Article Text

Abstract
Paediatric grommet insertions are a common ENT procedure which is typically carried out as a daycase procedure. National guidelines exist (NICE CG60) outlining the criteria for grommet insertions. At our institution it was noted that children were experiencing long waits for their grommet surgery with 78% breaching the national 18 week RTT target by time of surgery in the preceding 6 months. 38% of children were attending for surgery with out of date audiograms and as a consequence, due to children no longer meeting the NICE criteria for grommet insertions, 8% of children were being cancelled on the day of surgery.
To improve our waiting times and reduce on the day cancellations we introduced a pilot scheme of “rapid turnover” paediatric day case theatre lists. These lists were accompanied by a pre-operative consent clinic, enabling children not requiring surgery to be cancelled. The theatre lists were run by a senior ENT registrar and had two anaesthetic “pods” i.e. two anaesthetists and two ODPs. This enabled faster turnover of patients and consequently more patients could be operated on per theatre list.
Following our pilot there are no longer any children on the grommet waiting list in breach of the 18 week RTT time. Furthermore, there were no on the day cancellations due to surgery not being indicated. All staff and patients involved were satisfied with the “rapid turnover” lists and subsequently the idea is to be introduced on a regular, 2 monthly basis, to keep waiting times down.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Paediatric grommet insertions are one of the most commonly performed ENT operations. The waiting list for this operation has been spiralling out of control at our institution, Derriford Hospital, a tertiary referral centre for the South West of England, in Plymouth Devon. Our hospital is the largest within the South West covering a population of 700,000 within the immediate catchment area but up to 2,000,000 as a tertiary centre. Senior colleagues within the department were warning of a five to six month wait in late 2015. This breaches the NHS referral to treatment time (RTT) target of 18 weeks leading to financial implications for our department.
This however was not the only problem identified. Grommets are commonly inserted for otitis media with effusion (OME) or “glue ear” and/ or recurrent acute otitis media (RAOM). OME can cause significant hearing loss and both conditions can have a significant impact on quality of life. However, they are both considered to be self limiting conditions with spontaneous resolution with increasing age.1 Coupling this with the long wait for surgery suggested to us that many of the children on our waiting list may actually may no longer warrant their operation by time of surgery. It is widely accepted that audiological assessment demonstrating significant OME is required within three months of surgery to reduce the likelihood of unnecessary operations occurring. However, it has been noted, that within our practice children often do not have an up to date audiological assessment when presenting for surgery.
Children presenting for surgery without an in date audiological assessment at our institution would traditionally under go an assessment on the day of surgery if possible. This can be problematic to both theatre staff and audiological services. Furthermore, this can lead to on the day cancellations creating further financial burden to the department both through fines and through unused theatre time.
Finally, it was noted that theatre lists can be inefficient with long waits between cases due to anaesthetic and recovery times. This often meant that cases were cancelled, again on the day, due to lack of time and only a limited number of cases were being completed per list.
The combination of all of these factors highlights how the current running of our paediatric grommet lists is inefficient with obvious room for improvement.
Background
OME and RAOM are common paediatric ENT disorders. Studies suggest that up to 90% of children, by age 10, will have suffered from at least one episode of OME.1 Most of the time self resolution occurs however, in some children it does not and significant hearing loss ensues. Both conditions can be treated surgically whereby a myringotomy (hole in the eardrum) is made and a ventilation tube (grommet) is inserted.
The National Institute for Clinical Excellence (NICE) have produced guidelines on the management of children with both OME and RAOM whereby criteria for grommet insertion are outlined. They indicate when a child should be considered for surgical intervention: Persistent bilateral OME over a period of 3 months with a hearing level in the better ear of 25–30 dBHL or worse averaged at 0.5, 1, 2 and 4 kHz or exceptionally, persistent bilateral OME with a hearing loss less than 25–30 dBHL where the impact of the hearing loss is judged to be significant.2
Such surgery is typically a day case procedure under general anaesthetic. Generally speaking grommet insertion is a relatively short procedure however anaesthetic issues can slow down patient flow and limit the number of cases completed per list.
