Article Text

Abstract
Constipation is a common and often overlooked problem, but it can cause serious complications for patients including pain, nausea, urinary retention, and prolonged hospital admission. There are no recognised criteria for the diagnosis of constipation in the acute hospital setting, and it is often the role of the ward doctor to identify and manage this problem.
Completion and monitoring of “stool charts” by nursing and medical staff is key to proper recognition and management of constipation. A baseline study found that while charts were completed well, they were only monitored by doctors 17.5% of the time. This quality improvement project introduced an altered “continuation sheet” to the clinical notes to prompt monitoring of stool charts and provide an area for documentation. This resulted in an increase in monitoring to 66.7%.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Managing constipation can be challenging and there is no consensus on best practice. Guidelines that are available are often based on expert opinion due to the lack of high quality evidence; however, there are simple measures that can be taken based on this guidance. Healthcare staff should be able to prevent unnecessary patient suffering by identifying and managing constipation early.
Kettering General NHS Foundation Trust is a district hospital in the East Midlands with over 600 beds and a higher than average proportion of elderly patients. Constipation can affect up to half of elderly hospital inpatients.
In our hospital, the nursing team monitor a patient's bowel movements using a stool chart to record the date, time, and consistency. The ward doctors are responsible for checking the nursing notes and acting on the information. We have witnessed occasions where patients have not opened their bowels for several days but this was not reported or acted up on, leading in one case to acute urinary retention delaying the patients discharge from hospital. This suggests a lack of monitoring.
Three of us (FY1 doctors) determined to try and address this problem while undertaking the BaSIS Programme, using improvement science methods that we learnt to guide our efforts. Our initial aim was to reduce constipation to 0% over an eight week period on one gastroenterology/general medical ward, but as we gained more intelligence about the problem we revised this aim.
Background
Constipation is a common and often overlooked problem, both in the community and in the acute hospital setting. The prevalence has been reported to be between 2-28%;1 this variance might be due to inconsistencies surrounding the definition of constipation. While the “Rome Criteria” are often cited in the community setting as a useful diagnostic tool, clinicians in the hospital setting will often rely on the patient's concerns or information from nursing colleagues.2
The elderly are particularly affected by constipation, and prevalence rises to between 30 to 40% in those aged over 65.3 The reasons for this are numerous, but might include reduced mobility, comorbidities, polypharmacy, weaker abdominal and pelvic muscles, and a reduced gastro-colic reflex secondary to smaller meal sizes.2 Hospital admission is associated with many of these factors and may exacerbate or predispose to constipation, particularly due to immobility, dehydration, altered diet, and prescription of opioids.
Although it might be overlooked as a trivial problem, constipation has a serious impact on patients. At the very least it causes pain and discomfort, nausea, and reduced appetite. It has been shown to significantly impact quality of life.3 In elderly patients it is associated with distressing confusion, and in the most severe cases it could lead to urinary retention and bowel obstruction. Around 40% of hospital inpatients are thought to have faecal impaction which can lead to both urinary and faecal incontinence.3 Even the smallest of these problems can delay recovery and prolong admission, which is distressing for patients and detrimental to their health, while simultaneously causing potentially avoidable costs for the hospital. The economic burden of constipation extends to primary care, and is thought to cost £4.5 million a year in GP visits.3 It is clear then that effective recognition and management of constipation is crucial to good care.
We produced a high level process map (see Supplement 1 – process map) to identify the processes involved. We identified nursing staff filling in the stool charts as one of the earliest processes, so initially decided to work with the nurses on our interventions. We worked on the premise that if we improved recognition by nurses then we might also improve the processes downstream from them too, such as doctor's monitoring and prescribing.
