Article Text

Abstract
Tracheostomies are predominantly used in Head & Neck Surgery and the critically ill. The needs of these complex patients frequently cross traditional speciality working boundaries and locations and any resulting airway problems can rapidly lead to significant harm. The Global Tracheostomy Collaborative (GTC) was formed in 2012 with the aim of bringing together international expertise in tracheostomy care in order to bring about rapid adoption of best practices and to improve the quality and safety of care to this vulnerable group.
The primary aim of this project was to improve the safety and quality of care delivered to adult patients with new or existing tracheostomies. We implemented changes guided by the GTC using multiple PDSA cycles over a 12-month period. Interventions were across three themes: educational, patient-centred (earlier vocalisation and enteral intake) and organisational. We hypothesised that systematic healthcare improvements would reduce the severity of harm resulting from tracheostomy-related safety incidents and improve surrogate markers of the quality of patient-centred care. Furthermore, we hypothesised that raising the quality and safety of healthcare services would lead to more efficient care, measured by earlier tracheostomy decannulation times and reduced hospital lengths of stay.
This Quality Improvement project implemented the GTC into four diverse NHS Trusts in Greater Manchester. Key drivers implemented included multidisciplinary tracheostomy steering groups, ward rounds and bedside teams, standardisation of tracheostomy protocols, staff education and meaningful involvement of patient and family. Surrogates for the quality and safety of care were captured for all patients using a bespoke database.
Implementing the GTC into four NHS Trusts rapidly and positively impacted on patient safety metrics and surrogates for the quality of care delivered. It is likely that the comprehensive resources of the GTC will be of benefit to other NHS hospitals and indeed other healthcare systems around the world.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Tracheostomies are small tubes inserted into the anterior neck to act as artificial airways for around 15,000 adult and paediatric patients in England and Wales annually.1 Temporary tracheostomies are most commonly performed to facilitate weaning from ventilation in the critically ill or as part of Head & Neck Surgical procedures for airway problems. Patients are increasingly complex and dependent on competent, knowledgeable bedside staff to keep them safe and to provide high quality care. The needs of patients frequently cross traditional speciality and working boundaries and may involve transition into the community. Landmark papers and studies from the National Patient Safety Agency (NPSA)2 ,3 National Confidential Enquiry into Patient Outcome and Death (NCEPOD)1 and others4 ,5 consistently highlight failings in the provision of care for this vulnerable group. In addition to patient-safety incidents, patients and their families identify an inability to vocalise and delays in establishing oral fluid and dietary intake as important markers of the quality of care delivered.
Local context
Four acute NHS Trusts working in partnership in the South Sector of Greater Manchester participated in a tracheostomy Quality Improvement (QI) project funded by the Health Foundation. The sites comprised a 950-bed University Teaching Hospital (the lead site), an 800-bed University-affiliated District General Hospital and two smaller District General Hospitals (Table 1). The two larger sites hosted Head and Neck Surgical Units performing major surgery, with dedicated ENT specialist nursing staff. All ICUs performed percutaneous tracheostomies, with the largest site hosting a supra-regional cardiothoracic ICU in addition to a general unit. None of the sites had multidisciplinary (MDT) tracheostomy teams or ward rounds at baseline and no sites admitted paediatric patients with tracheostomies. Despite previous systematic healthcare improvements focussed on reorganisation of care and education of staff, previously reported local tracheostomy-related patient safety incidents rates were still considered unacceptably high.6
Profiles of the four participating sites. (a) Dedicated Head & Neck surgery on call service 24/7. (b) Baseline pre-project estimates of tracheostomy numbers.
Specific aims
The primary aim of the project was to improve the safety and quality of care delivered to adult patients with new or existing tracheostomies. We implemented changes guided by the Global Tracheostomy (QI) Collaborative (GTC) using multiple PDSA cycles over a 12-month period. Interventions were:
Educational: MDT staff training to increase knowledge of care and familiarity with emergency algorithms.