Within the NHS many performance targets exist to increase efficiency. One of these is the consultant-led referral to treatment time (RTT). This measurement was introduced in 2008 as the result of unacceptably long waiting times within the NHS. It is a complex system with many rules. However, the basics can be explained as follows. Once a referral is made to a consultant-led service a clock is started. This clock continues until the first treatment occurs. The Department of Health have set a limit for the RTT of 18 weeks to ensure patients are not kept waiting for definitive treatment for too long. In the case of children needing grommet insertions the RTT clock stops when the children undergo surgery.3 Therefore, the waiting time for surgery from listing is paramount to the RTT. Breaching the 18 week RTT, with no clinical cause, has large financial consequences on departments. By reducing the time from addition to waiting list we can aim to ensure all children requiring grommets, within our institution, are treated within the 18 week target.
Baseline measurement
At our institution background data on paediatric grommet containing cases, for the preceding 2 years (November 2013 – November 2015), demonstrated that on average we list 14 children for grommet surgery each month. During this time our institution carried out 264 grommet operations with 131 cancelled procedures. Of these cancellations 25 (8%) were never rebooked as surgery was no longer indicated. The remaining cancellations eventually went on to have the operation completed (28% of children were cancelled at least once prior to having grommets inserted).
The average waiting time for surgery from being added to the waiting list was 90 days (range 5–214). This does not include the time spent waiting from referral until first appointment with the ENT team. When this factor is considered, in the 6 months prior to our project, from January 2015 to July 2015, the average RTT time was 21 weeks with 78% of children breaching the 18 week target by time of surgery. This financial penalties for the department.
Audit of children who had undergone grommet insertion in the preceding 6 months (n=64) demonstrated that, on average the time between the child's last audiogram and date of surgery was 70 days (range 0- 317). This meant that 38% of children had an audiogram older than, the widely accepted limit of, 90 days by time of surgery.
Furthermore, our data demonstrated that, according to average case length, only 5.8 grommet insertions could be carried out on one theatre list. Coupled with the high rate of on the day cancellations this helps to explain why there has been such a problem with the paediatric grommet waiting list in our institution. An assessment by the finance department demonstrated a mean loss to the hospital of £24 for every grommet case performed.⇓
American Society of Anaesthesiology Physical Status Classification System (adapted from https://www.asahq.org/resources/clinical-information/asa-physical-status-classification-system)4
Design
After identifying the aforementioned issues and reviewing background data it became apparent that something needed to be done to increase efficiency of paediatric theatre lists, reduce waiting times for surgery and reduce on the day cancellations. A group of staff from our department (an ENT registrar, ENT CT2 and consultant, in conjunction with two managers and theatre teams) developed and proposed to pilot paediatric grommet “rapid turnover lists”. These streamlined theatre lists, for grommet insertions only, aim to achieve more timely turn around of patients increasing the number of operations performed per list.
The lists targeted the day case patients who are ASA (American Society of Anesthesiologists – see table 1 for full explanation) grades 1 or 2. This group of patients was chosen as they provide less concern for the anaesthetic team and are more likely to go home on day of surgery. The lists were designed to have between 8 and 12 patients and were run by a senior ENT registrar.
To ensure efficiency and increase patient turnover each list was allocated a senior anaesthetic registrar and an anaesthetic consultant along with two operational department practitioners (ODP). This enabled us to have two “anaesthetic pods” available meaning that whilst one patient was being recovered from the anaesthetic another could be in the anaesthetic room being anaesthetised.
Increased turn around of a paediatric theatre list also required sufficient staffing levels in theatre admissions and recovery. We therefore recognised that recovery staffing may need to be increased on the days that a “rapid turnover list” was running.
Each list had a designated consent clinic 2 weeks beforehand. The pre-operative consent clinic was designed to minimise and tackle the issue of on the day cancellations. The clinic was carried out by the ENT registrar who then went on to perform the “rapid turnover” list. Each patient was allocated 15 minutes and assessment was proforma based, in keeping with the NICE guidelines for grommet surgery (CG60). Any child not meeting these criteria was cancelled or discussed with a consultant if electing to proceed off guidelines. Furthermore, the clinic allowed us to check that children had an up to date audiogram (within 90 days) demonstrating the ongoing need for surgery. If this was not the case a tympanogram was peformed to confirm OME was still present. Children no longer requiring surgery or not meeting the NICE criteria were cancelled at the consent clinic instead of waiting until the day of surgery. Finally, a standardised, pre-populated consent form was used. Following consent, the patient and family were directed to the paediatric day case unit for familiarisation and anaesthetic pre-assessment.
