Article Text

Abstract
Access to mental health providers has become an increasingly common challenge for many patients with depression and anxiety disorders. Primary care providers often manage this gap in care and currently provide solo care without the assistance of other team members. In order to provide quality care that aligns with best practice, we developed a depression and anxiety disorder treatment pathway utilizing a multidisciplinary team based on each members' individual skill set, or skill-task alignment. The main change to treatment implemented by the pathway was the addition of a clinical pharmacist in the management of patient care. This pathway was trialed over five months targeting two adult primary care teams (approximately 34 physicians and Advanced Registered Nurse Practitioners [ARNPs]) while the other five teams continued with current practice standards. Post-implementation metrics indicated that clinical pharmacists successfully contacted 55% (406 of 738) of patients started on medication or who had a medication changed. Of these patients reached, 82 (20%) had an intervention completed. In addition, all physician leaders on the planning team (n=6) stated the new pathway was well received and delivered positive feedback from team members.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Access to behavioral and mental health specialists within Washington State, USA has been a struggle for many years. A 2015 report by the Washington Health Alliance (WHA) demonstrated that the state performance lagged on nationally-endorsed metrics for the treatment of major depression: antidepressant medication management adherence rate for the state was 70% at 12 weeks and 54% at 6 months after initiation of treatment, compared to the national 90th percentile of 75% and 60%, respectively.1
The Department of Primary Care at Virginia Mason Medical Center, a nonprofit regional health care delivery system with approximately 450 physicians, 800,000 outpatient visits, and 17,000 hospital visits annually developed a multidisciplinary guiding team to improve care for patients with major depression and anxiety disorders after the release of state-wide metrics. The team determined that in order to better serve patients, follow up care needs to be standardized and the numerous discrepancies in practice management patterns among providers needed to be reduced. These discrepancies included variation in assessment of depression, in follow-up time period ranging from weeks to months, and in the starting dose of antidepressants.
Background
Behavioral health conditions are prevalent among adults world-wide. A World Health Organization review of mental health management found that mental health problems account for 2.5% of the gross national product in the United States and between 3% to 4% of gross national product for the Member States of the European Union.2 In the United States 57% of the population will meet the diagnostic criteria for a behavioral health condition in their lifetime; 31% will experience anxiety, and 21% will struggle with a mood disorder.3 One report estimates the presence of mental health disorders raises overall health care costs by approximately $6,060 per patient annually in patients with chronic medical conditions.4 Within our organization, prescribing providers (i.e. physicians, physician assistants, ARNPs) individually determined the follow up plan for each patient. Without team consensus on standards of care, variation in practice patterns for mood disorders contributed to patient loss to follow up, medication non-adherence, and differences in quality of care. In each primary care team consisting of physicians, ARNPs, physician assistants (PAs), nurse care manager, clinical pharmacists, and medical assistants, the clinical pharmacist is responsible for assisting in medication management of chronic disease states such as cardiovascular disease and chronic pain. We realized that incorporation of clinical pharmacists into care for medication management for mood disorders could allow primary care teams to consistently deliver evidence-based care. A multi-disciplinary telemedicine-based care approach including clinical pharmacists that demonstrated improved outcomes for mood disorders provided evidence for our model of care.5
Baseline measurement
For this project, two of the seven primary care teams identified physician, pharmacy, and nursing leaders to develop a workgroup. The team recognized the WHA-reported score of 12-week and 6-month medication adherence for the organization was deemed “average.” We then analyzed current state alongside each team members' appropriate skill set and recognized an opportunity for incorporating pharmacists into the team-based care delivery model. We targeted improving follow up at two weeks after initiation of medication treatment for mood disorders in accordance to accepted standards of care.6 Our baseline measure showed zero pharmacist involvement after initiation or change in medication treatment for mood disorders in primary care.
