Article Text

Abstract
It is imperative that primary care referrals are directed to the appropriate secondary care service. Patients presenting to a primary care physician with ENT conditions may require review in an Emergency Clinic. The latter clinics provide patients with rapid access to secondary care, for urgent, yet non-life-threatening conditions. In our department, we noticed that patients with conditions inappropriate to the capabilities of the Clinic were being booked in or reviewed too late; thus causing wasted journeys for the patient. We conducted a Quality Improvement Project to improve the efficiency of the referral process. A prospective evaluation of referrals was collected continuously over a two-month period. Overall, 5 domains were deemed crucial to enable timely and accurate booking of patients to clinic: booking date, urgency, legibility, patient identification and appropriateness. Our proposed standard set for this project was 100% compliance over the 5 domains. Three separate interventions were instigated following the first cycle. The main components of the intervention were the phased development of an electronic referral system and an educational initiative for junior doctors.
20 referral forms were analysed during the initial 3-week period. No referrals met the recommended overall compliance standard of 100% (mean number of domains achieved: 3.38; standard deviation (SD): 0.637). Legibility and patient information were included in 21% and 30% of referrals, respectively. There was a trend of improvement following initiation of interventions. The mean number of domains achieved was 4.27 (SD 0.647; n=13) in the second data collection period, 4.53 (SD 0.514; n=16) in the third, and 4.75 (SD 0.452; n=24) in the fourth. Using linear regression, this change demonstrates a statistically significant improvement (p<0.001).
An e-Proforma referral system represents a safe and efficient communication technology. When implementing policy change, it is crucial to acquire managerial and consultant support.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The primary-secondary care interface is a key organisational feature of the NHS such that General Practitioners (GPs) act as the gatekeeper between primary care and referral to hospital specialties.1 In the current financial climate faced by the NHS, it is imperative that patients who are referred to secondary care are streamlined for review by the most appropriate clinician in the most appropriate setting. The ear, nose and throat (ENT) Emergency Clinic is a valuable resource in which patients are referred to obtain advice on diagnosis, management or obtain a specialist procedure of urgent ENT conditions. Prior to this project, there was anecdotal evidence that the availability of such emergency clinic appointments was limited and demand was high. Often the clinic was overbooked with complex patients who were unsuitable for junior ENT trainees with a result of clinics running behind schedule. Therefore, to continue to run an effective service, the department felt that it was imperative that this resource was updated to create a streamlined and appropriate system.
The project was conducted in the ENT department of a busy tertiary referral hospital in Cambridge, serving a population of over 500,000. The clinic is led by senior house officers (SHOs); who are either foundation year doctors, clinical fellows or core trainees. At the time of conducting this project, only two of the SHOs had any prior ENT experience. It is important to state that whilst the clinic is led by SHOs, there are more senior ENT doctors in adjacent rooms for advice and practical help if required.
The pre-existing referral system consisted of a hand-written referral which was faxed to the booking office. The office highlighted issues with the referral system, as referrals that were illegible or lacked patient details were often received. This resulted in an inefficient and unsafe service, leaving patients with an inappropriate appointment date for their condition or those who it was not possible to contact. Improving the efficiency of the referral process was seen as a necessary adaptation to streamline the service. The aim of the project was twofold. Most importantly, it was deemed necessary that all aspects of referral information should be correct to enable identification of the patient and ease of contacting them with an urgent appointment. Therefore, the first aim was to improve the accuracy of referral information to 100% by targeting the faxed referral form. Secondly, to ensure that appropriate patients were being booked into the clinic, we aimed to achieve an appropriate patient acceptance rate of 90% by targeting SHO triage. The project was conducted over a two-month period.
Background
Outpatient consultations constitute a significant proportion of an otolaryngologist's workload. Timely access into the most appropriate clinic is critical to ensure high quality patient care. Certain ENT conditions require urgent evaluation to avoid unnecessary admissions and prevent complications. These conditions include acute otitis externa, recurrent epistaxis, removal of foreign bodies (although batteries are an absolute emergency) and assessment of nasal bone fractures. Many UK ENT departments provide a one-stop clinic which provides an interface between GPs, the Emergency Department (ED) and ENT: the ENT Emergency Clinic.
