Article Text

Abstract
About one-quarter of all long-term care (LTC) residents are transferred to an emergency department (ED) every 6 months in Ontario, Canada. When residents are unable to describe their health issues, ED staff rely on LTC transfer reports to make informed decisions. However, transfer information gaps are common, and may contribute to unnecessary tests, unwanted treatments and longer ED length of stay. London Health Sciences Centre, an academic hospital system in London, Ontario, partnered with 10 LTC homes to improve emergency reporting of their residents' reason for transfer and baseline cognition. After conducting a root cause analysis, 7 of 10 homes implemented a standard minimum set of currently available transfer forms, including a computer-generated summary of resident’s most recent interRAI functional assessment. Results were analysed using statistical process control charts and data were posted on a public website (LondonTransferProject.com). The documentation rate of ‘reason for transfer’ improved from 61% to 84%, and ‘baseline cognitive status’ improved from 4% to 56% across all 10 homes. These results suggest that transfer communication can be improved by codesigning and implementing solutions with ED and LTC staff, which build upon current reporting practices shared across multiple LTC organisations.
- communication
- emergency department
- nursing homes
- quality improvement
- transitions in care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
Older adults use a greater proportion of emergency department (ED) services than other age groups. Those who live in long-term care (LTC) homes are among the highest users. In Ontario, about 25% of all LTC residents visit an ED at least once every 6 months.1 Hospital staff rely on accurate personal health information to provide safe, high-quality care. However, many residents have difficulty describing health information. In the absence of accompanying family or caregivers, ED staff look for key clinical details in LTC transfer reports.2
Canadian and international studies have found consistent and alarming information gaps in LTC transfer reports.3–5 These gaps prevent ED staff from making informed decisions, especially when patients have dementia. As a result, patients are exposed to quality and safety risks from service duplication, unnecessary diagnostic tests and undesired treatments.4 6 For example, residents with dementia who lack transfer documentation spend more time in the ED, which may increase morbidity and mortality.3
London Health Sciences Centre (LHSC) is a two-site hospital organisation in Ontario, Canada, that serves 23 LTC homes in London-Middlesex County. In 2015, the ED served over 2400 LTC residents—about 200 per month. Fifty per cent of LTC residents in the ED were discharged home; 25% returned to the ED within 30 days.
In London-Middlesex County, LTC homes are operated by non-profit and for-profit organisations. These homes share common characteristics that affect resident transfers: 62% of LTC residents have dementia, and 14.5% have suffered a fall in the past 30 days.7 Most LTC homes are staffed primarily by personal support workers, with a limited number of nurses working each shift. When a resident requires emergency transfer, nurses usually complete transfer documentation at an electronic medical record (EMR) workstation away from the resident’s room.8 Communication gaps are exacerbated by the combination of low staffing, inefficient documentation processes and residents with complex needs.
We defined transfer communication gaps by asking ED clinicians (22 physicians and 23 nurses) to rank 20 items from a systematic review as high, medium or low importance.2 4 5 The highest priority details requested were ‘reason for transfer’ and ‘baseline cognitive status’, which is consistent with other studies.2 4 Therefore, the aim of this project was for 90% of LTC emergency transfers to LHSC to include the resident’s reason for transfer and baseline cognitive status by 30 June 2016. We believed an aim of 90% was difficult but possible, and would provide the tension needed to redesign the transfer communication process.
Background
The prevalence of information gaps had not previously been studied at a local level. However, Cwinn et al4 described the extent of the problem at The Ottawa Hospital, which has similar contextual factors to LHSC: both are multisite, academic teaching hospitals in Ontario that serve more than 20 LTC homes.4 Using the National Ambulatory Care Reporting System database, they identified LTC residents transferred to The Ottawa Hospital’s ED within a 6-month period. Out of 457 transfers, more than 85% of reports were missing at least one essential data element. Baseline cognition was not described in 37% of transfers, and baseline orientation was missing in 47% of cases; 38% of patients without documented baseline cognitive function received a CT head scan; and 8% of patients with dementia were sent to the ED without a documented reason for transfer.4 Similar findings were seen in an Australian study of transfer documentation. Only 40% of residents with decreased level of consciousness had a documented baseline cognition. Patients who presented with information gaps were more likely to receive a CT head scan and concomitant radiation exposure.3
Previous efforts to address this issue have been met with limited success. A systematic review of transitional care interventions found that medication lists and advance directives may be better communicated using standardised forms. Unfortunately, there was limited evidence of successful change adoption by LTC staff.9 In a study of a novel standardised form, the quality of documentation improved by 19%, but the form was sent in only 32% (23/72) of transfers.10 Similar results were found when information was communicated using a proprietary web-based electronic discharge tool. While LTC staff were able to send necessary information using fewer pages, and ED physician satisfaction improved, the web-based tool was used in only 26% (78/276) of transfers.11
These studies shared two common themes. When EDs communicated what information was needed in a standardised form, LTC staff were more likely to include the information in transfers. However, successful documentation was limited by the ability and motivation of LTC staff to use the new process. Interestingly, these studies did not describe how LTC staff—the change agents—were involved in analysing current transfer processes or creating and testing solutions. This suggests that LTC staff engagement is necessary to create sustainable improvements in ED transfers.