Patient-centred: introducing patient champions to help guide service redesign, increased referral and input from Speech & Language Therapy (SLT) to facilitate earlier vocalisation and enteral intake.
Organisational: introducing staff champions, establishing MDT care teams and ward rounds, standardising protocols across clinical areas where possible.
Our project used the bespoke GTC database to track patient-level outcomes. We hypothesised that systematic healthcare improvements would improve surrogate markers of the quality of patient-centred outcomes, such as time to first vocalisation and swallowing. We also believed that targeted education and introducing MDT tracheostomy teams and ward rounds would reduce the severity of harm resulting from tracheostomy-related patient safety incidents. Furthermore, we hypothesised that raising the quality and safety of healthcare services would lead to more efficient care, measured by earlier tracheostomy decannulation times and reduced hospital lengths of stay.
As the participating sites were so diverse, we did not set universal targets, but aimed to achieve significant trends towards our improvement goals in the measured pooled data over the 12-months of the project.
Background
Tracheostomies are artificial airways that require good, basic care to keep the airway patent and in the correct place. The classic surgical indication for tracheostomy of actual or potential upper airway obstruction remains, but tracheostomies are increasingly used in the critically ill to facilitating prolonged invasive ventilation, to offer a degree of airway protection against aspiration, or to facilitate gradual weaning from ventilatory support. A number of well-recognised complications can occur, most notably tube blockage or displacement. Delays can occur in detecting incidents if staff are not trained to anticipate problems and appropriate equipment, monitoring and infrastructure is not in place.1–5 Confusion can arise due to the variety of tracheostomy tubes and ancillary equipment available, especially if staff are unfamiliar with airway devices and procedures.
Recurrent themes from national reports have identified deficiencies in trained staff, bedside equipment and the infrastructure required to safely manage tracheostomy patients around the clock, leading to avoidable patient harm, morbidity and mortality.7 Simply requiring a tracheostomy is associated with in-hospital mortality reported from 20-60%8 usually due to underlying illness. However, institutional harm also occurs in patients due to incorrect management of the tracheostomy itself with NCEPOD reporting nearly 30% of tracheostomy patients experiencing a patient safety incident.1 Measurable harm occurs in 60-70% of such incidents, ranging from readmission to hospital or the Intensive Care Unit (ICU), prolonged in-patient stays, hypoxic brain injury and death.2 ,9
The NCEPOD report highlights the need for improvements covering all aspects of medical and nursing care within hospitals and acts as a driver for action in provider organisations. The importance of meticulous on going care of the tracheostomy patient is recognised together with the need for MDT staff to have the competence and confidence to deal with common emergencies.
International exemplar institutions have been able to demonstrate significant improvements in the quality and safety of care by a variety of approaches. These have included forming multidisciplinary tracheostomy teams that regularly review patients10 ,11 the use of checklists,12 service redesign and ensuring key bedside staff have received appropriate education.6 Individual institutions began working together to share their methodologies, inviting international expertise to form the GTC in 2012. This QI Collaborative provided resources and support from a peer network to global sites wishing to improve tracheostomy care, with outcomes tracked and benchmarked by the GTC database.
Whilst individual elements of the GTC programme have been shown to be of benefit in individual sites, implementation of the package of resources and the ability of the database to track and benchmark healthcare improvements in a cluster of sites had not been evaluated.
Baseline measurement
The GTC database is a bespoke international, web-based, secure REDCap™ database, allowing anonymised patient details to be uploaded from the bedside. Protected Health Information (PHI) is not submitted from European countries and a separate local database of demographics and PHI was maintained, linked via a unique GTC patient identifier.
The GTC database allowed us to capture the following qualitative and quantitative metrics:
Patient demographics
Patient safety incident data (reported critical incidents)
Surrogates for the quality of care (time to referral to speech and language therapy)
Patient-centred metrics (time to vocalisation, first oral intake following new tracheostomy)
Measurements were taken continually throughout the project, but specifically captured at baseline and during the three planned PDSA cycles (Table 2). Educational outcomes were collected by surveys of staff groups across the four sites involving a total of 579 MDT staff. Detailed Speech and Language Therapy (SLT) data were collected at the lead site only by the tracheostomy MDT. Organisational metrics from the four sites concerning policy reviews, equipment provision and designated 'cohort' wards were collected by the lead team. Baseline data are presented in Table 2.