Design
Given the high burden of mental illness on disability on parity with other chronic illnesses, we determined that we should apply the rigor of our quality improvement processes to provide the best evidence-based care for depression possible to our patients.7–8
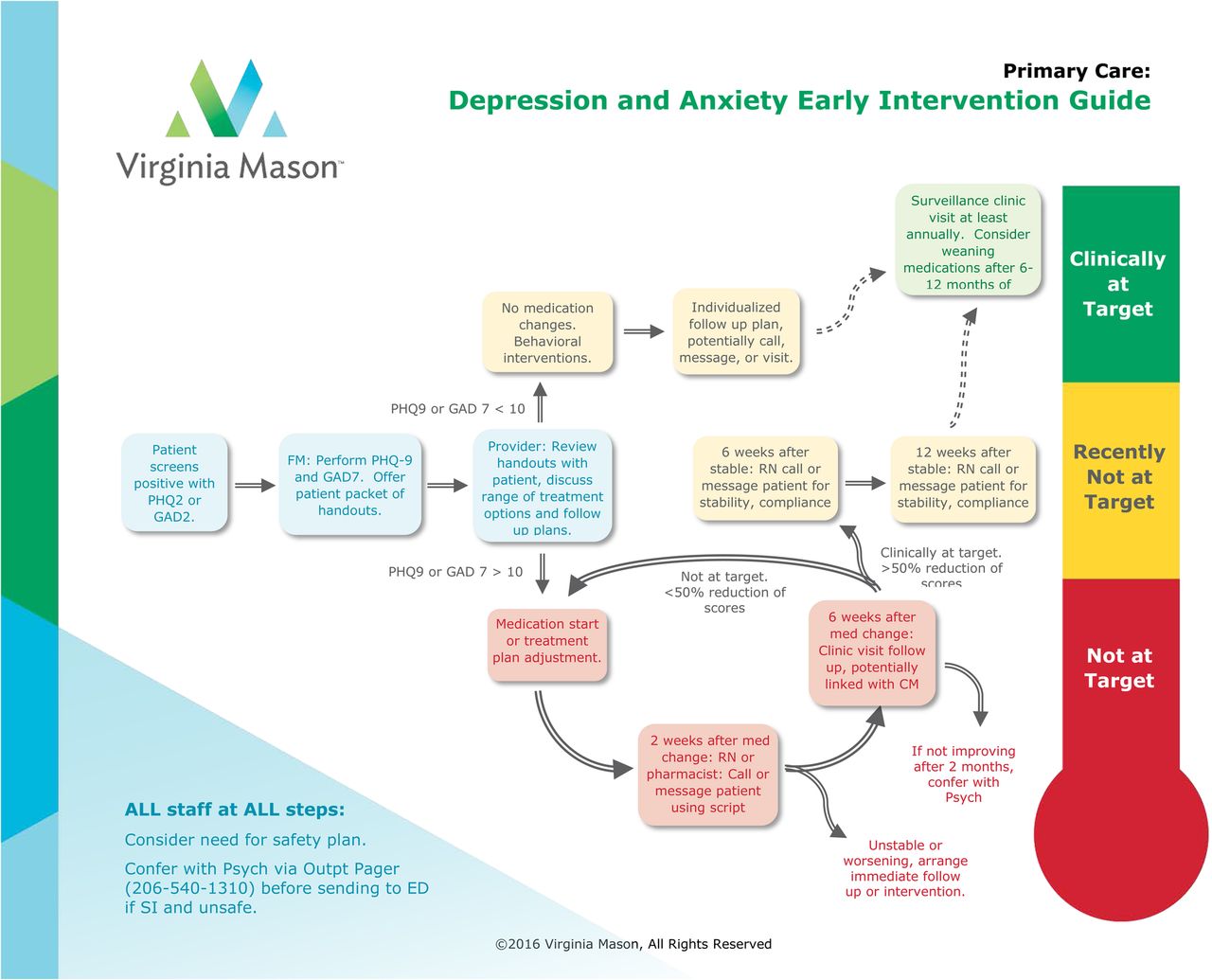
Relying upon the physician, ARNP, or PA prescribing the medication to provide comprehensive care was impractical, wasteful, and underutilized other members of the care team who could provide timely and effective care. Pharmacists have a unique skill set to allow for the assessment of medication tolerance and clinical response to treatment. We designed a clinical pathway to direct the flow of patient care among team members based on specific patient needs and response to therapy. This agreed upon standard of care was vetted with physician, pharmacy, and psychiatry leadership. After initiation of medication, or change to current treatment, the patient receives a two-week follow up phone call from a clinical pharmacist as evidence has shown the likelihood of discontinuation due to medication intolerance is highest in the first few weeks of treatment.6 Then, a six-week follow up visit with prescribing provider is scheduled. This cycle is continued until patient reaches a 50% reduction in baseline Patient Health Questionnaire-9 (PHQ9) or Generalized Anxiety Disorder-7 (GAD7) score, at which time the patient is scheduled with a 12-week and then 6-month follow up visit.9 (Figure 1) A behavioral health guiding team consisting of Department of Primary Care leaders, clinical pharmacists, clinician champions, psychiatry leadership, and nursing leaders met monthly to review the outcomes of the PDSA cycles.

