Article Text

Abstract
Shoulder problems account for 2.4% of GP consultations in the United Kingdom and of those 70% are related to the rotator cuff. Many rotator cuff tears are of a degenerate nature but they can occur as a result of trauma in 8% of cases. Evidence suggests that patients with traumatic rotator cuff tears gain a better outcome in terms of pain and function if the tear is repaired early after injury.
A specialist shoulder soft tissue injury clinic was set up in a large UK NHS teaching hospital with the primary purpose in the first year to halve the length of time patients with traumatic rotator cuff tears had to wait to consult a specialist and double the number of patients undergoing surgical repair within three months. The secondary purpose was to ensure that the new clinic was utilised to capacity by the end of the first year. The clinic was later expanded to manage patients with acute glenohumeral joint (GHJ) or acromioclavicular joint (ACJ) dislocations and identify those patients requiring surgical stabilisation. The new service involved referral of all patients presenting to the Accident & Emergency department with recent shoulder trauma and either an inability to raise the arm over shoulder height with a normal set of radiographs, or a confirmed GHJ or ACJ dislocation; to a specialist clinic run by an experienced upper limb physiotherapist. Patients were reassessed and referred for further imaging if required. Those patients found to have traumatic rotator cuff tears or structural instability lesions were listed for expedited surgery. The clinic ran alongside a consultant-led fracture clinic giving fast access to surgical decision-making. The service was reviewed after 3, 6, and 12 months and findings compared to a sample of 30 consecutive patients having undergone rotator cuff repair surgery via the previous pathway.
144 patients were referred to the clinic in the first year: 62 with rotator cuff symptoms, 38 with GHJ instability, 13 with ACJ instability, and 33 others. 7 missed fractures were identified. 12 patients subsequently underwent rotator cuff repair surgery, 10 GHJ stabilisation, and 1 ACJ stabilisation. Mean referral time to first clinical assessment improved from 37 days to 8 days. For rotator cuff repair: mean referral to surgery time was 86 days compared with 115 days on the old pathway. 58% of patients underwent surgery within 90 days of injury compared with 20% previously.
Our new service resulted in surgical repair of traumatic rotator cuff tears 29 days faster than the traditional system with an extra 38% of patients having surgery within 90 days of injury - a benchmark thought to improve outcome. Future work will aim to improve this percentage further and include long term patient follow up of outcome measures after surgery.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The Royal Derby Hospital, is part of Derby Teaching Hospitals NHS Foundation Trust, and is home to The Derby Shoulder Unit. This a secondary and tertiary referral centre for shoulder pathologies led by four specialist upper limb orthopaedic consultants. Historically, patients attending the Accident & Emergency department at The Royal Derby Hospital following traumatic injuries to the shoulder would be clinically assessed by a doctor or advanced nurse practitioner and undergo radiographic imaging if deemed appropriate. Patients with fractures or dislocations would be referred to the Shoulder Unit but those patients whose radiographs showed no bony injury or dislocation would be discharged home and advised to consult their General Practitioner if their symptoms failed to improve. Patients who had sustained significant soft tissue injuries, such as traumatic rotator cuff tears, often presented late to the Shoulder Unit having first been treated conservatively in Primary Care and then having waited for an out-patient referral. Evidence would suggest that these patients would gain better outcomes if their injury had been identified and treated sooner.
The aim of this project was to change the patient pathway by implementing a new soft tissue injury clinic where patients with such injuries could be diagnosed by a specialist in the Shoulder Unit soon after injury to facilitate earlier surgical repair. The primary purpose in the first year was to halve the length of time patients with traumatic rotator cuff tears had to wait to consult a specialist and double the number of patients undergoing surgical repair within three months. The secondary purpose was to ensure that the new clinic was utilised to capacity by the end of the first year.