Strategy for improvement. PDSA cycle summary. Fishers exact 2-tailed p reported for comparisons.
Local ward-level champions were recruited in all clinical areas where tracheostomy patients would be managed who recorded the details of all relevant patients admitted to those clinical areas. Data were collected contemporaneously and entries were reviewed by the site leads weekly, completing or checking missing fields as required. Pooled data were reviewed every 3 months to ensure records were complete. These records were compared with those of the clinical coding department to ensure adequate data capture and to provide quality assurance.
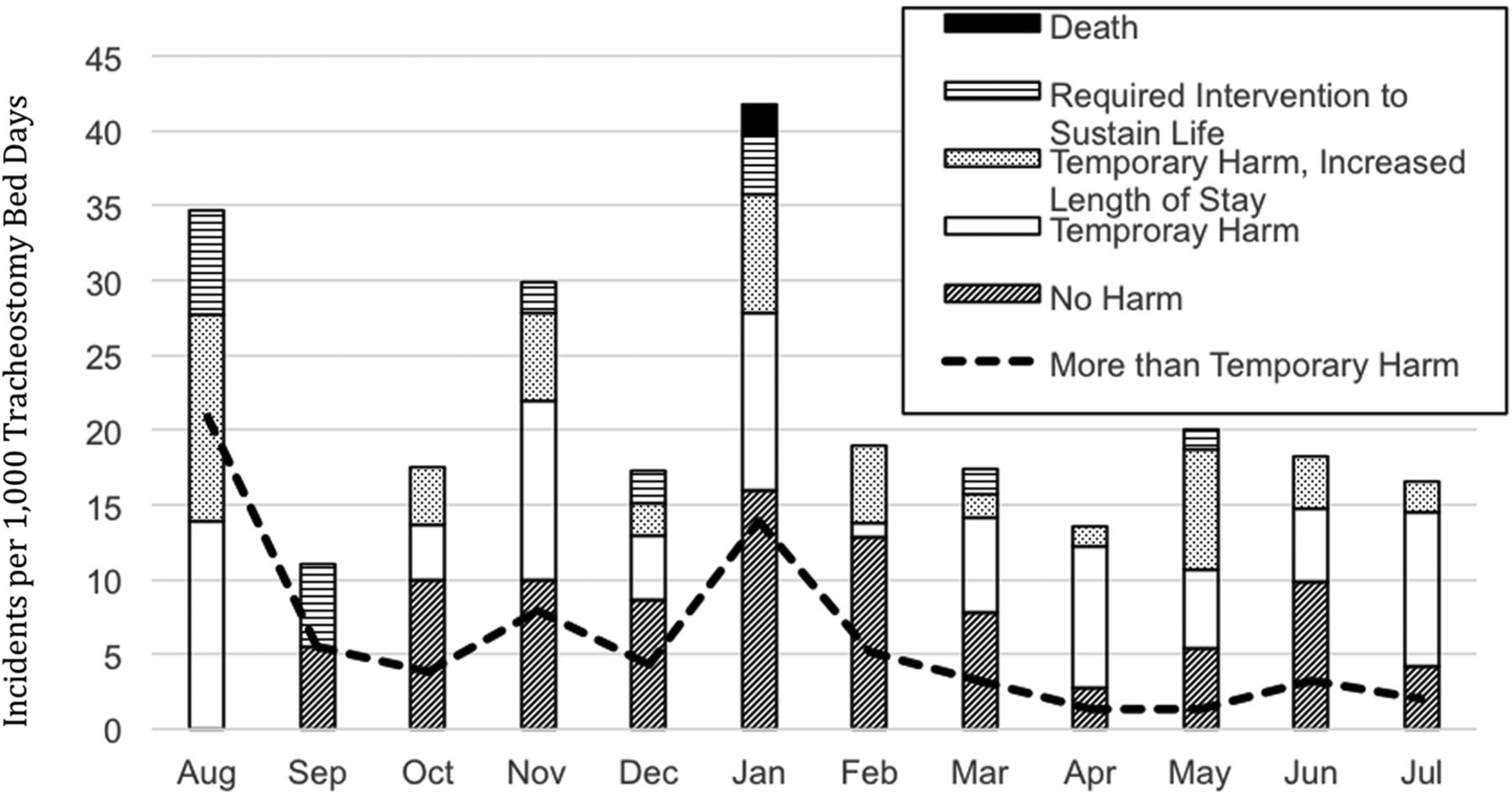
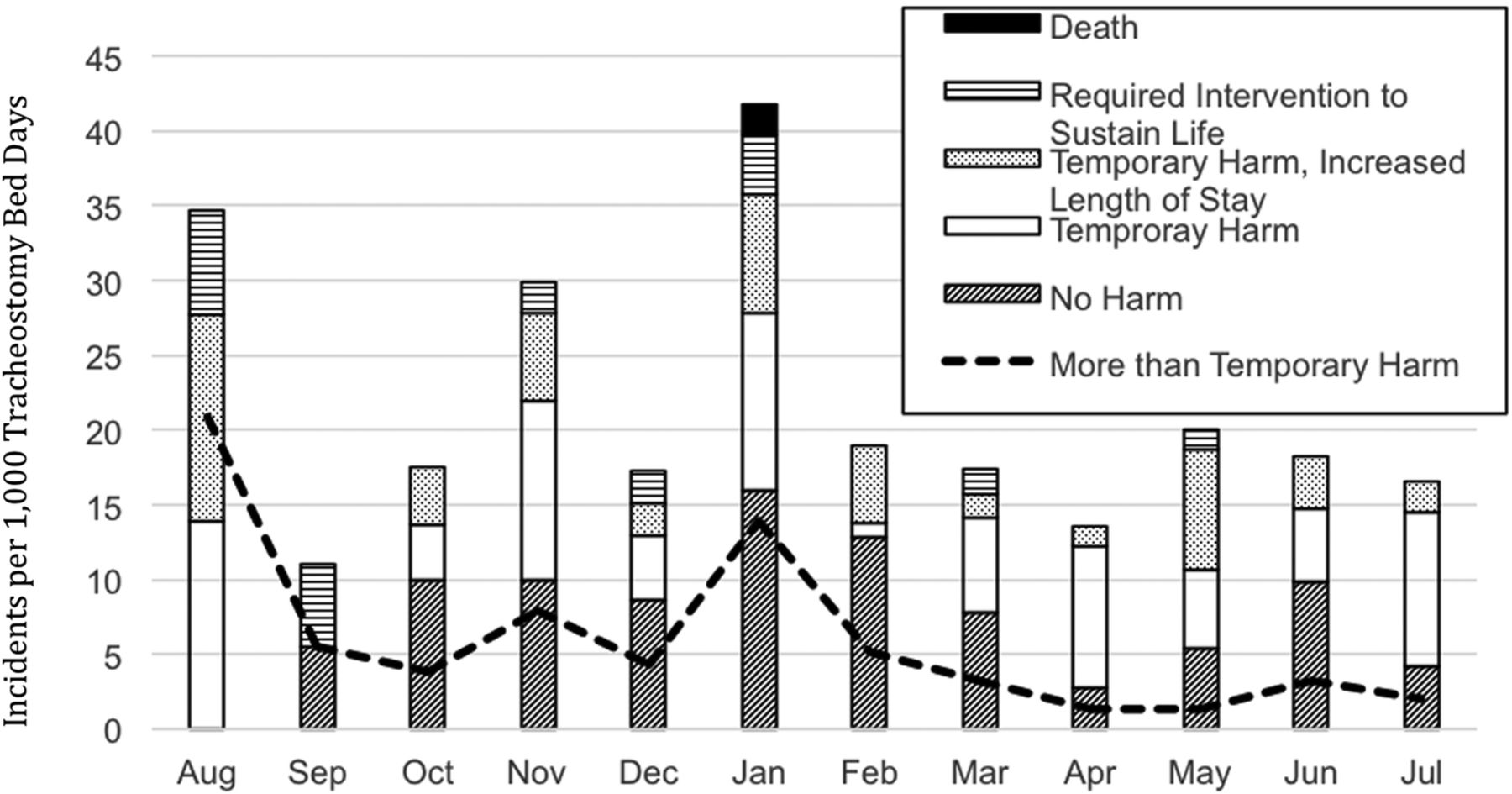
Tracheostomy-related patient safety incidents were reported by bedside staff and reviewed and categorised by the authors using the NPSA critical incident classification system. Incidents could be classified as resulting in no harm, temporary harm, temporary harm with increased length of stay (LoS), requiring intervention to sustain life or contributing to the patient's death. This allowed us to compare our incidents to historical data from the lead site6 and also to national data collected as part of the NCEPOD report into tracheostomy care from 2014.3
Patient-centred outcomes
National reports had identified inability to vocalise and/or eat or drink were the most distressing features of tracheostomy care from a patient perspective.1 Patient and Family focus groups held during international GTC conferences in 2013 and 2014 confirmed this. Some exemplar sites had reported rapid improvements in time to first vocalisation and to commencing oral intake10 leading us to capture these metrics, along with timely to referral to SLT that could reflect patient-focussed outcomes. Baseline data are summarised in Table 2.
