Article Text

Abstract
Previous qualitative studies suggest a lack of maternal confidence in care of their newborn child upon discharge into the community. This observation was supported by discussion with healthcare professionals and mothers at University College London Hospital (UCLH), highlighting specific areas of concern, in particular identifying and managing common neonatal presentations. The aim of this study was to design and introduce a checklist, addressing concerns, to increase maternal confidence in care of their newborn child.
Based on market research, an 8-question checklist was designed, assessing maternal confidence in: feeding, jaundice, nappy care, rashes and dry skin, umbilical cord care, choking, bowel movements, and vomiting. Mothers were assessed as per the checklist, and received a score representative of their confidence in neonatal care. Mothers were followed up with a telephone call, and were assessed after a 7-day-period. Checklist scores before as compared to after the follow-up period were analysed. This process was repeated for three study cycles, with the placement of information posters on the ward prior to the second study cycle, and the stapling of the checklist to the mother's personal child health record (PCHR) prior to the third study cycle.
A total of 99 mothers on the Maternity Care Unit at UCLH were enrolled in the study, and 92 were contactable after a 7-day period. During all study cycles, a significant increase in median checklist score was observed after, as compared to before, the 7-day follow up period (p < 0.001). The median difference in checklist score from baseline was greatest for the third cycle.
These results suggest that introduction of a simple checklist can be successfully utilised to improve confidence of mothers in being able to care for their newborn child. Further investigation is indicated, but this intervention has the potential for routine application in postnatal care.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
A proportion of mothers lack confidence in care of their newborn child. Discussions with members of the multi-disciplinary team further supports this, with general practitioners noticing maternal anxiety in neonatal care at six week postnatal checks and midwives echoing this on the wards and on community visits. A team of medical students previously trained in quality improvement led by a senior Consultant in Obstetrics and Fetal Medicine, investigated this problem on the postnatal ward at University College London Hospital (UCLH). UCLH is a tertiary centre hospital with a Maternity Services Department located in the Elizabeth Garrett Anderson Wing. The postnatal ward contains 45 beds and has a fast turnover of patients.
The mothers were interviewed and their knowledge of neonatal care issues was assessed. The analysis revealed eight repeating themes of concerns: breast-feeding, jaundice, nappy care, rashes, umbilical cord care, choking, stool care, and vomiting. It was found that, not surprisingly, primiparous mothers appeared more anxious than mothers with previous birth experience. Despite the availability of NHS-provided and private antenatal classes, all concerns were still not met. There is currently no method of determining or quantifying maternal confidence and knowledge in care of the newborn child prior to discharge. Having an intervention at this stage may help to support parents in their transition home following discharge.
Background
Maternal confidence is a key theme influencing maternal experience post-parturition, particularly after discharge from the maternity unit. Existing tools to improve maternal confidence aim to increase awareness of their newborn's health, subsequently reducing maternal apprehension.1 One such tool is the Personal Child Health Record (PCHR), which is well used by mothers from different backgrounds. This provides a means by which parents can be more involved in their child's healthcare and includes educational material for families on their child's health.2 However, factors such as socioeconomic status may influence the use and effectiveness of PCHRs.3 Moreover, despite implementation of PCHRs, mothers of newborns with health conditions may feel loss of support from the maternity and neonatal team post-discharge, indicating that there is an opportunity for further intervention.1
A checklist assessing maternal confidence and concerns of mothers could provide a solution, as it provides a medium of communication between parents and caregivers. Such a checklist may increase maternal internal and empirical awareness, empowering them to identify their newborn's needs;1 an important constituent of the process of becoming a mother.4 Improving information giving and thus parental confidence has been explored in previous studies, however the literature overwhelmingly focuses on interventions for parents of preterm babies.5 In addition, numerous studies have specifically focused on parental experiences of the service and discharge,6 while studies that looked into empowering mothers and improving neonatal care focused on breastfeeding.7 ,8 To our knowledge this is the first study that takes into account a broad range of concerns for parents and how to improve confidence and thus care of their children.