Strategy
All patients who were initiated on an anti-depressant or anxiolytic medication during PDSA Cycle 1 were referred to the clinical pharmacist for a two-week follow up phone call. Medication tolerance and adherence were assessed during this call, along with non-pharmacologic management of current symptoms. Based on standard guidelines and evidence for follow up, we hypothesized that outreach to the patient within two weeks of a medication start or change would result in improved medication adherence and clinical outcomes.
To assess clinical response to therapy, PHQ9 and GAD7 assessments were administered. If appropriate, the pharmacist would increase the dose of current medication or change to a different medication. The pharmacist also ensured all patients had a scheduled six-week follow up visit with the prescribing provider. Patient feedback during and after the phone call, along with provider feedback during team meetings, consistently reflected the value of the phone call in assessing response to treatment and determining next steps in therapy. However, the amount of time spent on the phone call (averaging 15 minutes) did not fit into the daily workflow of the clinical pharmacist. In PDSA Cycle 2, the administration of the PHQ9 and GAD7 assessment was eliminated. This portion of the discussion was very time consuming and was determined by primary care providers and psychiatry peers to not be value-added at two weeks into treatment initiation. The result was a more manageable time commitment for the clinical pharmacist as phone call cycle times decreased to an average of seven minutes. After five more months, the pathway was rolled out to all primary care teams resulting in 82 providers referring to the clinical pharmacist for follow up. There was no negative feedback and all members of the team (providers and patients) felt more supported by the frequent contact. After implementation at all sites, a final PDSA Cycle was initiated in which prescribing providers also referred patients to the pharmacist for the six-week follow up in-person visit. The success from earlier cycles demonstrated the pharmacist's ability to play a larger role in the patient's care. Any individuals with suicidal ideation or suspected bipolar disorder were excluded from follow up with the clinical pharmacist.To ensure patient safety, the behavioral health guiding team developed a standardized protocol for assessing suicidality where any team member with concerns about suicidality paged the on-call psychiatrist.
Results
After implementation, measurements were used to capture: 1) pharmacists' interventions during the call, 2) the rate of referral to pharmacist per primary care provider, and 3) the amount of time the pharmacist spent daily completing follow up phone calls.In PDSA Cycle 1 a total of 165 patients were referred to the pharmacist for a two week follow up call.Of these patients, 95 consults were completed (58%) with an average cycle time of 15 minutes for each phone call.For PDSA Cycle 2 the previously mentioned changes were implemented for a trial period of five months.A total of 55% (406 of 738) of patients started on medication, or who had a medication change, were successfully contacted by the clinical pharmacist (Figure 2). Those not contacted were unable to be reached or declined the discussion. Of those contacted, 20% had an intervention completed. These interventions included management of side effects, titrating up medication from initiation dose, or changing medication based on patient report. We determined that each primary care provider referred two-three patients each month to the pharmacist for a two-week follow up phone call assessment. The clinical pharmacists completed these assessments with an average phone call time of seven minutes (Figure 3). One year after the PDSA cycles were initiated, the behavioral health guiding team decided to scale up the intervention to all clinic sites within the health system. Reasons for the intervention and lessons learned from the PDSA's were disseminated through established organizational meeting structures to scale up successful innovations. We ensured sustainability of this intervention by incorporating it into existing workflows and ongoing modifications adapted to each clinic site.