Baseline measurement
Transfer packages were audited using a prospective, non-random convenience sample in the ED and inpatient general medicine units from October 2015 to July 2016. Geriatric emergency management nurses and patient care facilitators pulled transfer packages from patient charts at discharge, which were reviewed weekly with a standardised checklist. ‘Reason for transfer’ was considered present if any chief complaint was documented. ‘Baseline cognitive status’ was considered present if one of the following functional descriptors from the validated interRAI 2.0 Home Care assessment was documented: decision-making, memory, consciousness/awareness, or communication/comprehension.
Baseline data were collected from October to December 2015, and 50 transfers from any LTC home were reviewed. Reason for transfer was documented in 63% of cases, and baseline cognitive status was documented in only 7% of cases. See online supplementary figure 1 .
Supplementary Figure 1
Design
Our study included 10 LTC homes in London-Middlesex and two ED campuses at LHSC. Each LTC home was independently owned and operated. Nine homes used the same EMR.
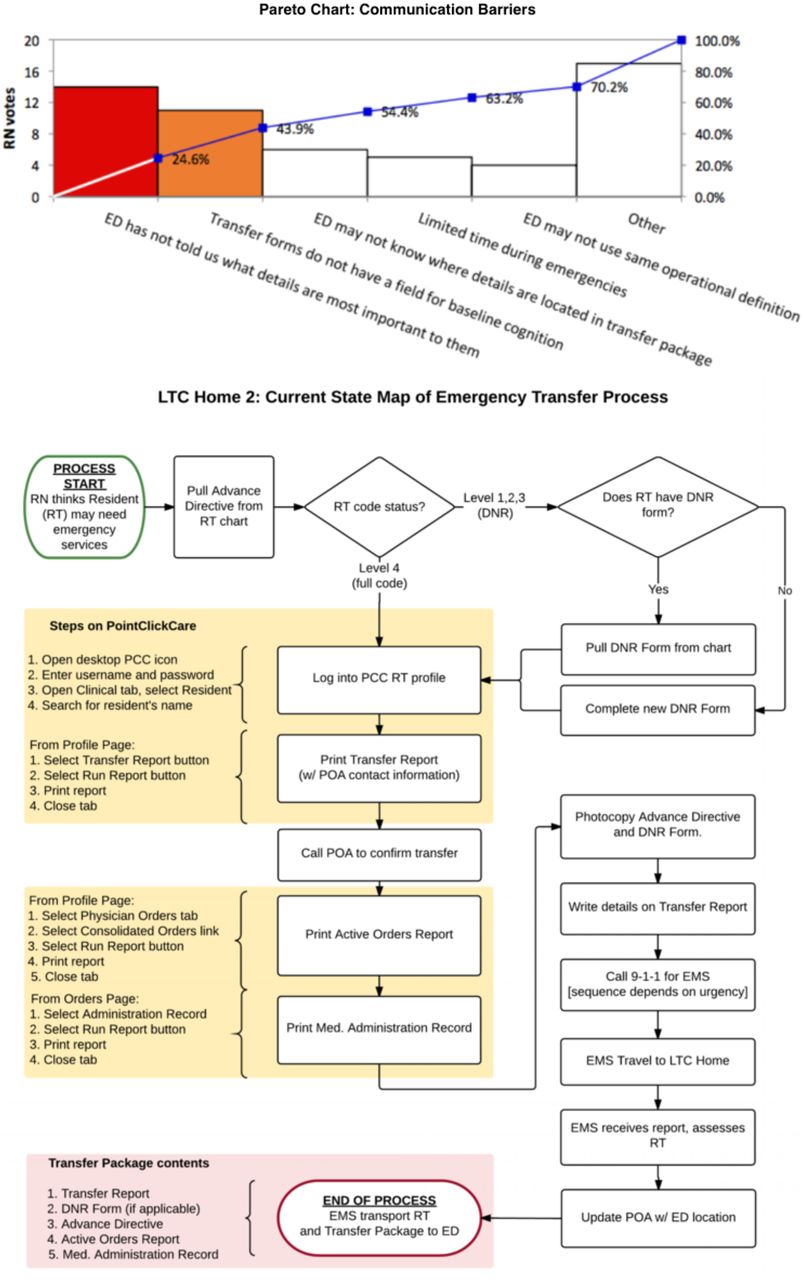
After confirming the extent of the quality gap in our baseline audit, we performed a root cause analysis with LTC nursing staff to learn about their perspective. Four LTC homes participated in process mapping exercises within their clinical areas, and nursing staff from two homes participated in Ishikawa brainstorming and Pareto multivoting exercises to find common communication barriers (figure 1).