Supplementary process map
Baseline measurement
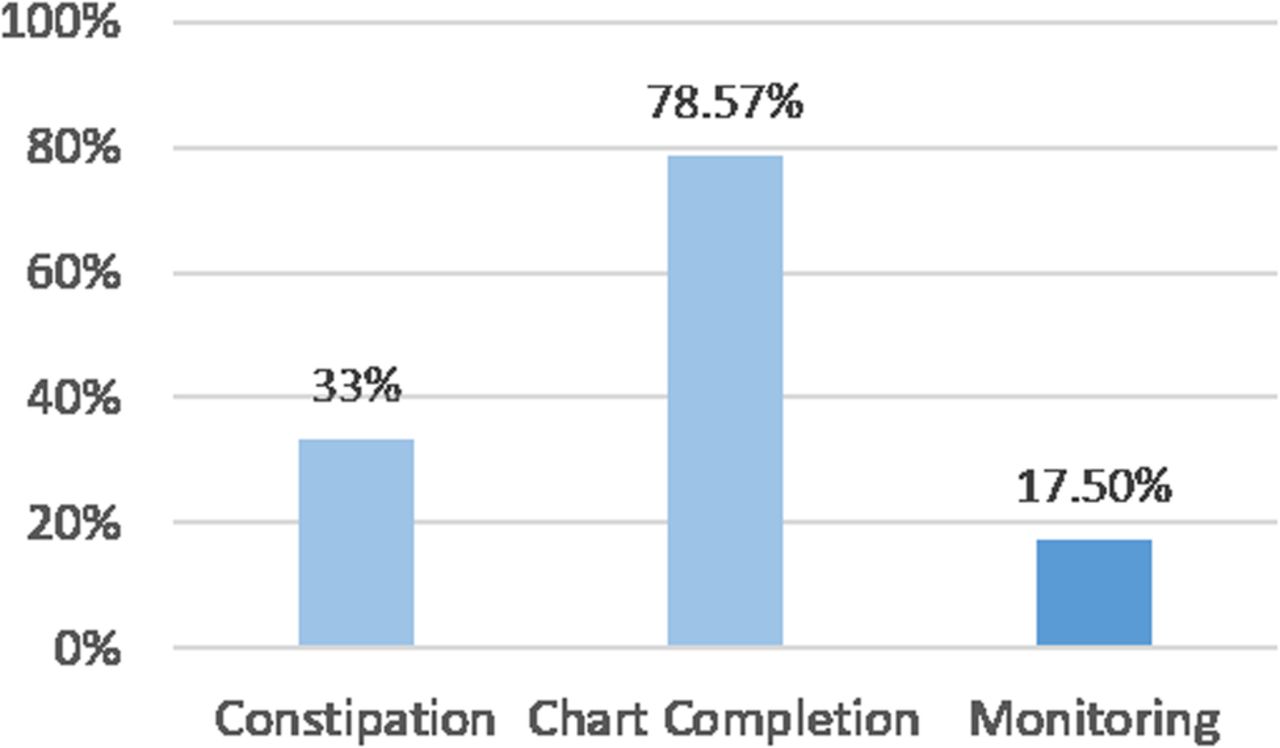
We went on to collect baseline data from a gastroenterology/general medical ward (See Figure 1). This demonstrated that nursing staff completed stool charts frequently, achieving 78.6% completion. In contrast, only 17.5% of ward rounds showed evidence in the clinical notes of doctors monitoring the stool charts.
Design
Our initial aim was to reduce the prevalence of constipation in our sampled patients since this is the outcome that matters most to our patients. However, we selected the following process measure as our primary aim due to the short duration of this project: to improve the monitoring of constipation by junior doctors on a general medical ward, so that 80% of ward rounds showed documented evidence of monitoring in the clinical notes. We aimed to achieve this over an eight week period.
In order to deliver an improvement within our reach we decided to limit our improvement efforts to the gastroenterology ward. All of our team members had worked there, making interventions easier to carry out; this comprised of 29 hospital beds divided across four bays. Each bay was staffed by a different doctor and nursing staff. When collecting data, we selected patients across all bays to prevent bias from monitoring the performance of only specific doctors.
As previously stated, defining constipation is difficult. We chose a simple and common definition seen throughout the literature where constipation is bowel opening frequency less than three times per week.1 ,3 Because of this definition we chose patients whose admission had lasted at least one week. We also chose to focus on elderly patients, given that this group are most affected by constipation and more often have complications such as faecal impaction.3 On the occasion that a patient's stool chart was incomplete, we assumed that they had not opened their bowels that day.
We randomly selected six patients across all four bays every two weeks collecting data from the stool charts and clinical notes. Our process measure was the percentage of ward round entries that showed evidence of monitoring by doctors (% monitoring) while our outcome measure was the prevalence of constipation. We also collected data on the completion of stool charts although we did not intend to directly target this. We generated a number of change ideas and selected some of these as our interventions which we tested by completing four plan, do, study, act (PDSA) cycles across the eight week period.
Strategy
Our SMART aim was to improve monitoring of constipation by doctors on one gastronenterology/general medical ward so that 80% of ward round entries made by doctors took into account stool charts by the end of eight weeks. We undertook four PDSA test cycles (see Supplement 2 - PDSAs and final monitoring chart)
Supplementary PDSAs and final monitoring chart
PDSA cycle 1: Our initial intervention was to provide a reminder to doctors during each morning ward meeting that stool charts should be checked. This was done by a designated doctor on the ward each day. This achieved an increase in monitoring to 30%. Feedback received indicated was that this was not sustainable as the designated doctor would not always be there and would lose interest.
