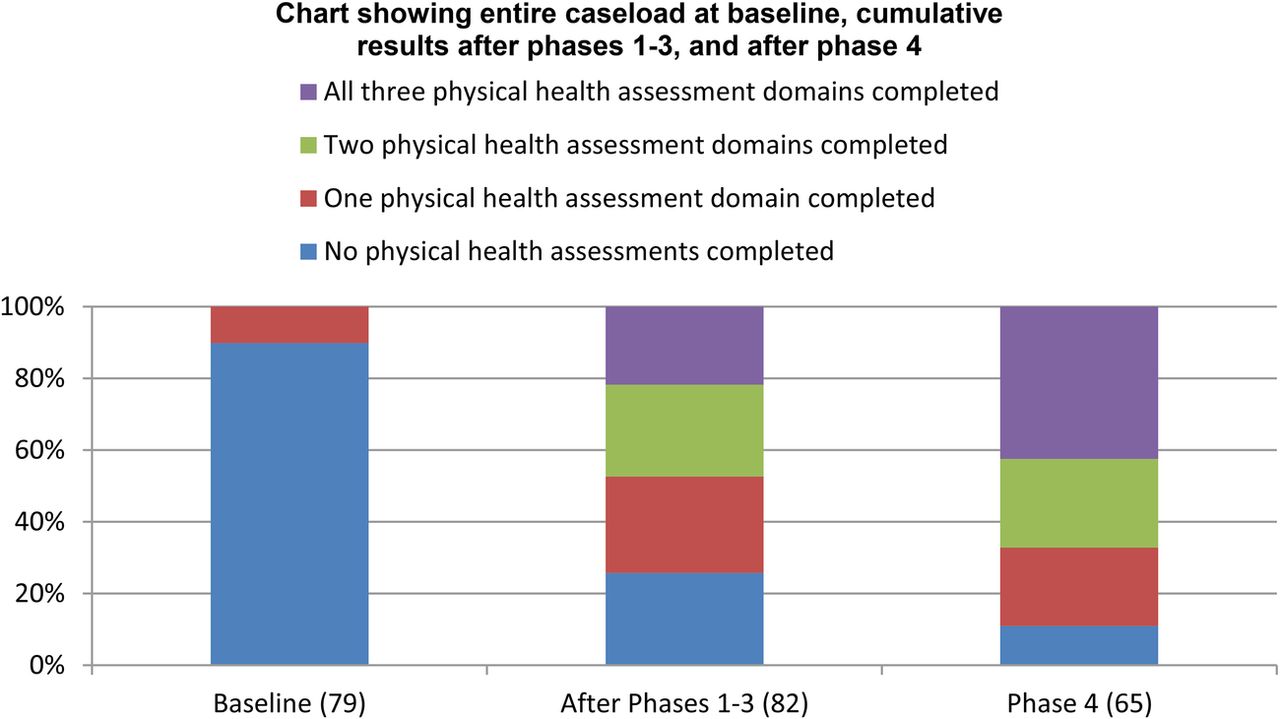
Chart showing entire caseload at baseline, cumulative results after phases 1-3, and after phase 4

{kind=link}
{kind=link}
Results at baseline and following each phase of intervention.
supplementary Table
Time impact of the mobile physical health care clinic:
All appointments were conducted by a psychiatrist and a psychiatric nurse and were scheduled to last thirty minutes; however, it is estimated actual time spent was between 1-4 hours per patient. The additional time was composed of related tasks, including phoning the patient to book the appointment, checking records for previous results, travel time, updating the electronic patient record, acting on abnormal results, and liaising with relevant other parties including GPs. During this time the doctor and nurse were unavailable for other clinical duties. If these duties were carried out by a speciality doctor at £38 per hour,18 alongside a Psychiatric Nurse at approximately £15 per hour,18 one could estimate that 1-4 hours spent on physical health check would cost between the range of £53-£210 per person. In our case, there were 2 junior doctors on the team, therefore the bulk of additional costs were met through NHS England. However, junior doctors are not consistently attached to the team. We did not have additional training and funding available, therefore relied on existing staff resources.
One possibility for reducing the cost of the mobile physical health clinic would be for the non-medical members of the team to be trained in phlebotomy. It costs in the region of £400 to achieve a certificate of competency in phlebotomy.19 This would allow two non-medical members of staff to run the clinic, costing between £30 and £120 per patient if these members of staff were both registered mental health nurses; cheaper still if one were a mental health support worker.
