Article Text

Abstract
As part of the Scottish Patient Safety Programme – Mental Health one of the main drivers was the reduction of harm to patients caused by restraint. The aim of this project was to reduce the number of restraints on our Acute Admissions ward.
Through use the of the Improvement Model (PDSA), frontline staff were empowered to implement small tests of change at a grassroots level. This approach has led to frontline staff having ownership of driving the changes on a daily basis within the Clinical area.
The use of a restraint data collection tool has been adapted and developed with frontline staff to ensure that the staff have ownership of data collected and is used to facilitate improvement. This data is used to inform the development of our Physical Interventions training. Most recently, following analysis, were able to introduce changes to promote the increased use of de-escalation and a shift from prone restraint to the safer seated restraint position.
Patient involvement has been paramount with their inclusion in the debrief process. The information gleaned from the patients is used for staff and patient reflection. This has created a learning environment not only for staff but also patients and carers. Everyone involved is able to identify reasons and triggers and generate ideas to reduce the possibility of another restraint.
The use of staff and patient safety climate surveys has ensured that we are constantly monitoring improvements in the feeling of safety amongst staff and patients.
Our approach has resulted in a change in the culture of restraint resulting in a sustained reduction of 50% in restraint.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
We set out to reduce harm experienced by staff and patients related to restraint incidents, within the Mental Health Service in Fife. We decided that this would be a significant improvement in the safety of our patients as “physical restraint is the only non-medical intervention in mental health with the potential directly to cause severe and even fatal injury to patients.“. (Lancaster et al, 2008, p. 307). We aimed to reduce the number of restraints but also to minimise the harm should an incident occur. Although our number of restraints were not higher than the national average we knew that any reduction we could gain would ultimately improve safety on our ward.
The Improvement Team consisted of a Project Manager and a Clinical Lead. We worked closely with the ward staff, the Physical Interventions Trainer, and our Administrative support.
Background
Over the last 15 to 20 years restraint and seclusion have received a growing level of political and public interest. They are contentious and potentially dangerous (Huckshorn et al, 2014) practices still in use in many healthcare settings today.
The Scottish Patient Safety Programme in Mental Health aim is to reduce harm experienced by patients in receipt of mental health care in Scotland. The programme is a national initiative which aims to drive improvement through the application of quality improvement methodology. Within the Mental Health programme one of the change packages is ‘Seclusion and Restraint’. In addition to this one of the key outcome measures is the reduction in the rate of restraint.
Baseline measurement
Data was collected to obtain a baseline using an existing reporting tool which was adapted with front-line staff. The data was collected from a 30 bedded Acute Admissions ward, with an average of 593 occupied bed day per month. Every restraint incident was recorded by ward staff and sent to the Patient Safety Team for collation.
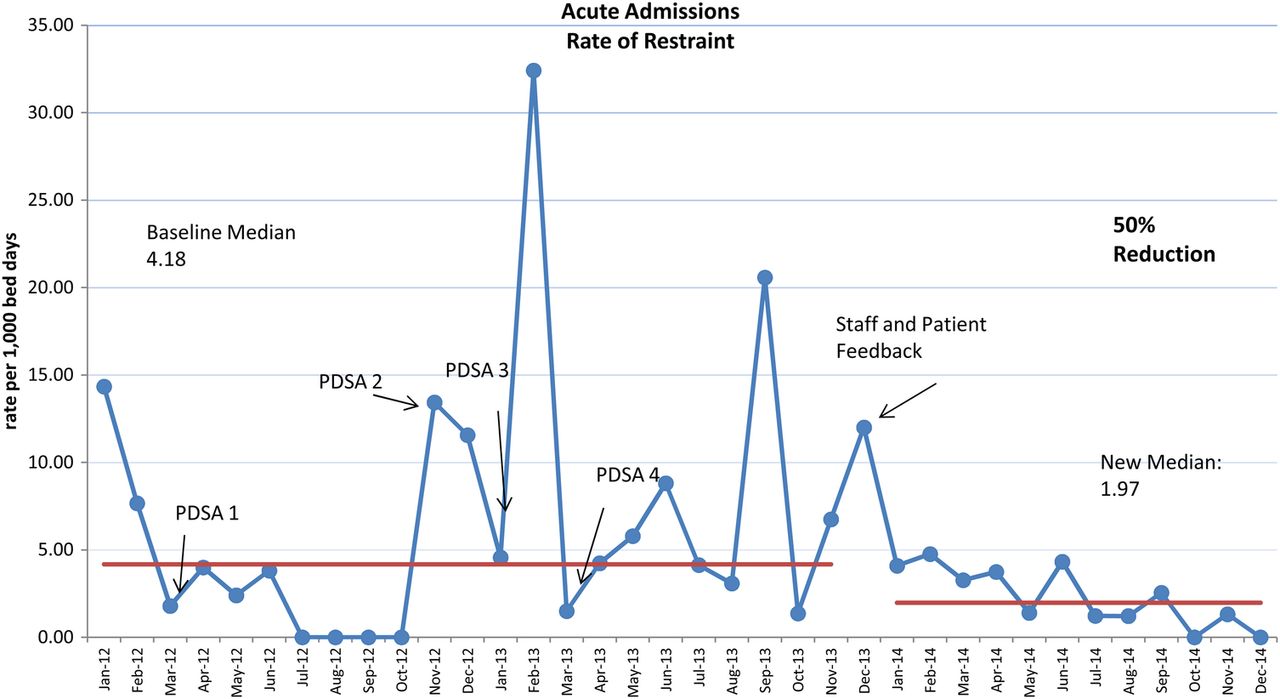
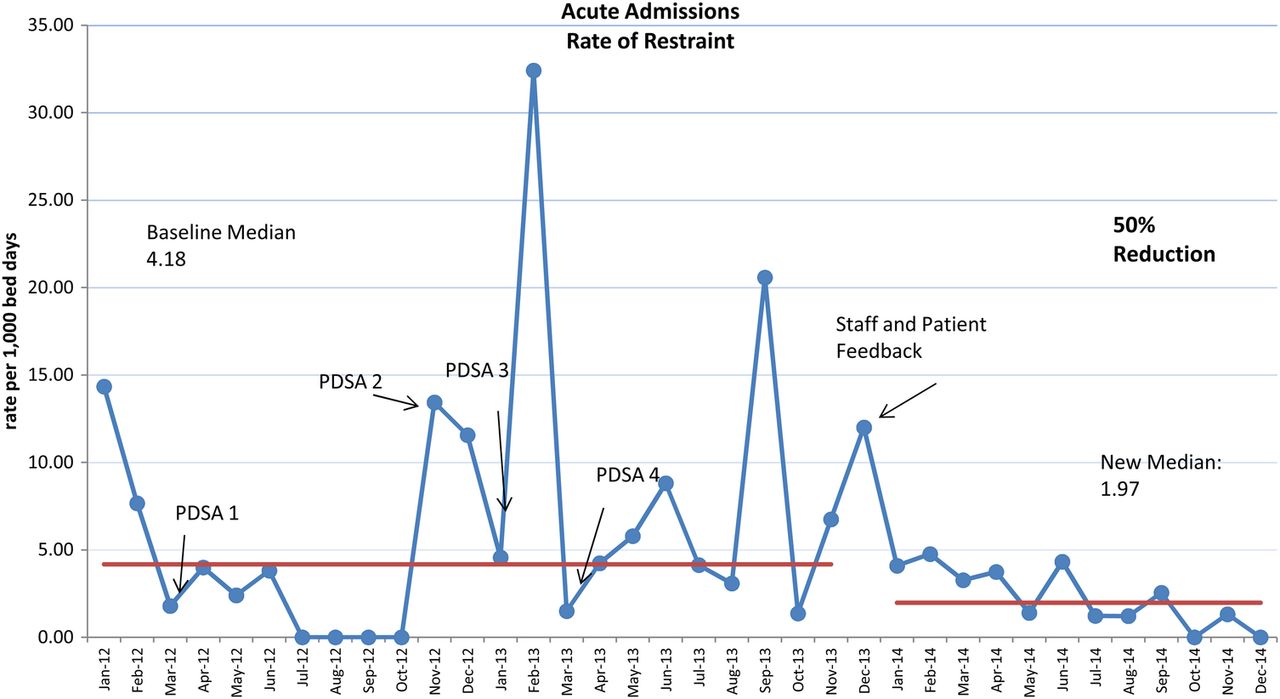
In the year prior (Jan 2011-Jan 2012) to the commencement of the project baseline data was collected retrospectively. This gave us a baseline rate of restraint of 4.18 per 1,000 bed days.