Background
Shoulder problems account for 2.4% of GP consultations in the United Kingdom and of those 70% are related to the rotator cuff.1 Many rotator cuff tears are of a degenerate nature but they can occur as a result of trauma in 8% of cases.2 A systematic review published in 2013 drew conclusions, based on the limited evidence available, that patients undergoing rotator cuff repair fared better in terms of pain and function (measured by Constant Score) if surgery was performed less than three months from injury compared with those operated on after three months.4 Similar conclusions were drawn from a subsequent study measuring Oxford Shoulder Score comparing patients undergoing rotator cuff repair within versus beyond six months from injury.2 In that study the improvement in pain and function for early repair was double that of delayed repair. Another large retrospective study investigating predictive factors of successful rotator cuff repair found that symptom duration was important for traumatic tears and a statistically significant risk of retear was present if surgery was delayed beyond two years.5 In contrast, one recent retrospective study6 found that there was no difference in outcome in patients whose surgery took place before or after three months, however this may be explained by the fact that these patients underwent open surgical repair rather than the more modern and less invasive arthroscopic technique described by the other studies. Authors have suggested optimal repair times ranging from within three weeks3 to two years5 however no consensus exists. In general, though, the trend in the evidence would suggest that the earlier the repair the more satisfactory the outcome for the patient.
Baseline measurement
A retrospective analysis was undertaken to investigate the referral pathways of 30 patients who have previously undergone surgical repair of a traumatic rotator cuff tear. The typical pathway is described in Figure 1 as shown by the white text boxes. The mean time from General Practitioner referral to the patient being seen by a specialist in the Outpatient Orthopaedic Clinic was 37 days. The mean time from referral to treatment (surgery) was 115 days.

A flowchart showing the existing patient referral pathway in white and the new shoulder soft tissue injury clinic pathway in grey.
Design
The pathway for patients attending the Accident & Emergency department at the Royal Derby Hospital was redesigned in collaboration with the lead consultants for emergency care, upper limb trauma & orthopaedics, and radiology along with hospital management, the lead advanced nurse practitioner for A&E, lead upper limb physiotherapist, and administrative staff. The new pathway, shown via the grey text box in Figure 1, involved a new outpatient clinic run by an experienced upper limb specialist physiotherapist that was held once a week with 10 appointment slots available. The clinic was geographically situated adjacent to the upper limb fracture clinic with access to orthopaedic consultant advice if required. Access to urgent imaging was arranged with radiology with a view to same-day ultrasound scanning if capacity allowed.
Referral criteria were defined as:
Patient aged 45 or over.
Recent history of shoulder trauma.
Normal radiograph.
Unable to actively raise the arm above shoulder level.
Patients presenting to A&E that met the above criteria were no longer discharged back to the care of their General Practitioner but were given an appointment for the next available shoulder soft tissue injury clinic before going home.
Patient attendances to the clinic were subsequently monitored to record the volume of referrals, appropriateness of referrals, subsequent diagnosis, investigations, and treatments. Prior to commencement of the clinic a training session was delivered by the physiotherapist running the clinic [MB] to all of the advanced A&E nurse practitioners as typically they would be the clinicians usually assessing the majority of shoulder injuries to ensure that they were aware of the new service and understood the referral criteria.
The performance of the new system was assessed using the following outcome measures and compared to the aforementioned primary and secondary objectives:
Mean time from referral to assessment in the soft tissue injury clinic.
Mean time from referral to surgery for patients with traumatic rotator cuff tears.
Average number of appointment slots booked.
Percentage of patient non-attendances.
Strategy
Cycle 1:
The shoulder soft tissue injury clinic began in October 2014 and referrals were monitored in the first three months to the end of December 2014. The mean referral to assessment time was 5.8 days. During that time period only one patient with a traumatic rotator cuff tear was identified and listed for surgical repair. The time from referral to treatment for this patient was 28 days. During the first three months there were nine clinics but only 24 new patients had been referred and of those nine failed to attend their allocated appointment (37.5%). Seven patients were followed-up meaning that an average clinic only had three to four patients booked in. The majority of referrals did, though, meet the referral criteria but five had not had radiographic imaging.
At that stage further discussion took place to decide how best to proceed. So far the primary goals of the project had been met with the referral to assessment time more than halved and the patient having surgery within three months, however due to the small numbers of patients involved this was not a reliable measure. The concern was the free capacity in the clinic, so, to reduce the burden on the busy fracture clinics and to boost patient numbers, the referral criteria were expanded to include patients with confirmed acromio-clavicular joint dislocations, gleno-humeral joint dislocations that had been relocated, and suspected pectoralis major or biceps brachii tendon ruptures. Email memorandums were also sent to all A&E staff to remind them of the new pathway and encourage more referrals.
Cycle 2:
Referrals were monitored over the subsequent three months to the end of March 2015. Mean referral to assessment time was 6.1 days. Two patients were found to have traumatic rotator cuff tears and were listed for surgery. Both underwent surgery within three months with mean time from referral to treatment of 58.5 days. Three missed greater tuberosity fractures were identified but managed conservatively. Three patients were listed for shoulder stabilisation surgery following dislocation.