PDSA cycle 2: In order to build and strengthen on our reminder idea, we added a column to the ward doctor's handover sheet for our second intervention; a tick box for if the stool chart had been monitored. There was a slight improvement with this as monitoring increased to 40%. Feedback from the ward doctors stated that this was inconvenient as it added extra paperwork.
PDSA cycle 3: We hypothesised that our change idea (intervention) may be more effective if we made it more convenient. For our third test we thought about how we could integrate the reminder into the doctor's ward round. We felt that the only place a doctor was guaranteed to look was in the medical notes themselves. We therefore altered the hospital's “continuation sheets” to include a tick box for if bowels had opened; this acted as a prompt and a convenient way to record monitoring. Although successful in increasing monitoring to 60%, the feedback was mainly regarding logistical issues and “continuation sheet” design. It was deemed that the changes to the sheets were not obvious and it was not easy to find and use the sheets. For this reason we thought that the improvement was unlikely to be sustained after we had left the team.
PDSA cycle 4: For our final test cycle we took our most successful intervention and acted on the feedback we received. We informed the ward clerk of the sheets and placed them on notes trolleys around the ward. We also changed the design so it was more prominent on the page. There was a small increase in monitoring to 66.7%.
Results
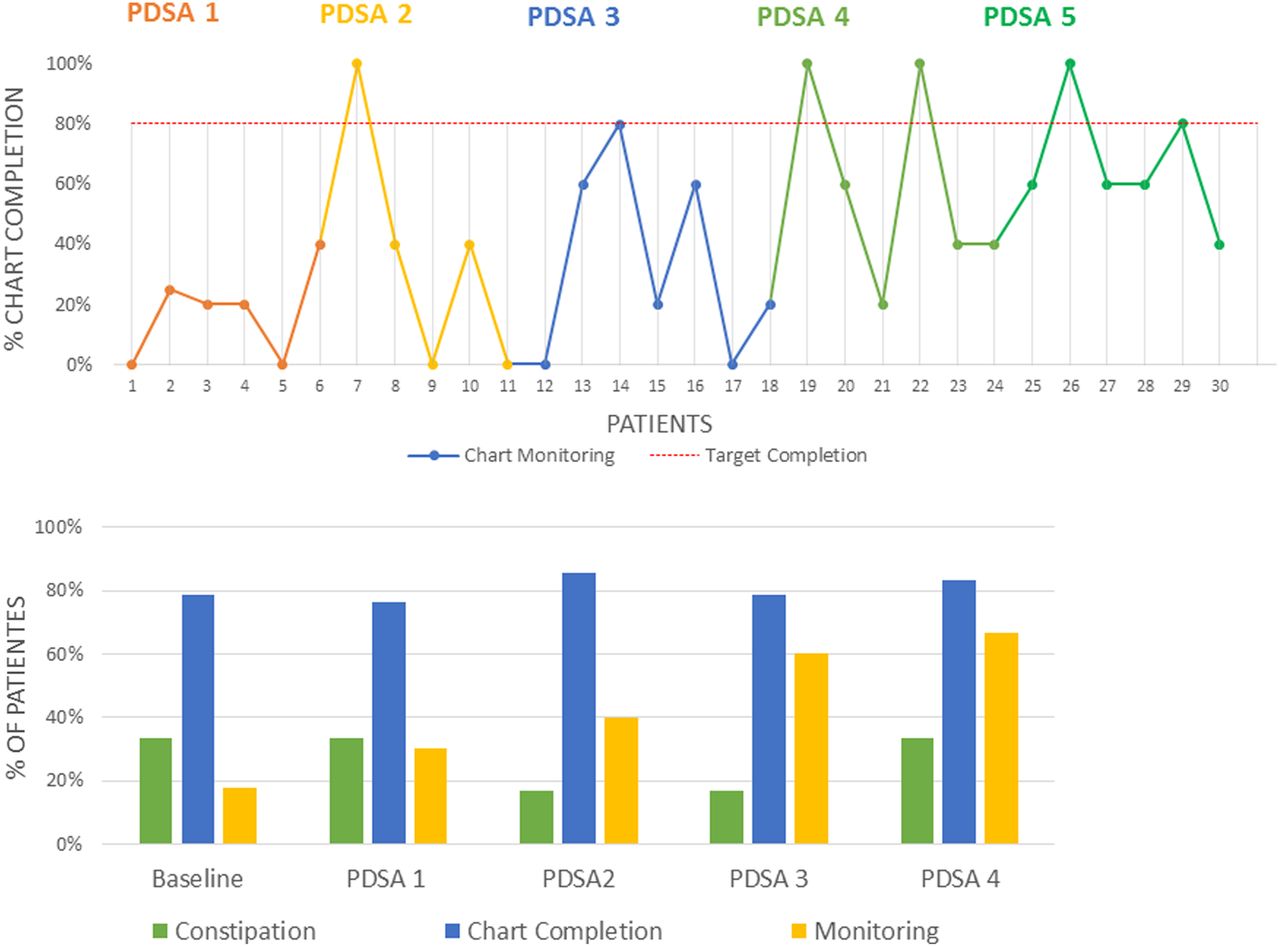
Each subsequent intervention that was implemented had a significant effect on stool chart monitoring percentages. Data were collected for six patients for each test cycle and the process measure was plotted on a run chart. Evidence of stool chart monitoring with the intervention from PDSA cycle 4 was very effective (66.7%) in comparison to baseline data (17.5%). Our final change idea was more than twice as effective as our first. Chart completion by the nurses during the improvement project period did not vary significantly, and outcome (as measured by diagnosis of constipation) did not alter significantly either (see Figure 2).