A market research study was undertaken to aid us in the design of a checklist intervention with an aim to determine common concerns of mothers in respect to care of their newborn child. In our market research, 30 mothers at UCLH postnatal ward were interviewed over a 7-day period. Interviews were structured using a pre-designed questionnaire. Mothers were asked about their previous birth experiences, concerns regarding care of their newborn child, and were questioned as to what resources they need in preparation for discharge home. Additionally, mothers were encouraged to express their concerns on the following topics: feeding, sleeping, nappy changing, rashes, and jaundice, and were questioned as to how they identify their baby to be unwell, and how they would respond in such a situation. Finally, the mothers were invited to help us create a checklist that will address the most common concerns and improve maternal confidence in neonatal care.
From the 30 mothers interviewed, 63% (19/30) of the mothers were primiparous, and 17% of mothers had reported a single miscarriage in the past. 67% of mothers reported a lack of confidence in feeding their child, with particular reference to latching on and expression of milk during breastfeeding. A high proportion of mothers reported confidence in the topics of sleeping (93%) and nappy changing (86%); only 23% of mothers reporting concerns for neonatal jaundice. However, over 40% expressed concerns over identifying rashes, and distinguishing severity of different rashes. These mothers suggested that photographic or visual aids of common rash presentations would alleviate their concerns. Posing open questions to the mothers was effective in highlighting additional concerns of mothers, such as umbilical cord care. In conclusion, working in partnership with the mothers on the ward, using a patient-centred approach, helped us identify key themes where more information should be provided.
Based on the relevant background taken from literature search and from market research the checklist intervention was designed. This checklist included eight key themes identified as common and important in neonatal healthcare, including feeding, jaundice, nappy care, dry skin and rashes, umbilical cord care, choking, bowel movements and stool care, and vomiting. The checklist was also designed to collect key demographic factors including age and ethnicity of number, first-newborn status, and previous-miscarriage status.
To guide our quality improvement study we followed the commonly utilised SMART criteria. The specific goal was to increase maternal confidence in neonatal care, which was measured using a numeric score on a checklist that addresses eight key concerns. It is achievable and relevant as there is currently no method of determining maternal confidence and knowledge prior to discharge. Having an intervention at this stage would help to support parents in their transition home following discharge and personalise care. We conducted this project over four months to assess the significance of this intervention.
Baseline measurement
In order to take baseline measurements, a team of seven medical students previously trained in quality improvement approached mothers on the Maternity Care Unit at UCLH. 44 mothers gave informed consent to take part in the study, and after patient demographics were taken, the mothers gave permission for a follow-up phone call seven days after consent was taken. After the 7-day follow up period, mothers were called and assessed for their score according to the checklist criteria. The maximum score on the checklist was eight, representing confidence about managing eight common neonatal situations. The minimum score was zero, signifying that the mother would like to receive more information on all eight common presentations in neonatal care. The final score was expressed as a percentage of the total score out of eight. All data was collected using Excel by Microsoft, Version 15.9 (Redmond, Washington). Statistical analysis of checklist score and patient demographics was performed using IBM SPSS Statistics for Windows by IBM Corp., Version 22 (Armonk, NY). A total of 33 mothers were successfully followed up. The 33 mothers had a median checklist score of 75, with an interquartile range of 62.5–87.5.
Design
Our intervention involved the introduction of a checklist given to mothers on the postnatal ward to invite questions directed to healthcare professions, both in the hospital and in the community, in order to provide personalized access to care and information. The checklist encompassed eight thematic questions with illustrative examples focusing on the main concerns highlighted by mothers during our background research. The responses were scored out of eight using a yes or no scale to address maternal knowledge of managing common issues in newborn care. Mothers were handed the checklist together with the PCHR and were encouraged to seek further information on any of the aspects that they did not feel confident with. After a period of seven to ten days, in which they would have had contact with healthcare professionals or independent research to address their queries; we followed up mothers by a phone call and repeated the eight questions. This allowed us to assess whether their knowledge had improved after the checklist intervention had been implemented by comparing the initial score to the follow-up score. In addition, we asked mothers to be involved in a qualitative evaluation of our checklist intervention, to receive feedback on the study.