Provision of assigned appointments to patients (rapid access), as opposed to open access clinics, have been shown to improve the effectiveness of an ENT Emergency Clinic.2 ,3 The time-sensitive nature of rapid access clinics requires effective communication between GPs, ED and ENT to provide an effective and patient-centred service. Poor communication when referring a patient to a rapid access clinic is an important quality and safety issue.4 In many departments, the initial referral request is received, triaged and booked by the junior ENT doctor in conjunction with the bookings office. Failure to communicate effectively can lead to confusion, delays in service provision and ultimately a negative impact on patient care.
A recent systematic review evaluated interventions to improve the quality of outpatient specialty referral requests.5 Three common interventions were analysed. The first, software-based interventions, showed significant improvements in all three studies. Electronic communication systems are being introduced into many healthcare organisations and are seen as one mechanism by which the NHS can become safer and more efficient.6 The second, template/pro-forma interventions, showed improvement in four studies but these improvements were either variable or did not evaluate the improvement for statistical significance. The final group, educational interventions, consisted of four studies; two illustrated an improvement in outcome whereas two did not show any difference.
Baseline measurement
Prior to commencing the study, a mapping exercise of the patient referral pathway was developed to identify the stages of the booking process (Figure 1a and 1b). Data was collected prospectively over a continuous two-month period with interventions introduced in a staggered format throughout the study period. All referral forms during the time period were included in the study. There were no exclusion criteria. The first three weeks constituted the baseline measurement.

The facilitators of the improvement project evaluated referral forms which were analysed for content. In consultation with the booking office, five domains were deemed fundamental per patient to enable timely and accurate booking of patients to clinic. These domains were date of referral, urgency or desired appointment date, legibility, two patient identifiers and appropriateness of referral. Each domain was scored as 0 (not achieved) or 1 (not achieved) to create a maximum total domain compliance score of 5. Mean total domain compliance (maximum score 5; standard deviation, SD) and individual domain compliance rates (%) are presented. Data collection periods were analysed for statistical significant (p<0.05) using linear regression. Data were analysed in Prism 7.0 software (GraphPad Software Inc., San Diego, CA).
In the first three weeks of the project, mean total domain compliance was 3.38 (standard deviation 0.637; n=20). No individual domains met the compliance standard of 100% (Date of referral 79%; urgency 80%; identifying information 30%; legibility 21%). The baseline appropriate patient acceptance rate was 82%.
Design
The team was composed of a physician champion, the departmental manager and the booking office secretary with support provided by departmental Consultants. The schematic developed prior to the project (Figure 1a and 1b) showed different areas of error related to education, the referral information and education. Based on these processing errors, several solutions were proposed for testing using PDSA cycles (Plan, Do, Study, Act). Proposed interventions included targeting the referral proforma to ultimately eliminate all fax referrals, SHO education and to gain support from senior physicians and managers. The latter was included to make the intervention sustainable in the long-term.
First intervention: Introduction of proforma
A proforma was introduced as a simple intervention to prompt SHO-recall of the desired referral information. The proforma included three patient identifiers, contact details, date of referral and timeframe of review. This was completed by hand. There was space to allow freehand completion of the presenting complaint. Following completion, the proforma was faxed to the booking office.
Second intervention: Educational intervention
A teaching session was delivered during the departmental audit day to junior doctors, registrars, consultants and the booking management office. The primary aim was to deliver a teaching session of suitable conditions to junior doctors, including when to escalate management to a senior colleague. Secondarily, a discussion was held over suitable conditions for management in a SHO-led clinic to ensure consistency. These common conditions were added to the proforma to be encircled by the referring SHO. Most importantly, unsuitable conditions were discussed and strategies were developed to re-direct these patients to an elective Consultant-led clinic.
Third intervention: e-Proforma
An e-proforma was developed which was sent directly to the bookings office utilising either the electronic medical records system (for patients already registered with the hospital) or secure hospital email (for new patients). The electronic health record system utilized at our hospital is EPIC (Epic Systems Corp., Madison, Wisconsin).