{kind=link}
{kind=link}
Lessons and limitations
Our findings suggest that each intervention was somewhat effective and that simple reminders on the ward can have a positive impact, at least in the short term. The intervention that proved most effective involved an edited “continuation sheet” which was quick and simple to complete. We feel that this worked because the medical notes are already a part of the doctors workflow and therefore using this as an area for prompts and reminders is more effective than the introduction of new forms and excess paperwork. We also felt that this intervention had a greater chance of being sustainable. In comparison, the interventions that were least effective included verbal reminders and tasks that added to the doctors' workload, such as the handover sheet.
We were not able to achieve our main process aim of a target level of 80% of stool charts that were evidently monitored by doctors. Timing was one of the main limiting factors as this project was bound by an eight week period, which meant that our ideas for intervention to improve the monitoring of stool charts were not all implemented due to the time constraints. Other factors that hindered our efforts include doctors displaying little interest to our project or being too preoccupied to participate. There were also minor issues with supplying and distributing our edited continuation sheets.
For example, for our change idea to succeed, we had to ensure that these edited continuation sheets were placed appropriately across the ward so that they were readily accessible. Finally, some interventions were not feasible due to a lack of budget. For instance, we wanted to re-organise the bedside notes into folders with dividers to indicate where each chart is, as this would again simplify both the doctor's and nurse's workflow. On discussion with ward management, this is something that may be possible in the future.
Although our findings showed an improvement in the monitoring of stool charts by doctors, we did not see a corresponding improvement in terms of reducing of the overall incidence of constipation among the patients on the ward (outcome measure). We felt that the prescription of laxatives would have been our next stage of improvement based on our initial process map, but only when our initial aim has been achieved, ie the target level of 80% stool chart monitoring.
Improvement of laxative prescription using quality improvement methodology has been demonstrated previously, which successfully changed attitudes towards prescriptions while reducing costs, but without showing an improvement in prevalence of constipation.4 This would be an interesting way to further our project, but as previously stated constipation and the complications thereof are difficult to measure.
This was our first improvement project, and while we know that constipation matters to patients we did not illicit their views. This would be another measure that could be developed if the improvement were to be developed further.
Conclusion
In summary, constipation is a common problem in hospital, particularly in elderly patients. Doctors should assess a patient's bowel habits on a daily basis, which could prove useful in terms of recognising constipation at an early stage and acting on this accordingly. This could prevent the development of unnecessary complications associated with constipation as well as inappropriate delays in discharge. A simple tool such as a “continuation sheet” can be an ideal way to aid staff in doing this, without producing extra work.
We have learnt a great deal about the use of improvement science as a method for testing, refining, and embedding change and look forward to undertaking our next improvement project and continuing improve as we learn.
Acknowledgments
Health Education England (Working across the East Midlands) Building Safety Improvement Skills (BaSIS) programme, Dr Sarah Moreman (FY1, QI Team member), the ward staff (help along the way), Quality Improvement Clinic (publishing and sharing this work), Dr Lisa Smith (for being our Mentor).
Footnotes
Declaration of interests Nothing to declare.
Ethical approval This project was designed to improve the service for patients. It was undertaken using improvement science methodology and was not deemed to require ethics approval. The interventions made were designed to standardise and optimise routine accepted good practice.