In the six months prior (May-September 2012) to implementing the debrief process, 22% of restraint incidents resulted in a staff debrief.
Design
Our pilot was a 30 bedded Acute Admission ward. The improvement process began with short, on ward, improvement training. This involvement has created an environment where staff and patients are empowered to make small local changes to improve outcomes on their wards.
Many studies have been carried out into what interventions reduce restraint.The five recurring topics that were focused on are: Policy change, Data use, Debrief, Training, and Involvement (Scanlan, 2010, D'Orio et al, 2007, Huckshorn et al, 2014, and Hellerstein et al, 2007)
We decided to look at four of these interventions (data use, debrief, training, and involvement) and apply the improvement model to achieve our aim. Hughes (2008) defines quality improvement as “systematic, data-guided activities designed to bring about immediate improvement in health care delivery in a particular setting” (p. 3–3).
We decided to look at making improvement in all the areas within a short time-frame, as beyond making an improvement we wanted to achieve a fundamental change. A fundamental change will result in an improvement in several measures at once, altering how the system works and will also show improvement into the future. (Langley et al, 2009)
Strategy
For our first PDSA we piloted changes to an existing incident reporting tool. We wanted any changes to the tool to be from a grassroots level as “the best performing healthcare organisations take local ownership of quality measurement, and do so proactively, rather than reactively in response to external demands.”(Mountford & Shojania, 2012 p. 521) We worked with staff to ensure that the information they wanted and we required was collected. We piloted each change within the pilot wards. The information gathered from the form is fed back to staff on a bimonthly basis, and received enthusiastically by them.
For our second PDSA we implemented debriefs. Mayers et al (2010) report that those who experience any form of containment, be it restraint, seclusion, or sedation, found the experience stressful. This stress was further increased if a debrief did not occur following the event. Above all a cultural change is required if sustained restraint and seclusion reduction is to be achieved. This change is from one that restraint is necessary and caused by the actions of the service user to one where restraint is framed as a treatment failure that's reoccurrence can be avoided (Paterson et al, 2013). The debrief process promotes learning from each incident to ensure real time changes occur. Our aim was that all restraint incidents should result in a staff debrief. To initiate the use of debriefs we developed a Principles of Debrief document and provided training in the principles.The debrief process was also added to the Physical Interventions Training curriculum. To measure the use of both staff and patient debriefs we added a section to our Restraint Monitoring Form. We measure and feedback to each ward on their use of debriefs. The uptake and continuation in the use of staff debriefs is variable depending on the ward. We continue to promote the use of debrief through our Physical Interventions Training. Two of our wards are now piloting the use of patient debriefs.
Our third PDSA focused on training. Hughes (2008) suggests that a key strategy for improvement is training and education about the practice intervention and the current problem. Training that focuses on the development of skills, attitudinal change, and de-escalation is essential to reducing seclusion and restraint (Scanlan, 2010). To focus more on de-escalation the theory part of the training included more discussion around de-escalation and the dynamic scenarios were adapted to provide an opportunity for de-escalation which would result in no restraint occurring. The restraint incident information was used ‘live’ to inform the training. The use of de-escalation is now evident in all clinical areas and has become part of the culture within the mental health services.
Our fourth PDSA aimed to increase the use of seated restraint in order to promote the use of a safer restraint position to minimise harm should a restraint occur (D'Orio et al, 2007). Langley et al. 2009 advocated that changing the order of steps could result in an improvement in the process. We therefore changed the sequence of the Physical Interventions Training to promote seated restraint use before floor management. The dynamic scenarios were also altered to give resistance and allow staff to practice de-escalation skills with the eventual aim of a seated restraint. Results from the data collection tool show an increase in seated restraint. The data also shows that following a brief floor restraint many patients are then moved into a seated position.