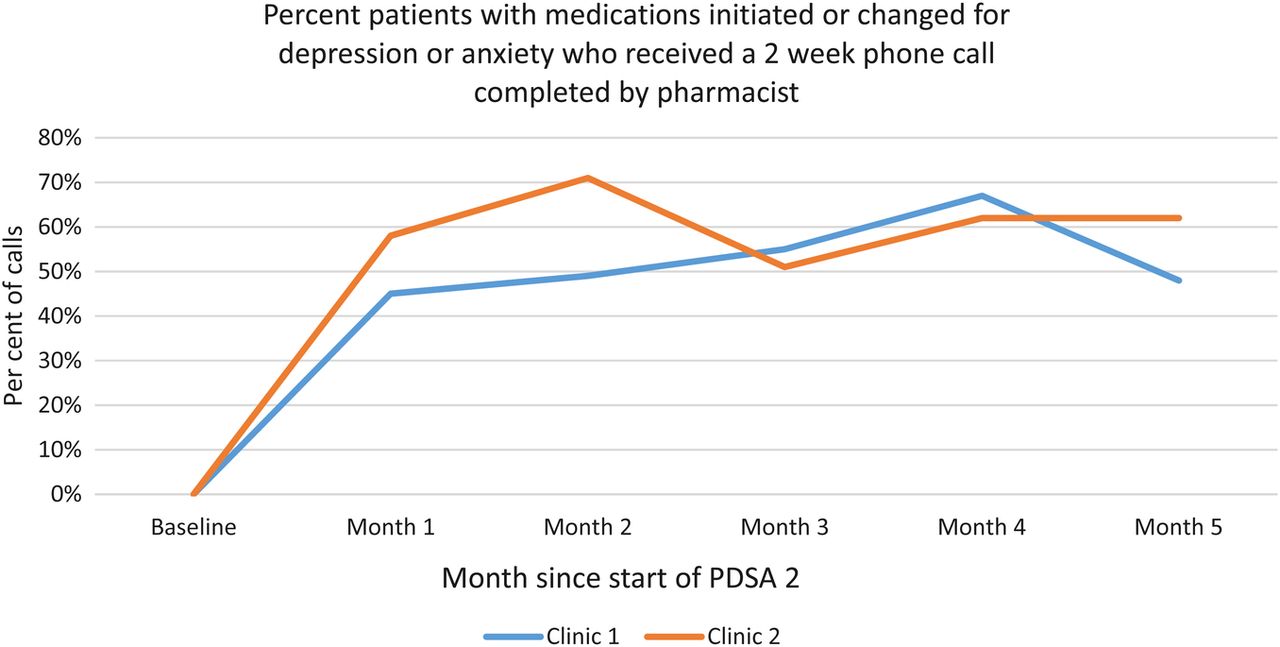
*PDSA1 data not displayed due to missing data

{kind=link}
{kind=link}
{kind=link}
Lessons and limitations
We learned many lessons through this workgroup and PDSA cycles. One lesson was to make sure to review current state workflows and how to fit new patients, or a new patient population, into a process that is already in place. Utilization of a multidisciplinary workgroup helped to ensure all team members are contributing at the top of their license and scope of practice. This work also lead to increased collaboration between the psychiatry department and clinical pharmacy team. Moving forward, a clinical pharmacist specializing in psychiatry will be added to the behavioral health outpatient team.
The impact this work will have on the WHA medication adherence quality metrics is not yet known as the annual WHA Community Checkup Report has not been released.However we anticipate an improvement in our outcomes in 2016.
We acknowledge several limitations to our evaluation. This study was performed at a single integrated health system in an urban setting, limiting the generalizability of the findings. Lean concepts, including continuous quality improvement and embedding evidence-based care into practice, are familiar to our staff and providers, enhancing our ability to rapidly implement change.10
Outcomes for the five provider groups not involved in the PDSA were not compared to the pre- or post-study results.With no ability to track these patients on a registry, it is difficult to identify those who fall outside the follow-up protocol, or fall out of care.Without this registry function, we are also unable to determine if we saved downstream healthcare costs in terms of emergency department visits averted or decrease in complications from uncontrolled depression on comorbid disease.
As we scaled up the intervention to the entire department, it became apparent the volume of follow-up phone calls was higher than previously thought, which limited pharmacists' time to spend on other clinical activities such as hypertension management. When available, the pharmacists conduct outreach via our secure patient online portal, which may allow quicker initial outreach to patients. There was no reimbursement from payers for telephonic care, which may limit the scalability of this intervention to other settings, although this may change in the future.
Conclusion
Implementing a standard treatment pathway for depression and anxiety disorders built a structured process for a patient population that does not always have access to behavioral health specialists. The work resulted in level-loading the care provided among team members based on expertise and ensuring the patient had timely follow up and management. Clinical pharmacists increased their skillset for treating depression and anxiety and enhanced their ability to make interventions with patients who are referred to them for other chronic disease state management (e.g. hypertension, chronic pain).
One randomized controlled trial had a telephone follow up call for patients failing one medication trial which showed follow up rates of 8.2%, but to our knowledge, our intervention is the first to offer pharmacist follow up phone calls for all patients on medication management of depression regardless of prior success or failure of medication therapy.5 If we improve outcomes on our depression quality metrics, we hope that this model can be adapted to other healthcare settings.
Acknowledgments
Catherine Potts, MD, Karina Uldall, MD, Richard Furlong MD, Jenny Park, PharmD, Michelle Lyon, PharmD, Tina Ngo, PharmD, Laurel Morrison, MD, Nick Moy, MD, Catherine Edwards, MD
Footnotes
Declaration of interests Nothing to declare.
Ethical approval According to the policy activities that constitute research at Virginia Mason Medical Center this work met criteria for operational improvement activities exempt from ethics review.