Since the PCHR is a national programme, the addition of the intervention as an extra page within the book would foreseeably allow it to have a national impact in the long-term. It would be a sustainable resource, as it is completely independent of the mother's socio-economic status and background, providing no extra financial cost on her behalf and ensuring that each mother receives the opportunity to maximize her knowledge on basic neonatal care.
Strategy
We conducted a total of three PDSA cycles. Each intervention (or PDSA cycle) was conducted with an interval of approximately two to three weeks. Data collection was repeated on the postnatal ward after each intervention, prior to beginning the next cycle.
PDSA cycle 1 intervention:
Implementation of the 8-question checklist handed to mothers before discharge from a postnatal ward was designed to improve maternal knowledge of the management of common issues in neonatal care. The checklist addresses eight key topics with illustrative examples to prompt mothers to seek further information from healthcare professionals in the hospital and the community where necessary. Mothers are then followed up seven to ten days after discharge and their knowledge and confidence of caring about their baby was assessed. The aim was to improve mother's confidence and knowledge, since the checklist would allow them to tailor their questions to healthcare professionals and/or independent research towards areas they feel less confident with.
PDSA cycle 2 intervention:
Posters and leaflets around the post-natal ward in both staff-only areas and areas with patient access were used to raise awareness of the project on the ward, invite further discussion between midwives and the mothers, and most importantly inform the mothers of the checklist intervention about the study and prompt them to seek information before the checklist is given.
PDSA cycle 3 intervention:
The checklist was stapled to the PCHR and given to mothers as an integral part of the PCHR. The aim was to ensure the checklist would be readily accessible for the mothers at all times, and allow them to go through the topics discussed in the checklist with their doctor or a midwife when assessing other aspects of the PCHR.
Supplemental material
Results
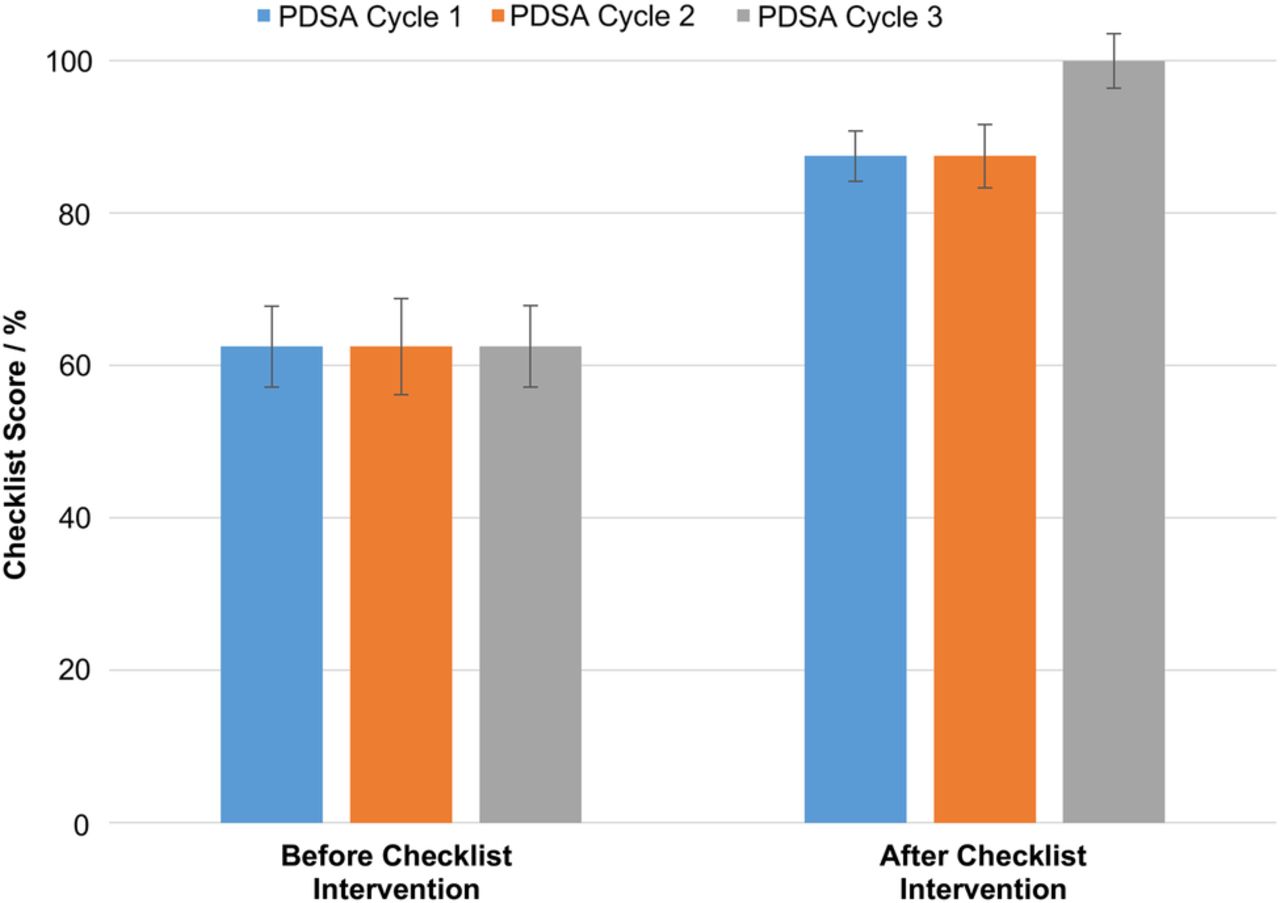