Strategy
Our overall project aim was to improve the accuracy of referral information to 100% and achieve an appropriate patient acceptance rate of 90%.
PDSA Cycle 1: Proforma
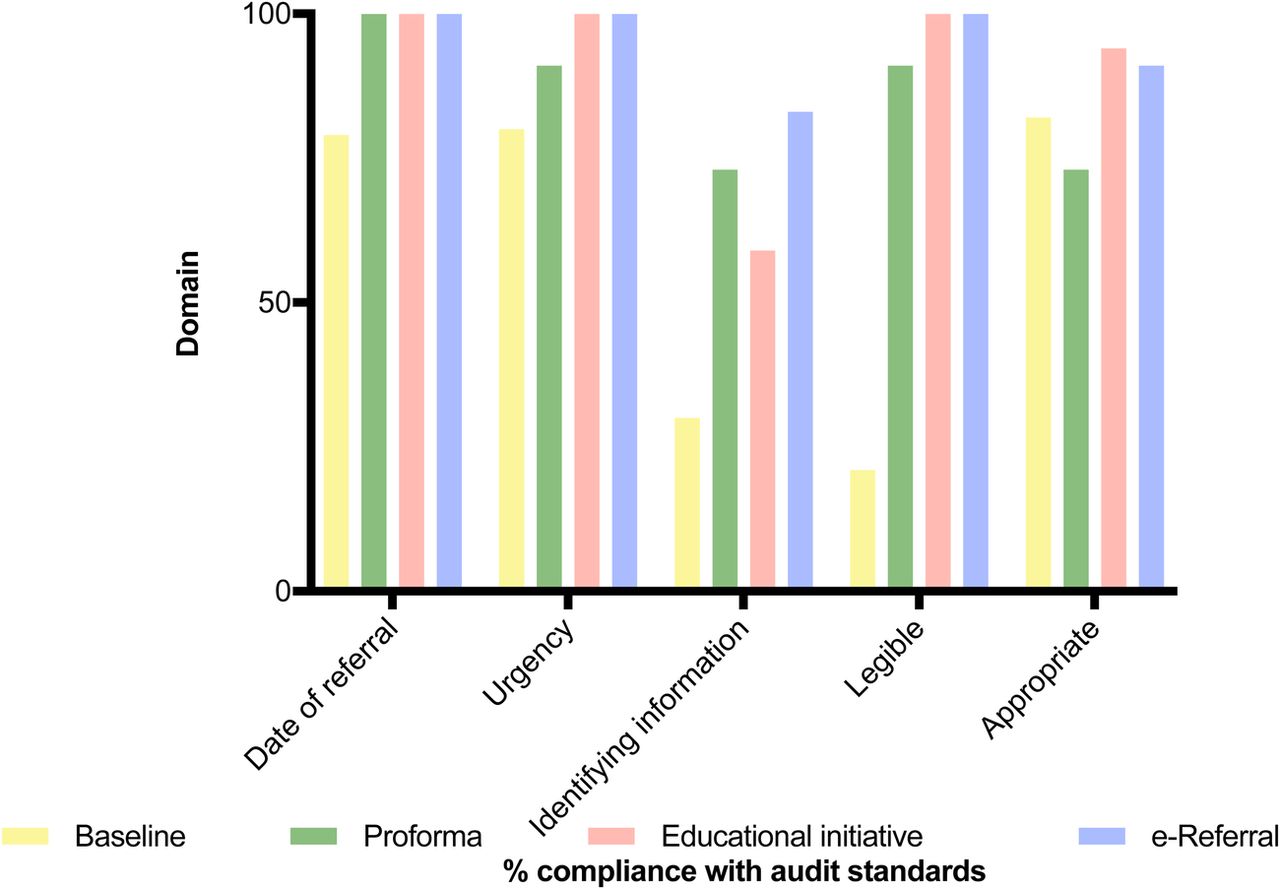
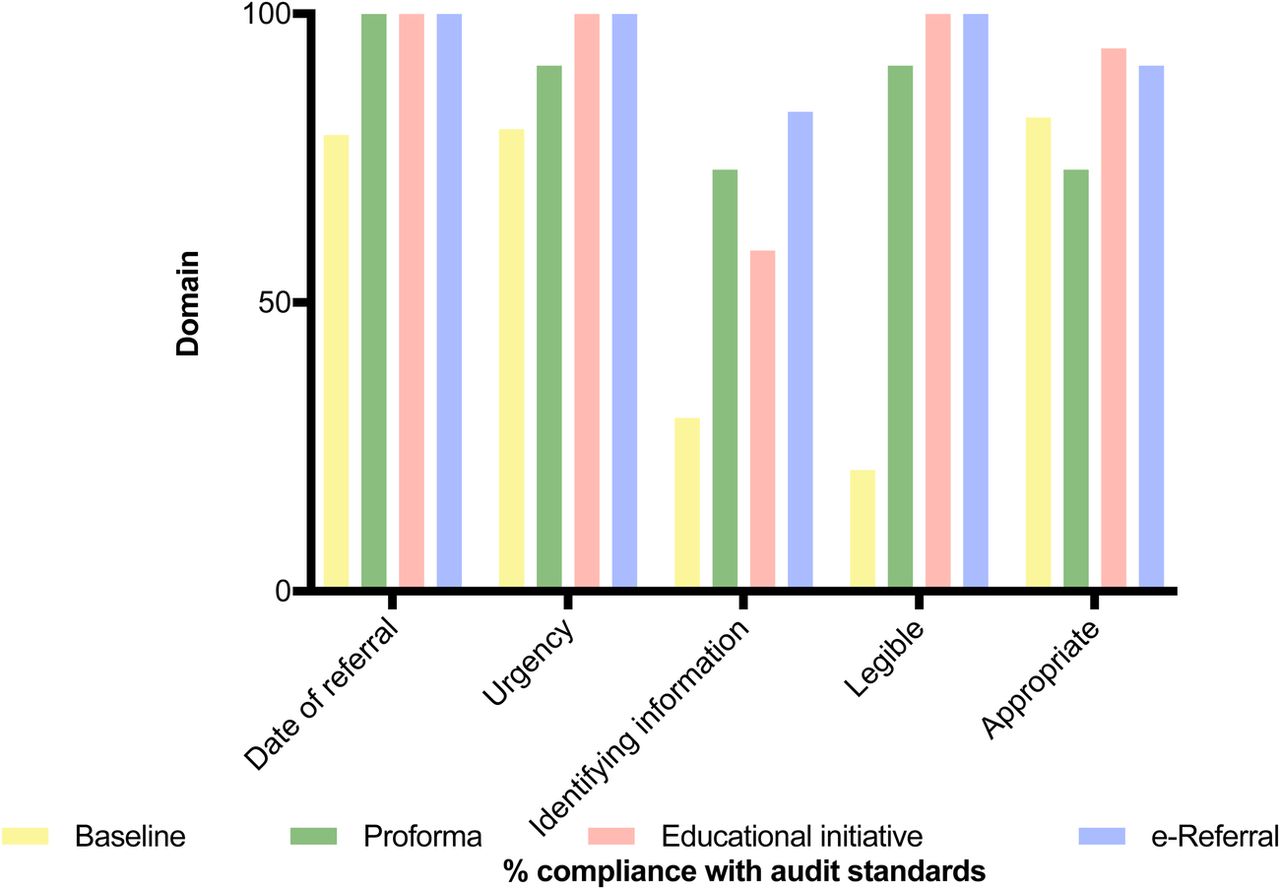
The aim of this intervention was to increase the amount of information provided on referral forms. Improvements were seen in overall domain compliance. Legibility and identifying information showed the most significant improvement; however, there was a reduction in the appropriate patient acceptance rate (Figure 2). This led us to target SHO triage in the next intervention.
PDSA Cycle 2: Educational intervention
The aim of the second intervention was to improve the appropriate patient acceptance rate. This intervention achieved an improvement in the appropriate acceptance rate. Feedback following this intervention was that the teaching session had been useful but that the fax referral system was still causing problems for the booking office due to poor handwriting.