Design
Our interventions were guided by the GTC resources, developed by exemplar centres around the world that had demonstrated meaningful improvements in patient-centred care. Our interventions are considered in three categories:
Educational: Building on the resources of the UK National Tracheostomy Safety Project (www.tracheostomy.org.uk) we designed in-house half day teaching sessions to cover practical aspects of tracheostomy care for medical, nursing and allied health staff13. We aimed the resources at staff who would have little or no prior knowledge of tracheostomy care. We anticipated that whilst the sessions might be considered 'basic' for more senior staff, we needed to ensure that basic anatomical, equipment and emergency scenario management was covered. An educational MDT was recruited from simulation departments, ward-based educators and the site leads.
Patient-centred: It was clear from published work10 and GTC resources that all of our patients could benefit from an early referral to SLT14. Staff were sometimes unaware of the roles SLT (and other key allied healthcare professionals such as physiotherapy) could play in the care of patients, especially when it came to communication, vocalisation and swallowing. We used patient videos and feedback during our educational sessions to increase staff awareness, reinforced during MDT ward rounds. We hoped that by demonstrating and celebrating early successes in some patients, we could change the referral and engagement culture amongst ward staff. Demonstrating that tracheostomised patients could vocalise earlier in their treatment helped patient communication with staff and families, reduced anxiety and made care easier. This progress enables patients and their families to start to drive sustainable SLT interventions with ward staff.
Organisational: Exemplar GTC institutions had demonstrated that coordinated care reduced treatment and referral delays and could lead to shorter lengths of stay and cost savings10. Our starting point was to form tracheostomy MDT steering committees at each site with guidance from the lead team. These committees reviewed local existing policies and streamlined and amalgamated these where possible, as duplication and different practices were expected. We anticipated challenges here as what works well for one patient group in one location does not necessarily translate across the organisation. However, we were confident that the principles of MDT care could be incorporated into Trust-wide guidelines. These guidelines would include the provision of important bedside equipment and re-organisation of care such that patients with tracheostomies and laryngectomies were only managed in designated 'cohort' wards. This would allow us to create safe areas within each Trust where education could be concentrated and staff would be knowledgeable, equipped and supported in delivering safe and effective care.
Strategy
Our strategy for improvement was based on repeated PDSA cycles, guided by the GTC resources and the lead team. Our model covered educational, patient-centred and organisational themes outlined above and can be considered as three distinct PDSA cycles, summarised in Table 2.