After the first PDSA cycle, the Wilcoxon Signed Rank test determined a significant increase (p<0.001) in median checklist score in the intervention group after follow up (n=30, median=87.5, IQR=75–100) as compared to before (n=37, mean=62.5, σ=25.6). Linear regression showed the only variable significantly associated with the checklist score to be the first-newborn status, in the control group of mothers (p=0.031) and the checklist intervention group prior to the 7-day follow up (p=0.004). However, no variables were significantly associated with the checklist score in the intervention group after the 7-day follow up, after adjustment for age of mother, ethnicity, and previous miscarriages.
After the second PDSA cycle, the Wilcoxon Signed Rank test determined a significant increase (p<0.001) in median checklist score of mothers after the 7-day follow up (n=32, median=87.5, IQR=75–100) as compared to before follow up (n=32, median=62.5, IQR=25–75). In contrast to the first PDSA cycle, linear regression showed that no variables were significantly associated with the checklist score in the intervention group, before or after the 7-day follow up, after adjustment for age of mother, ethnicity, and previous miscarriages. Similarly, after the third PDSA cycle, the median checklist score increased significantly (p<0.001) in mothers 7-days after checklist intervention (n=30, median=100, IQR=87.5–100) as compared to before follow up (n=30, median=62.5, IQR=37.5–75). As such, the difference in median of mothers' checklist scores before as compared to after the study period was greatest for PDSA Cycle 3 than previous Cycles, suggesting that the checklist had the greatest effect on maternal confidence by Cycle 3. However, linear regression determined the first-newborn status to be significantly associated with both mothers before (p=0.001) and 7 days after (p=0.003) the checklist intervention, after adjustment for age of mother, ethnicity, and previous miscarriages. All statistical significance was calculated to a 95% confidence interval.⇓

{kind=link}
Lessons and Limitations
A potential challenging aspect of this project was the incorporation of different healthcare professionals who provide care at the post-natal ward, mainly clinicians and midwifes. However, both parties saw the potential positive impact of the checklist intervention and participated fully. The response from the mothers were overall very positive and the mothers described it as a “really useful and excellent idea.” The pictures of jaundice and different common rashes appeared to be beneficial, and one mother commented how it helped her to “feel empowered to ask questions herself.”