The aim of this project was to reduce both waiting times and on the day cancellations for paediatric grommet insertions within our institution by introduction of “rapid turnover lists” and consent clinics. We planned to re-audit our data following a short pilot (3 theatre sessions) to identify any reduction in 1. RTT for our paediatric grommet waiting list and 2. on the day cancellations due to surgery not being indicated.
Strategy
After designing the paediatric grommet “fast list” initiative, all stakeholders were identified and the project was discussed with all individually to gauge opinion and refine the intervention. This included anaesthetics, theatre staff, audiology, outpatient clinics, the ENT team and managerial staff. By involving the whole multi-disciplinary team agreement was obtained to conduct a trial of intervention. The trial period would involve having 3 “rapid turnover lists” with 8 per list, involving 2 different surgeons. 4 consent clinics would occur, with the extra clinic being used to back fill any cancellations.
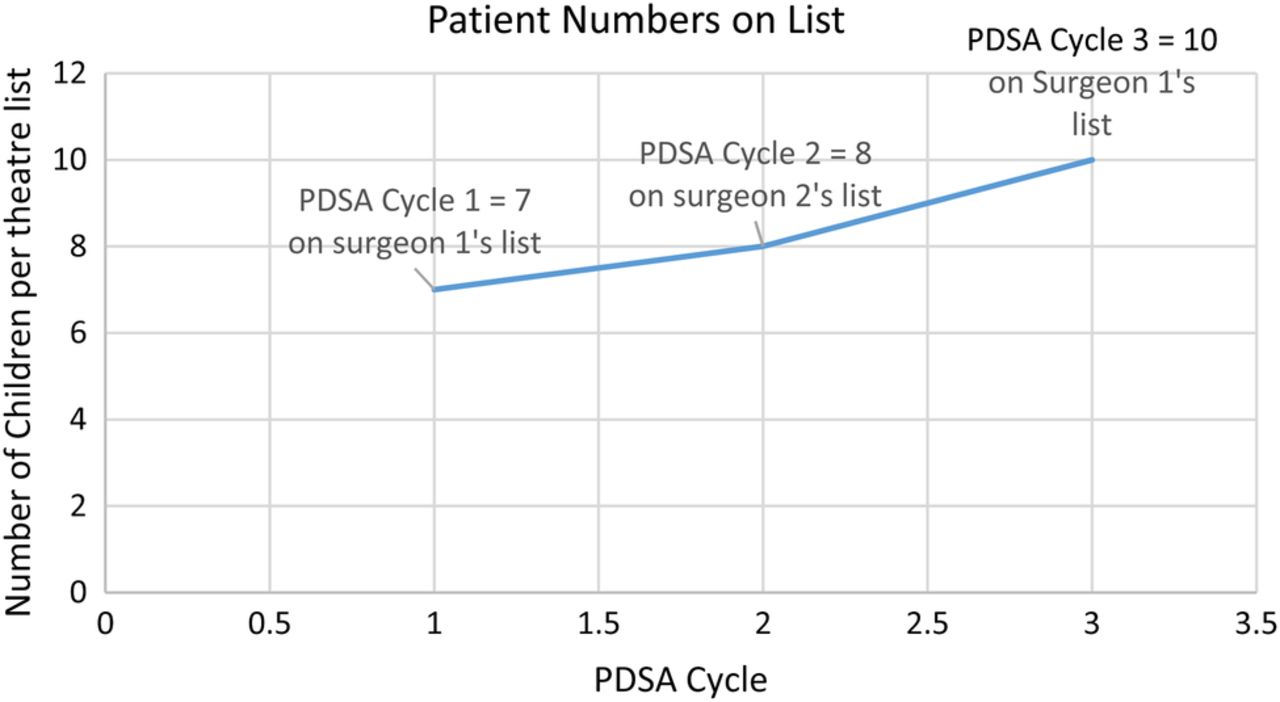
PDSA Cycle 1: The first theatre list had 8 patients allocated with a preceding consent clinic. At the consent clinic 3 children were cancelled due to surgery no longer being indicated. 1 patient was cancelled on the day of surgery due to an active upper respiratory tract infection. This left 7 patients and review of the list demonstrated that, on average, it took 24 minutes of theatre time (anaesthetic and surgical) per patient. Consequently, the list finished at 1045, indicating capacity to expand the list. Feed back was sought via the formalised WHO debriefing process. Agreement was reached to expand the list for the named surgeon for that day. Other points raised was staggering patient arrival times to smooth flow, this too was taken forward.