A key element of our strategy was high-level institutional support and membership of the GTC and participation in this project was approved in writing at executive board level at all participating sites. Recruiting credible local staff and patient champions to lead the project helped to ensure that all MDT areas were included. These were powerful enablers proposed by the GTC and undoubtedly drove the project forwards.
Educational aims were to increase the knowledge and familiarity with emergency algorithms of bedside staff. We started with generic half day training sessions which were voluntary but quickly learned that this approach was not focussed enough. Revisions were made (aligned with organisational changes) to develop tracheostomy 'cohort' wards, allowing the educators to target smaller numbers of staff. Cycle 2 demonstrated that whilst shorter teaching sessions were better attended, the majority of staff wanted access to broader-based resources, leading to e-learning modules being uploaded into Trust mandatory training platforms. Finally, in order to sustainably train all relevant staff going forwards, Trusts were asked to consider making tracheostomy-related training mandatory for cohort wards.
Patient-centred aims were to improve communication, support earlier vocalisation and oral intake through earlier and increased involvement of the SLT teams. Not all sites has SLT established, but our early data helped to develop appropriate business cases to access these vital services. We hypothesised that demonstrating and promoting early successes would improve knowledge and awareness of what the SLT and tracheostomy MDT could offer patients, and powerful accounts from patients describing their communication difficulties were recorded. We played these videos during teaching sessions and relevant audit meetings. Cycle 1 learning led us to reinforce this approach during MDT ward rounds, maintaining the 100% referral to SLT that we had aspired towards. Our final PDSA cycle focussed on the use of speaking valves to aid communication, used as a surrogate for bedside staff being pro-active in addressing communication needs. The use of speaking valves is not indicated in all patients and their use can cause potential problems, meaning our predictions of universal use when appropriate were not realised.
Organisational aims were to standardise as much of the care across diverse locations of the Trusts as possible, reorganising care into designated 'cohort' wards and ensuring universal essential bedside equipment provision. High level institutional support was key in engaging bed managers, surgery, medical and intensive care wards and staff. Historical local incidents were used to provide a contextual case for change, with GTC exemplar institutions used to provide evidence that change was achievable and desirable. Capturing and reporting inappropriately located patients or bed spaces without essential equipment as critical incidents was aided by the MDT ward rounds and was fed back at executive level. Engagement across all directorates was not universal however. Learning and data from the PDSA cycles were fed back locally and used to encourage participation and standardisation where possible and benchmarking between the sites introduced an element of positive rivalry and competition between sites.
Results
Over the 12 month data collection period (1st August 2014 to 31st July 2015) 296 tracheostomy patient admissions were tracked across the four sites with similar demographics to previously reported national data1. There were 87 females and 209 males admitted across the four sites, with a median age of 63 years (IQR 20, range 16-86) with no significant between-site differences, other than numbers of in-patients with tracheostomy (Table 1). No sites reported in-patient care for paediatric tracheostomy patients.
Project leads for each site assessed data quality. Only 67.2% of patient episodes captured by the GTC database were recorded by existing hospital clinical coding methods, providing assurance that the GTC database was capturing accurate, contemporaneous patient records. Where missing data were identified, these were added retrospectively.
A total of 124 adverse events were identified affecting 88 patients (29.8%). The impact of these incidents ranged from no impact (for example; equipment not available at a bedside but no clinical incident occurred) through to one death. Analysis of reported incidents over the duration of the project showed a significant reduction in the severity of harm by month (Chi Square p<0.01, Figure 1). There was also a significant trend towards lower harm categories for incidents over the duration of the project (Chi Square test for linear trend, r= -0.21, p<0.01). Further evidence of change is apparent in staff questionnaires, collected at two sites showing significantly improved understanding and familiarity of emergency algorithms that likely contributed to safer care.