There were nine clinics during that time and the number of new patient referrals had more than doubled to 44, with 10 failing to attend (22.7%). Additionally 23 patients were seen for follow-up meaning the average clinic was booked with seven or eight patients. The lower DNA rate was considered to mean that referrals had been more appropriate.
Further discussion was had regarding the format of the clinic and referral criteria. These were left unchanged as it was felt that the clinic had now become productive and referrals had increased. The primary goal was being surpassed with referral to assessment time more than halved and all patients with rotator cuff tears undergoing surgery within three months. The secondary goal of the clinic running at the full capacity of 10 patients per session, however, had not been met so details of the clinic were then sent to two minor injury assessment clinics at outlying community hospitals inviting direct referral of patients that met the inclusion criteria, in the hope of increasing referral numbers further.
Cycle 3:
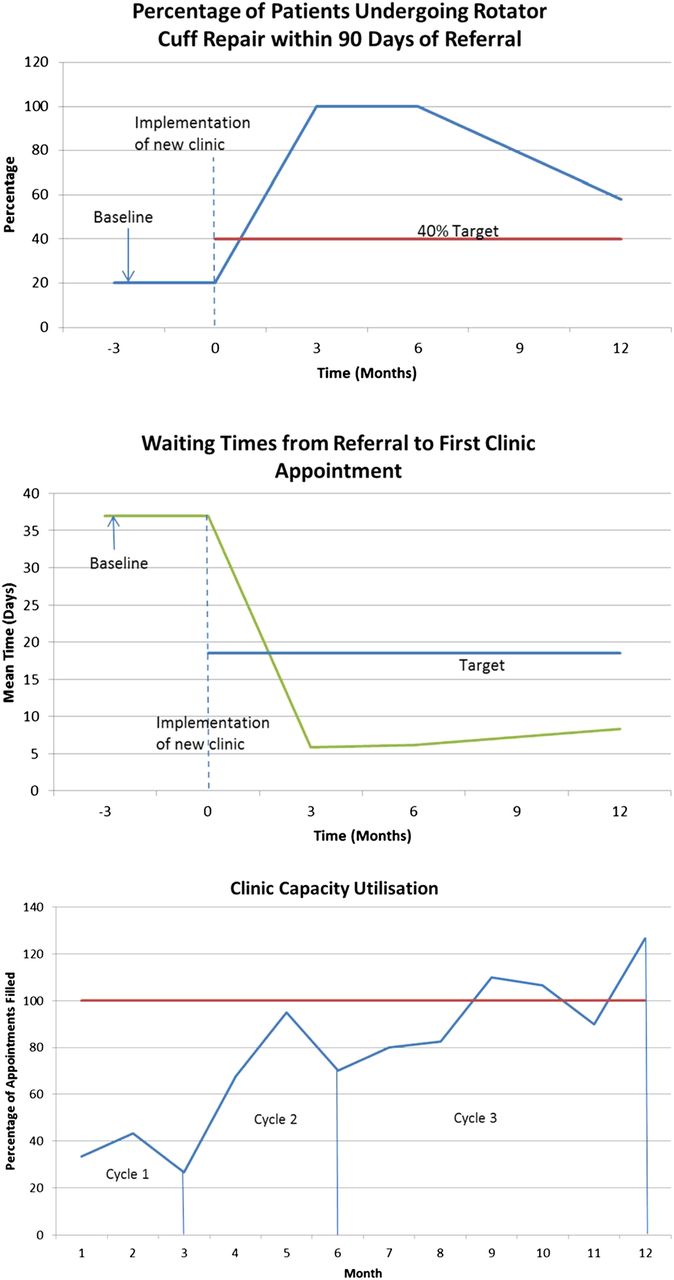
The final six month period from April 2015 to October 2015 saw 110 new patients referred. These patients were seen across 19 clinics along with 76 patient follow-ups. New patient non-attendance rate was 18.2%. The average clinic was fully booked with 10 patients. Mean referral to assessment time was 8.3 days. Nine patients underwent rotator cuff repair with mean referral to surgery time of 98.8 days. Four of these patients (44%) were operated on within 90 days.
The clinic had therefore satisfied the secondary goal having run at capacity for the last six months and had continued to meet the primary objective of the project.