PDSA Cycle 3: e-Proforma
The aim of the third and final intervention was to change the delivery method from written referrals sent by fax machine to an electronic system. This intervention improved identifying information by 176%. Of note, there was 100% compliance in those patients referred using the electronic health record system. At the time of completing the project, it was not possible to use EPIC for new patients as physicians are not permitted to register new patients as it requires extra training. Therefore, this referral system was implemented as a standard.
Results
73 referral forms were analysed during the course of the study period. No forms were excluded from analysis. The majority of patients were referred with otological conditions (73%; n=53). This is of importance for senior ENT clinicians who might be responsible for inducting new SHOs every 4–6 months. Given the preponderance for otological conditions, we need to direct teaching more towards otology and microsuction competence.
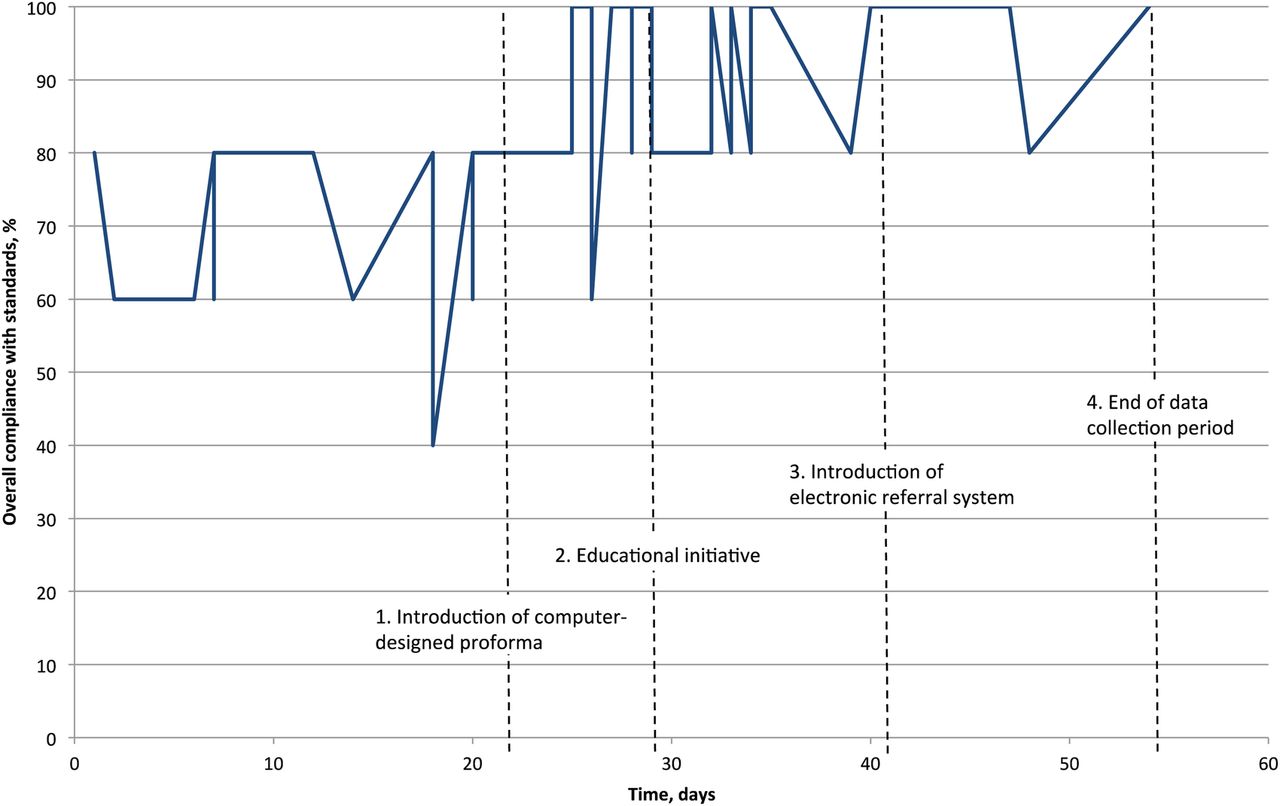
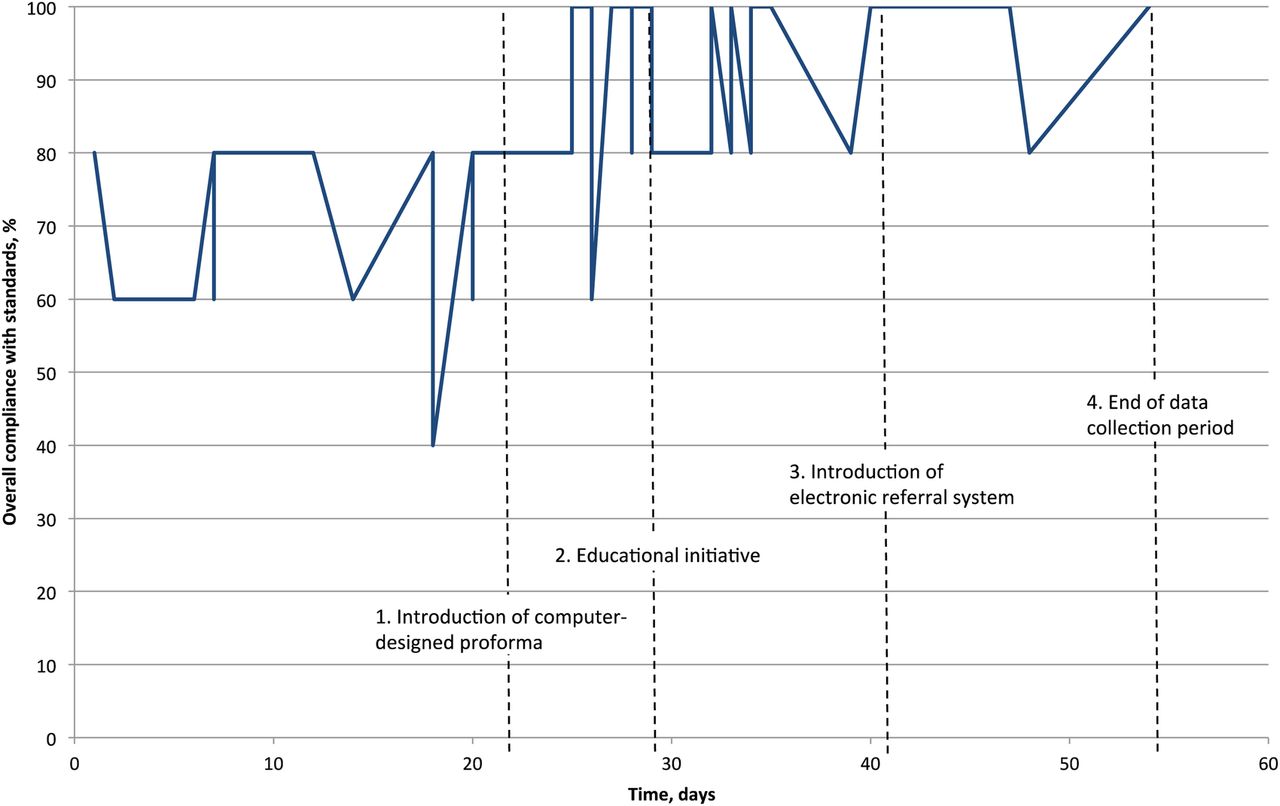
During the initial collection period (n=20), no referrals met the recommended overall compliance standard of 100% (mean 3.38; SD 0.637). During subsequent data collection periods there was a trend of improvement following implementation of interventions (Figure 3). The mean number of domains achieved was 4.27 (SD 0.647; n=13) in the second, 4.53 (SD 0.514; n=16) in the third, and 4.75 (SD 0.452; n=24) in the fourth phase. Using linear regression, this change demonstrates a statistically significant improvement (p<0.001).