PDSA Cycle 2: 8 children attended the pre-operative consent clinic with 4 being cancelled at this stage. On the day of the theatre list no child was cancelled and 8 underwent successful grommet insertion. We introduced staggered start times during this cycle as suggested by team members during the first cycle. This improved efficiency with admissions and enabled the list to start earlier due to the anaesthetic team only seeing 4 of the children first thing in the morning. The other children were admitted and reviewed by the anaesthetist whilst the list was ongoing. During the list the general surgeons had to perform and emergency appendicectomy within our theatre. Despite this the list was completed on time. The first two cycles demonstrated that having only 8 children on the list was not using the theatre time to full capacity, therefore, reducing the cost effectiveness of our initiative. Consequently, agreement was reached to expand the list for both surgeons taking part in the pilot.
PDSA Cycle 3: Following the success of the first two pilot lists, in agreement with all staff involved, the next list had more patients to ensure maximal utilisation of allocated time. 11 children attended the consent clinic with 1 being cancelled at this point. Subsequently, 10 children went on to have grommets inserted during the last pilot list (see figure 1). Once again the list finished 45 minutes early. Feedback supported this to be the desired enduring strategy. Although spare capacity was noted, it was felt this allowed flexibility in the future should there be external factors delaying patient flow.⇓

{kind=link}
Run chart demonstrating how patient numbers on each theatre list changed with PDSA cycle over time
Results
During the pilot 25 children successfully underwent grommet insertion. Both the staff involved and the parents were happy with the consent and surgical process. There were no on the day cancellations (0%) as children not requiring surgery were cancelled at the consent clinics (24%). This is in contrast to the 8% of on the day cancellations seen prior to our project. Before these theatre sessions 78% of children were in breach of the 18 week RTT target by the time of surgery. However, following our quality improvement project there are currently no children on the waiting list, for grommet insertion, in breach of the 18 week target. This project has therefore clearly helped to reduce financial penalties received by our department and improve waiting times for grommet insertions.
Financial assessment of the enduring 10 patient ‘rapid-turnover' grommet list showed a £3255 increase in gross income generation per list when compared to the 5.8 case/list baseline.
Lessons and limitations
During this project it became apparent that by involving all staff groups from the outside led to smooth implementation of the pilot. Clear communication and discussions meant that all staff involved were happy to carry out the trial period and continued to improve the project as time went by.
The main limitation identified during this process was ensuring that the children listed were only having grommet insertion and no other associated surgery such as adenoidectomy. Commonly within paediatric ENT populations patients have multiple operations, such as grommets and tonsillectomy, performed during the same anaesthetic. Ensuring patients included in this study were only having the one procedure was challenging, especially as at times they were incorrectly listed. The theatre and managerial staff had to work hard to sieve through the waiting list, identifying appropriate patients.
The trial lists and consent clinics were found to be a success and are a sustainable option to continue to keep waiting times down for our paediatric grommet population.
Conclusion
The introduction of “rapid turnover” paediatric grommet have proven to be a sustainable solution to the problem of long waiting times at our institution. There is little in the literature supporting our conclusion. However, one study conducted by Al-Hussaini et al evaluating the number of grommets performed following the introduction of the NICE guidelines CG60 (as used in our project) did not reduce the number of grommets performed between 2000 and 2010 within the UK (p>0.5).5 This is contradictory to our project, as by strictly adhering to these NICE guidelines our team cancelled 24% of children who were listed for grommet insertion prior to surgery.
Following the success of the pilot our institution plans to introduce these “rapid turnover” lists regularly, having one at least every 2 months. Each of these lists will have 10 patients. If the waiting list once again becomes overstretched we will aim to run extra rapid turnover lists to prevent the issues highlighted prior to this project occurring once more. In the long term, we aim to get the consent clinics run by ENT nursing staff and to use disposable, single use grommet sets to increase turnover and reduce work on the theatre support staff.
If required, the template of these “rapid turnover” theatre lists could be extrapilated and used in other minor day case surgeries, both within ENT and other specialties. However, this would depend on other institutions having capacity in a similar set up to ours with and available of appropriate staffing levels.
Acknowledgments
James Rainsbury, Sarah Wimlett, Leanne Chapman, Emma McCurdy, Andrea Anstey, Rachael Buller and the staff of The Plym Children and Young People's Theatre Unit, Derriford Hospital.
Footnotes
Declaration of interests non declared
Ethical approval This work was deemed an improvement study and local policy meant that ethical approval was not required.