Median hospital LoS across the four sites was 30 days and pooled data were used to calculate monthly median LoS. There was a significant trend month-by-month towards reducing LoS, with median hospital LoS reduced by 6 days over the 12 months of the project (95%CI 9.96-3.96 days). Detailed, validated ICU LoS data was available for one site with 169 patient episodes. ICU LoS reduced significantly over the duration of the project with a median slope of -0.11 (-0.25 to 0). This equates to a reduction in median ICU LoS of 1.3 days over the project.
When considering all patients admitted to hospital during the study period with new or existing tracheostomies, there was no reduction in total tracheostomy days (number of days that patients had tracheostomy tubes in situ). However, for the 214 newly inserted tracheostomies (60 surgical, 99 percutaneous and 55 un-specified, 72.3% of all patients), there was a non-significant trend towards reduced tracheostomy time (median slope -0.05, -0.17 to 0.25).
Patient-focussed outcomes
At baseline, 78% of patients with new tracheostomies were referred to SLT. At the lead site, this increased to 100% by month 3 and was maintained throughout. Successful SLT case studies concerning early use of one-way tracheostomy speaking valves to facilitate early vocalisation were highlighted to relevant staff during educational sessions15. Monthly analysis of the dataset for percutaneous tracheostomies showed non-significant trend toward earlier speaking valve use (median slope=-0.17, -0.83 to 0.4). The time taken to commence full oral diet from date of first cuff deflation also reduced (median slope -0.5, -1.0 to 0) translating into a median reduction of 5 days across the study. Two of the participating sites did not have an inpatient SLT service but though sharing of SLT outcomes, successful service redesign facilitated access to these important services.
{kind=link}
Pooled incident rates per 1000 tracheostomy bed days by NPSA level of harm during the 12-month data collection period.”
Lessons and limitations
Our study has demonstrated that meaningful improvements in the safety and quality of care for patients with tracheostomies in diverse NHS Trusts are possible using improvement methodologies advocated by the GTC. Individual quantitative outcomes such as reductions in the severity of harm associated with patient safety incidents, reductions in time to vocalisation and oral intake undoubtedly contributed to more global measures of impact such as LoS. Qualitative feedback from patients, their families and from staff helped to convey key drivers by framing the problems with a local perspective. Engagement and multidisciplinary participation was driven by feeding back early successes and by demonstrating the effect that interventions could have on system-wide outcomes. We were able to demonstrate significant improvements in the quality and safety of care and reductions in LoS within 12 months, which is unusual for projects of this complexity.
Because of the nature and complexity of tracheostomy patients, it is unlikely that patient safety incidents can be totally eradicated. Whilst there was variation in the numbers of incidents reported, the severity of harm resulting from patient safety incidents over the course of the project to significantly lower levels than that reported by the 2014 NCEPOD report and from an earlier healthcare improvement project in Greater Manchester.6 ,16 Considering the root causes of many such incidents are amenable to simple, prospective improvement strategies (such as staff education, checklists and essential equipment provision) it seems likely that participation in this project directly led to many of these improvements.17 The significant trend towards lower levels of harm over the course of the project supports our opinion that the reduction in incidents is due to improvement rather than reduced reporting.
The variation across the four sites in mean tracheostomy bed days per patient is likely due to local case-mix and differing practices. However, the longer the tracheostomy tube is in situ, the more opportunity there is for potential complications. Reporting incident rates per patient does not take this into account and may result in sites reporting longer tracheostomy days to be unfairly scrutinised when benchmarking. We described our incident rates per 1,000 tracheostomy bed days and this method of presenting incident data may be useful in benchmarking sites with different lengths of stay in the future.