Additionally, the early detection of physical health complications amongst this at-risk population may reduce future costs. A similar initiative aiming to detect people aged 40 to 74 who have or are at risk of cardiometabolic and vascular disease in primary care (The NHS Health Check Programme)20 has been found to be very cost-effective, with the cost per quality adjusted life year being just £2142.21 The programme is particularly successful in the detection and treatment of hypertension, hypercholesterolaemia, and obsesity.22
It is difficult to estimate the time taken by the team manager and administrators on this project, but this was significant, as it involved large amounts of time checking on results, alerting team members where checks were missing, and keeping it a priority in individual's minds. This time will have come at a cost of prioritising over other tasks, which may have included other clinical tasks.
The team were successful in achieving 95% compliance to CQUIN targets, therefore the financial costs of implementing the project were recouped due to this significant CQUIN payment. However, the authors believe it is important for physical health monitoring to be embedded into the running of the service, regardless of CQUIN awards.
Lessons and limitations
Our objective had been to improve the physical health care for patients in the community under the BaNES Early Intervention in Psychosis service. We were able to bring about improvements, with much time, effort and passion. All involved in the project remain concerned about the sustainability of the success, due to time pressures and conflicting priorities when managing a complex group of patients, often difficult to engage.
The CQUIN created an important incentive, adding to the priority that this project was given by the whole team, and with this level of input, our results were good. Our concern remains that if the financial incentive had not been there, such an improvement in outcomes would not have been achieved. It is difficult to know how successful our interventions would have been if the financial incentive had not been in place. The CQUIN has been extended this coming year to include all patients with psychosis, which adds the group in general community teams to the target group as well as those in Early Intervention teams and on the wards. This will be an even more challenging group to reach, without additional systems in place, given higher caseloads of each professional.
We felt the time inputted into achieving these results was significant, and that psychiatrists may not be the most cost-efficient way to achieve physical health checks. It is also difficult to maintain overall responsibility for patients' physical health when this is overseen by junior doctors who rotate every 6 or 12 months, and are not consistently attached to the team. This does not appear to be a sustainable or efficient system.
An additional critique of this project and the outcomes measured, were that success was defined by recording a physical health parameter, rather than providing an appropriate intervention leading to an improvement in this parameter (for example a reduced alcohol intake following brief motivational interviewing, reduced BMI following healthy eating advice, or change of antipsychotic leading to reduction in QTc or weight loss). It was often necessary to refer on to primary care, since many of the interventions were outside the training or confidence of team members, given the varying backgrounds of team members. This added further inefficiencies to our system, but this was not directly measured. It may be that team members giving lifestyle advice was not effective in bringing about meaningful changes. A more effective measure of success may be to measure improvements in parameters, rather than just the documentation of such parameters.
Particular challenges were time, motivation to sustain attention towards physical health, patients who have poor engagement, and the “At Risk Mental State” group, who are not prescribed antipsychotics and for whom it is more difficult to justify the need for tests such as bloods. There was also some difficulty in obtaining ECGs. One GP surgery refused to do them, and there was no one suitably trained on the team to interpret results if not done by a GP.
Ideally, physical health care would be provided seamlessly and efficiently by all team members, and acted on at the time of discovery. Such an approach is hard to achieve in a multi-professional Early Intervention in Psychosis Team, most of whom have little experience of physical health care. Furthermore, few will have had phlebotomy training, so doctors were relied upon to perform and interpret blood test results. Other Early Intervention in Psychosis teams have also tried a range of approaches. One team has a dedicated Band 4 Nurse who has responsibility for physical health monitoring across the caseload, and non-medical staff could be trained in phlebotomy, physical health interventions and interpreting blood results.
In order to provide optimal physical health care in this difficult to reach and high morbidity population, the authors recommend trialing the use of a dedicated primary care nurse or approrpriately trained clinician, integrated into the team. This professional would be trainedto deliver effective interventions, including smoking cessation, dietary advice, and cholesterol guidance. Having a dedicated professional in a permanent position would also ensure a good database could be kept.
The authors both have experience of successful long-stay inpatient psychiatric services which function in this way, employing primary care nurses and part time GPs to address the needs of patients. Such services ensure parity of care for patients using mental health services, who would often otherwise struggle to access primary care services independently.