Fluctuations in clinic capacity utilisation, mean waiting time from referral to first appointment, and percentage of patients undergoing surgery within 90 days are shown in the attached run charts.⇓

{kind=link}
{kind=link}
Results
Over the first year of the clinic a total of 144 individual patients were seen (139 new referrals and 5 follow-ups transferred from the fracture clinic). 62 patients had rotator cuff pathology with 30 rotator cuff tears identified. 12 patients were listed for rotator cuff repair surgery and the remainder were treated conservatively due to co-morbities, the massive size of some of the tears or their own volition. One patient underwent arthroscopic bursectomy for chronic bursitis. 38 patients had glenohumeral joint instability with 10 undergoing surgical stabilisation. One patient underwent acromio-clavicular joint stabilisation. Seven fractures of the greater tuberosity or glenoid were identified that had been missed by A&E. The remaining patients had a mixture of diagnoses including acute frozen shoulder, minor acromio-clavicular joint sprain or simple soft tissue bruising.
The mean time from referral to first clinic visit was eight days. The mean time from referral to surgery was 86 days with 58% of patients undergoing surgery within 90 days. This compares to a mean referral to first appointment on the old pathway of 37 days and mean referral to treatment time of 115 days with only 20% of patients undergoing surgery within 90 days. It should also be noted that on the new pathway the referral time to treatment time accurately reflects the time from injury to treatment as patients are referred directly from A&E on the day or within a few days of injury. The old pathway measures referral from GP to treatment so the majority of patients will have been referred after a period of conservative management. The referral to treatment time of 115 days on the old pathway is therefore an underestimate to the actual time from injury to surgery.
Lessons and limitations
Despite careful planning of the new service and widespread advertising of it to potential referrers within our organisation the uptake was very low initially. Unfortunately no accurate data was available prior to implementation regarding the numbers of potential patients presenting to the A&E department. Such information would have helped to guide the planning of new service to ensure better use of capacity. As it was, the initial three month trial informed us that referral numbers were lower than anticipated and that the referral criteria could be expanded to maximise capacity. In hindsight, a data monitoring exercise could have been performed prior to implementation to assess numbers of relevant patients attending A&E over a defined period e.g. one month. That said, there also appeared to be a gradual increase in referrals just simply with time suggesting that any new service takes time to become familiar to referrers and at the forefront of their minds when considering options for their patients.
In an ideal situation more frequent monitoring of data would have been advisable, however, with the clinic only held once per week and allowing for cancelled clinics due to leave, the data would have been too limited to highlight trends if reviewed more frequently than three-monthly. In hindsight, a further review at nine months may have helped to highlight the increased demand on clinic capacity with increasing numbers of clinics being over-booked. The challenge for the future is to ensure that clinic capacity is well utilised and that patients with acute rotator cuff tears continue to gain faster access to surgery despite the increased numbers of referrals. A limitation of the current study is the small sample size of 12 patients undergoing rotator cuff repair within the study period so this will require continued monitoring over time.
Following the expansion of the referral criteria to include acromioclavicular joint and glenohumeral joint dislocations a further study could investigate the potential benefit of faster access to specialist upper limb assessment for this patient group.
Conclusion
Our new service resulted in surgical repair of traumatic rotator cuff tears 29 days faster than the traditional system with an extra 38% of patients having surgery within 90 days of injury – a benchmark thought to improve outcome.4 Our service design also allowed for spare capacity to be utilised for the management of patients with shoulder instability to alleviate some of the outpatient fracture clinic demand. Patients with other soft tissue pathology such as calcific tendinitis or acute frozen shoulder gained access to specialist conservative treatment. Additionally a number of missed fractures were identified early and managed appropriately. Future study will involve on-going monitoring of the service and evaluation of long term patient follow up of outcome measures after surgery to assess whether faster access to surgery does indeed result in better outcomes for our patients as the literature would suggest.2–5 It is hoped that a similar pathway model might be adopted by other NHS Trusts to improve access to specialist management of shoulder soft tissue injuries.
Acknowledgments
The authors wish to acknowledge the contributions of Rachel Goulding, Dr Iain Lennon, Dr Chris Fang, and Dr Sanjay Patel in implementing this new service.
Footnotes
Declaration of interests The authors declare no conflicts of interest.
Ethical approval Ethical approval was not required as this study investigated pathway design rather than the treatments patients received.