Improvements were not uniform across the four sites, with the biggest changes seen at the lead site. Whilst this site had the largest number of tracheostomy patients and a larger baseline infrastructure, there were also significantly more staff to train and patients were of greater complexity (two critical care units and regional head and neck service). A multidisciplinary team with existing expertise in tracheostomy care commenced detailed tracheostomy ward rounds, providing a different context to the other sites. Local MDT oversight teams were established at all sites, but it took interim reporting of patient-level data to drive engagement and change at the two smallest sites. Due to fewer numbers of tracheostomy patients at these sites, meaningful data took longer to collect. Pre-existing critical incident local data to drive early MDT engagement may be of benefit in planning future projects.10–12 ,17 Setting clear and over-arching organisational goals related to tracheostomy patients likely contributed to enabling change and was key in delivering the multidisciplinary care required, and this approach is recommended for similar healthcare improvement initiatives.18
Conclusion
Whilst individual elements of tracheostomy healthcare improvements have been have been evaluated and published before, our project is the first detailed evaluation of the effectiveness of bringing together all of the GTC best practices, combining education, equipment provision, service redesign, multidisciplinary leadership and patient involvement. The GTC community provided invaluable expertise and personal resources to the participating sites and teams and this on going support and the ability to anonymously benchmark and feedback comparative data with other global sites is expected to continue to maintain the improvements at participating sites.
The educational, patient-centred and organisational aims were largely achieved, although due to the diversity amongst the participating sites, the aims of the project were tailored and adapted to reflect baseline differences. The GTC database proved effective in capturing meaningful data from the bedside and our chosen metrics appeared to reflect the quality of care delivered, as reported by staff, patients and families. Our data drove improvements, even where engagement was less enthusiastic and the reported benefits led to new teams and ways of working being implemented that appear sustainable.
Whilst the primary aim of this project was to improve the quality and safety of care, economic evaluation is important in modern healthcare. Membership of the GTC currently costs £5,000 for two years and effectively meeting key drivers will also have an associated cost. For our current project, £74,992 was awarded by the Health Foundation to integrate the GTC into four sites. Approximately £30,000 was spent on staffing costs with the majority of the rest spent on education and comprehensive evaluation.
The ‘cost’ to an organisation of tracheostomy-related problems can be measured in reputation, service loss and financially, with poor care leading to patient harm, readmission or admission to higher levels of care, prolonged LoS and potentially, compensation. Separating the expense of specific tracheostomy care from the costs of providing care for the patient as a whole in hospital is difficult. Extreme adverse events leading to death and hypoxic brain injury have defined, associated costs.19 As there was only one tracheostomy-related death during this project and no hypoxic brain injuries we estimated potential cost savings based on reductions in ward and ICU LoS. Using the NHS Institute for Innovation and Improvement cost model (ward bed day £225, critical care bed day £1,321)20 we estimate savings of £472,969 for the 296 patients. These reference costs are conservative in comparison to other reports21. A more robust and detailed economic evaluation will be essential if the membership of such programmes is to be recommended unreservedly to the wider NHS.
This pilot project has attracted further funding as part of the Health Foundation Spreading Improvement programme 2015. Whilst further evaluation in politically and geographically diverse sites is needed, it is likely that the comprehensive resources of the GTC will be of benefit to other NHS hospitals and indeed other healthcare systems around the world.
Acknowledgments
We gratefully acknowledge the support of all multidisciplinary staff involved in delivering this project at each of the sites.
References
Footnotes
Declaration of interests BAM is European Lead of the Global Tracheostomy Collaborative and a member of the Board of Directors. BAM is also NHS England's Tracheostomy Lead Clinician.
DWR is Founder and President of the Global Tracheostomy Collaborative and a member of the Board of Directors.
Funding Funded by the Health Foundation as part of the Shine 2014 project (Improving multidisciplinary tracheostomy care: implementing the Global Tracheostomy Collaborative quality improvement project). Health Foundation is an independent charity committed to bringing about better health and health care for people in the UK.
Ethical approval The Health Research Authority online toolkit concluded that this study did not require formal application for ethics review. The Governance Board and Caldicott Guardian of the University Hospital South Manchester provided oversight and governance throughout the project on behalf of the South Sector Partnership (the four participating NHS Trusts). The Board considered and agreed with the position statement of the GTC ‘Navigating IRB/ethics 2014’ available from www.globaltrach.org that details why participation in the GTC meets criteria to be considered as a QI initiative.