{kind=link}
{kind=link}
{kind=link}
On analysis of the 5 individual domains, audit standard compliance showed an improvement in all domains (Figure 2). Legibility, urgency and date of referral all achieved the audit standards of 100%. Identifying information showed a statistically significant improvement (30% to 83%, p<0.001). A subset of patients (those referred by EPIC in the final cycle) achieved the standard of 100%. The appropriate acceptance rate achieved the audit standard of 90%.
Lessons and limitations
Interventions for quality improvement require careful modelling in order to maximise potential successes 7. Outcome measure evaluation is of paramount importance to ensure sustainability of the interventions 8. We found the initial task of delineating the patient care pathway from referral to review acted as a helpful goal setting exercise. This schematic identified potential themes for development and allowed the facilitators to introduce targeted interventions and evaluate the outcomes in real-time. Three natural categories of interventions emerged: education, referral information and communication.
ENT junior doctors facilitate triage between GPs and the Emergency Clinic, thus requiring ENT junior doctors to have an appreciation of the limits and aims of the clinic. Effective triage and advice is necessary to ensure patient safety. In the literature, it has been identified that educational resources which are integrated within a clinical setting often stand a higher chance of being successful than a standalone resource 9. Therefore, an educational initiative was developed to be incorporated during monthly departmental teaching and audit sessions. This enabled a wider discussion from consultants and juniors to appreciate the priorities of senior colleagues.
Correct and complete referral information is necessary to ensure accurate and quick creation of clinic appointments. Use of an e-proforma system increases accuracy of patient identification and ease of use. It also creates an easily accessible audit trail so that a referral does not become “lost in transit”. These results are consistent with other studies which improve accuracy of data entry following introduction of a computerised template 10. Advances in electronic medical record technology promise significant advances in patient care 11.
This project highlights the importance of effective communication. At a basic level, communication is seen between primary care, junior doctors, the booking office and patients. However, altering processes that affect referrals from doctors in the community is challenging and requires support from consultants/senior doctors to ensure that these changes are sustainable. The case of the Emergency Clinic is particularly unique due to the expedient nature of clinical problems for review. By examining implementation from multiple perspectives (junior ENT clinician, booking office, senior support), the findings provide information about the priorities of different policy makers and clinicians. It is clear that improving healthcare performance and efficiency requires commitment from all levels of the hierarchy within a team, but in particular, engagement from the most senior member of the team is key. Fitzgerald et al concluded that, even for limited service improvements, ‘distributed change leadership’ is needed, comprising united senior-level support from clinical leaders, managers and ‘willing workers’ in the form of front line clinicians who are prepared to embrace the new way of working.12 Furthermore, with the transient nature of junior doctors rotating through different departments, senior engagement is imperative to ensure sustainability and training for each new set of doctors.
There are a few limitations to our study. Firstly, the interventions were tested over a relatively short time period. This may explain the reason that, despite a significant improvement, two areas (patient information and appropriateness of referrals) did not reach the audit standard of 100%. Future work will look to improve these domains. Secondly, data collection was limited to analysis of the referral information, and does not necessarily reflect accuracy of triage. Finally, it is important that all Quality Improvement Projects are considered within their wider context and takes into account the system as a whole. We must therefore review the numbers referred to non-emergency ENT clinics to ensure that there has not been a spillover effect.
Conclusion
This project demonstrates the power of Quality Improvement Projects in initiating change. The development of an e-proforma using multiple intervention cycles in conjunction with improved communication has proved an effective method of significantly improving referrals to the ENT Emergency Clinic. Senior support is crucial when implementing changes which affect primary care referrals.
Acknowledgments
We would like to acknowledge the help and assistance of the ENT booking team at Addenbrooke's Hospital without whom this project would not have been possible.
Footnotes
Declaration of interests None declared.
Ethical approval According to the policy activities that constitute research at our institution, this work met criteria for operational improvement activities exempt from ethics review. Our project is primarily intended to improve local care, not provide generalisable knowledge in a field of inquiry. We sought only to evaluate the improvements in referrals as a result of auditing and feedback of compliance rates to hospital staff.