The checklist was designed based on the in-depth discussions with the mothers in our market research and the findings of our literature search. Moreover, our project supervisor and senior Consultant in Obstetrics and Fetal Medicine ensured the checklist was clinically relevant. However, our checklist was not validated in a separate study with patient focus groups and that certainly represents the limitation of our project, which we plan to address in the future.
We have recorded that some mothers misplaced or lost the checklist, therefore were unable to use it to guide their community midwife visits. We believe that this logistics problem could be overcome by incorporating the checklist into the PCHR in the future. This could also provides a means of scalability and sustainability as the PCHR is a standardised tool given to all mothers nationwide, aiming to improve maternal confidence on a wider scale. Therefore, we plan to work in partnership with the community midwives and general practitioners, in order to ensure the sustainability of our project by incorporating the checklist as an integral component of the PCHR.
Our project is unique as it specifically looks how to implement a patient-centered care approach. Empowering mothers first hopes to increase the patient activation measure and allow mothers to be more involved with the care of their child. Furthermore the intervention implemented is not restricted to the UCLH trust, but can be expanded nationwide as it already incorporates the use of the PCHR which is given to all mothers in the UK. This study can be expanded to other studies and with enough evidence become part of standard practice.
The checklist was developed, in part, from the concerns of the mothers and can be expanded to other NHS trusts and potentially nationally. While the ranking of the key themes of the checklist may change in the different locations in the country it should still achieve the overall outcome of improving maternal confidence.
Conclusion
Our project aimed to increase maternal knowledge in care of their newborn child through a checklist intervention given to the mothers before discharge from a post-natal ward. The first stage was problem identification, followed by a study about most common concerns of newborn mothers that was used for the creation of a checklist intervention. The checklist intervention was successfully implemented in three separate PDSA cycles. The results showed the checklist brought in positive change, as evidenced by a statistically significant improvement in maternal knowledge following its implementation, evidenced by a statistically significant improvement in maternal confidence in all three cycles compared to the baseline. We found that the optimal method of checklist administration was together with the PCHR, as performed in our final PDSA cycle.
A similar recent study investigated the implementation of a parent pack ‘Train-to-home’, demonstrating a significant reduction in the number of out of hours emergency department presentations in the intervention group.9 However the topics are neonate-specific, not covering the broad range of the more basic aspects of neonatal care that mothers have reported a lack of confidence in. Nevertheless, in keeping with our findings it suggests the benefit of empowering parents with regard to neonatal care.
In conclusion, the checklist represents a standardised method with wide applicability, as it may enable high quality care to mothers, regardless of their background. Since it addresses simple and common concerns, steering away from complex medicalisation, it could be used as a simple and readily available tool to improve patient experience.
Acknowledgments
This manuscript is the sole work of its authors. All authors contributed equally.
Footnotes
Declaration of interests All authors have contributed significantly to the conception, design, and acquisition of data, analysis and interpretation of data, or drafting the article and revising it critically for important intellectual content. We have read and understood the BMJ Group policy on declarations of interests and declare the following interests: none.
Ethical approval This work was carried out under the auspices of the Women's Health Divisional Service Improvement strategy. Local policy for service improvement work meant that ethical approval was not required. The project was supervised throughout by Dr Melissa Whitten, Consultant Obstetrician. Approval was gained from the Divisional Clinical Director and Divisonal Clinical Governance team prior to proceeding with the work.