A limitation of this study is that some of the groups were of small sample size, so it may be difficult to draw firm conclusions from the data available. In addition to this, we did not undertake statistical testing to evaluate the validity of our results, meaning that any changes could have been due to chance variations. We however, think this unlikely, since longstanding team members reported very low levels of health checks in the years prior to the interventions.
Another limitation is that we only collected data at certain time points, not as frequently as is recommended in Quality Improvement methodology, for example with run-charts, mainly due to time constraints. This less precise methodology may make it more difficult to be certain of the impact of specific interventions, especially in Phase 4, where there were multiple interventions as well as the external financial incentive (CQUIN). Once the authors moved to different teams (between phase 3 and 4), the authors had limited influence over the approach of the early intervention in psychosis team, and so the project evolved more naturalistically, building on the findings from the earlier phases. Therefore, whilst phase 4 was informed by the previous 3 phases, it was also driven by the necessity to tie in with external financial incentives in a short period of time, resulting in a multi-pronged approach. Therefore, it is difficult to precisely distinguish which specific intervention(s) in phase 4 were most effective in producing change.
Our study may have underestimated the improvements made in phsycial health monitoring, due to our stringent criteria for marking a domain as “completed”. Indeed CQUIN standards were fully met for those patients audited by the end of the time period monitored.
Another limitation of the study is its generalisability of our findings. We were studying an early intervention in psychosis team, with a caseload of around 80 patients and motivated and enthusiastic staff. Some EI teams do not have any doctors on their teams, so would be unable to implement some of the interventions such as responsibility for checking blood test results, and would need to depend either on primary care, or on providing an additional service as we have proposed. In fact, it is likely that if similar aims were made to provide physical health care to patients on larger teams, where staff have larger caseloads and less patient contact time, their capacity to implement the strategies we used would be even more limited.
Conclusion
Patients with severe mental health problems have a much increased physical health burden, and receive poorer physical health care. We cannot ignore this problem, a need which has been recognised nationally and incentivised by CQUIN payments. Using a variety of approaches as detailed above, we were able to improve physical health checks on a large proportion of patients in the early intervention in psychosis team. The most successful approach appeared to be a combination of the mobile health clinics for physical monitoring and blood tests, letters to GPs requesting ECGs, alongside regular reviews of the caseload, and prompts to care coordinators.
Our study builds on previous research findings around poor engagement of mental health patients in physical health care, which may explain why a multi-facetted approach proved more successful, providing a range of acceptable options for patients to access. One of the key determinants of success of our project is likely to have been around keeping physical health issues on the agenda for the team, as well as providing a system where patients could have their checks. Given the resources and time necessary to produce the changes we saw, we believe engagement and motivation of the whole team is key. In our project, team and managerial engagement and motivation around physical health was high not only due to increased awareness and understanding, but also enhanced by the financial incentive of the CQUIN, where payments are linked to success in audit. Our project suggests that when aligned with team priorities, financial incentives continue to be an effective way to enhance change.
An alternative solution may be to employ trained staff whose role would be to monitor, record, and provide appropriate interventions and signposting for physical health. Such an approach is likely to be more sustainable, reliable, and cost effective, than relying on mental health professionals to deliver this care, and we propose a pilot of this to be tried in such a setting. As recommended in the literature, alternative models could co-locate mental health appointments within GP practices, thereby providing an automatic link in with appropriate services.
Whilst this project focused on the BANES early intervention in psychosis team, other teams in different environments (for example Recovery Teams) are likely to find similar issues. Further studies and pilot projects would be useful in determining cost-effectiveness of certain approaches, and would ideally be linked to meaningful improvements in physical health parameters, rather than completed checks.
Acknowledgments
Dr Richard Stanton (Consultant Psychiatrist), Elena Ely (Bath and Northeast Somerset Early Intervention in Psychosis team manager), Berni Crowley (registered mental health nurse), Michelle Mogg (registered mental health nurse), Bradley Phelps (registered mental health nurse), and Dr Clare Trevelyan (Psychiatrist).
Footnotes
Declaration of interests Nothing to declare for either author.
Ethical approval Ethics approval was not required for this quality improvement project. Avon and Wiltshire Mental Health Partnership refers staff to the National Research Ethics Service's “Defining Research” document. According to this document, this project would be exempt from needing ethics approval as it concerns itself with service evaluation, the data collected was that which should be collected as part of usual care, and likewise all interventions fell within the category of usual gold-standard practice.