To gain patient feedback we implemented the Patient Safety Climate Tool designed nationally by the Scottish Patient Safety Programme and VOX (Voices of Experience). The survey is facilitated by two members of the Scottish Patient Safety Team. Feedback was that an increasing amount of patients agree strongly that they feel restraint is carried out safely. The results are shared with the wards and an action plan is developed in conjunction with ward staff. We will continue to carry out the survey on the wards on a six monthly basis.
Finally, we decided to carry out staff focus groups to gather further information from the staff group. We have carried out two staff focus groups to date, using semi-structured questions. Notes were taken throughout the session. When asked what made their wards feel safer one member of staff replied: ‘using PDSAs around change has improved the ward.’ The staff then began to discuss the PDSAs around debrief: ‘Debriefs help us to discuss how incidents can be better managed in the future’, ‘debriefs create an open forum to discuss improving practice’, ‘we have started patient debriefs to discuss incidents’. When asked about how restraints were managed on their wards staff said that ‘sometimes you take it for granted that people know (about restraint), but they don't and it can be frightening’, ‘restraint can make patients feel vulnerable.’ As a result of the focus groups we have initiated the creation of a ward handbook which will highlight the use of restraint and act as a prompt for staff to discuss restraint with patients and carers.
Results
Data was collected throughout the project, at monthly intervals, using an existing tool. The results were variable throughout the project, with reductions seen after PDSA 1 and 2. The variability can mainly be attributed to specific patients. For example, the first and largest peak in restraints was due to a single patient who was misplaced on the ward.
The use of staff debriefs increased to 60% during the final six months (July-December 2014). Staff have valued the debrief process and its use continues to grow.
Within the Acute Admissions ward there was no improvement to the use of the seated restraint of the duration of the project. However, we do know that throughout the service its use has increased by 6%.
Following the implementation of our fourth PDSA and gathering staff and patient feedback a sustained improvement was seen. This improvement was a 50% reduction in the rate of restraint in our Acute Admission ward.
Overall we believe that communication has had the largest impact on the reduction of restraint. During this project communication around restraint has become apparent in areas where it did not happen before. Data about restraints are communicated to staff at all levels. Staff now discuss restraints during the debrief process. During Physical Interventions Training staff are encouraged to use communication through de-escalation and finally staff and patients have been given the opportunity to discuss and feedback about restraints during surveys and focus groups.⇓
{kind=link}
Lessons and limitations
The early involvement of front line staff has been a significant factor in the success of this project. Staff felt as though they had ownership of the project and its results. By reviewing the literature prior to commencement we were also able to gain invaluable insights into how to progress with the project.
Having seen the greatest reduction following staff and patient feedback, it may have been beneficial to start with this.
Unfortunately we could not obtain an accurate baseline for the types of restraints used. Prior to the implementation of the PDSA the type of restraint used was not always recorded. We adapted the tool to ensure this was easier for staff to complete however, we should have addressed this issue earlier.
Due to the small number of restraints by the end of the project it became difficult to measure improvements in areas such as the seated restraint.
There was no extra cost to this project, as we adapted existing systems. It would have been beneficial to consider any financial benefits to the project and we will consider this in the future.
Conclusion
By applying the Quality Improvement Model to the interventions suggested by Scanlan, 2010, D'Orio et al, 2007, Huckshorn et al, 2014, and Hellerstein et al, 2007 we have shown that significant improvement, a 50% reduction in the rate of restraint, can be made. Therefore our aim to reduce the number of restraints was met. Although it is difficult to measure harm, by reducing the number of restraints we are in turn minimising the harm caused by restraints on our Acute admissions ward.
We will continue to apply this model when developing our improvement work in restraint. We will be focusing particularly on patient debriefs and the reduction in the use of prone restraint. Staff are updated on a yearly basis in Physical Interventions and we will hope to sustain and spread this work through the training. As we begin to work with other wards we are seeing encouraging results, suggesting that this process is able to be replicated to the wider Mental Health inpatient environment.
Acknowledgments
All staff in Acute Admissions, all patient participants, Administrative support, and Physical Interventions Trainers.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval Ethical approval was not sought as this project was deemed an improvement project.