LTC Home nurses brainstorm and voteon the most common perceived barriers to emergency transfer documentation. ED, emergency department; EMR, electronic medical record; LTC, long-term care; RN, registered nurse; DNR, do-not-resuscitate; EMS, emergency medical services (ambulance); POA, power-of-attorney.
The current state maps revealed similar process steps; however, not all homes included the same forms in transfer reports, and documentation practices varied within and between homes. Two major root causes were identified: (1) the ED had not clearly communicated what information was needed; and (2) the current transfer forms did not have a field to document baseline cognitive status.
Change ideas were tested and implemented at seven LTC homes in London-Middlesex that all used the same EMR. Based on our root cause analysis, our interventions centred on improving and standardising the information package sent at the time of transfer.
Strategy
PDSA Series 1: modifying EMR forms
Our team’s first change ideas required modification of the existing transfer form: reordering text fields, improving instructions and autopopulating data from the EMR. We hypothesised that a redesigned form would help staff document the reason for transfer as a top priority, and baseline cognitive descriptors could be autofilled from residents’ validated minimum data set (MDS) assessments, which are conducted quarterly on all LTC residents in Ontario. Our PDSA (plan-do-study-act) cycles involved gathering feedback from LTC nurses and MDS coordinators, and investigating the EMR system’s ability to customise forms. It ended by meeting with a director of the EMR company.
PDSA Series 2: introducing MDS Kardex
The failure of PDSA Series 1 led us to a second change idea: sending the MDS Kardex in all emergency transfers. The MDS Kardex was a one-page, autopopulated summary of the resident’s most recent MDS assessment, which included details about baseline memory, communication and behaviour. We hypothesised that LTC staff would be motivated to use it in order to save time, and ED staff would benefit from receiving this information in a one-page, standardised format. PDSA cycles included surveying ED staff about the perceived value of the MDS Kardex, and educating LTC staff on accessing the form.
PDSA Series 3: standardising transfer package
The third change idea was to standardise a minimum set of forms for all emergency transfers. We hypothesised that LTC nurses would send the most essential information if their forms prompted for the right data. We identified four forms that were available to LTC homes using the most common EMR system, and trialled them as a standard transfer package: (1) Transfer/Discharge Report; (2) MDS Kardex; (3) Medication Administration Record; and (4) Advance Directives (including the Ontario DNR form if applicable). Our PDSA cycles involved group and individual LTC nurse education, and the development and modification of a one-page guide (Appendix C) posted at every nursing station.
PDSA Series 4: audit-feedback
The final change idea was for the chart reviewer to provide individual feedback to LTC team leads when a transfer package was missing a documented reason for transfer, baseline cognition or standard form. We hypothesised that this feedback would provide LTC nurses with reminders about the process change and offer reassurance that hospital staff were in fact reading their transfer documents, which was a common concern. Our PDSA cycles involved asking permission from LTC leads to participate in reviewing recent transfers with their staff as often as needed.
Our outcome measures were the percentage of transfer reports documenting reason for transfer and baseline cognition. Our process measures were the percentage of transfers containing the MDS Kardex and all four standard forms. Our balance measures included the percentage of transfers documenting medications and advance directives, which the ED also rated as high-priority information.
Results
Over the course of the project, 250 transfers were analysed between October 2015 and July 2016. Interventions were implemented and spread across LTC homes between January and June 2016. Transfers were reviewed using the same process as in baseline data collection. Transfers were analysed chronologically in subgroups of 10 patients. Subgroups were then plotted on statistical process control p-charts to identify special cause variation.
PDSA Series 1 was aborted after meeting with a director from the EMR company. Due to other projects under way, the company was not interested in modifying the existing transfer documentation process at this time. We were therefore unable to reorder text fields, add new fields or autopopulate information into the form from the electronic chart.
PDSA Series 2 began in January 2016. ED physicians and nurses were surveyed prior to implementation and 92% (60/65) rated the MDS Kardex as ‘useful’ or ‘very useful’ on a 5-point Likert scale. Individual and group education for LTC nurses was provided on how to access the MDS Kardex. Analysis of transfer reports showed that inclusion of MDS Kardex increased from 0% to 52% by study end.
PDSA Series 3 also began in January 2016. Individual and group education for LTC nurses was provided on which forms should be included in the standardised package and how to access them. Analysis of transfer reports showed that inclusion of all four forms in the standardised package increased from 0% to 40% by study end.
PDSA Series 4 was aborted after some LTC leads resisted the idea, citing the high workload requirements to identify nurses involved in specific transfers and retrain them in the documentation process.
However, there was a trend showing increasing documentation rates in ‘baseline cognition’ after individual nurse feedback was implemented (figure 2).
![[SP1.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/6/2/e000024/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
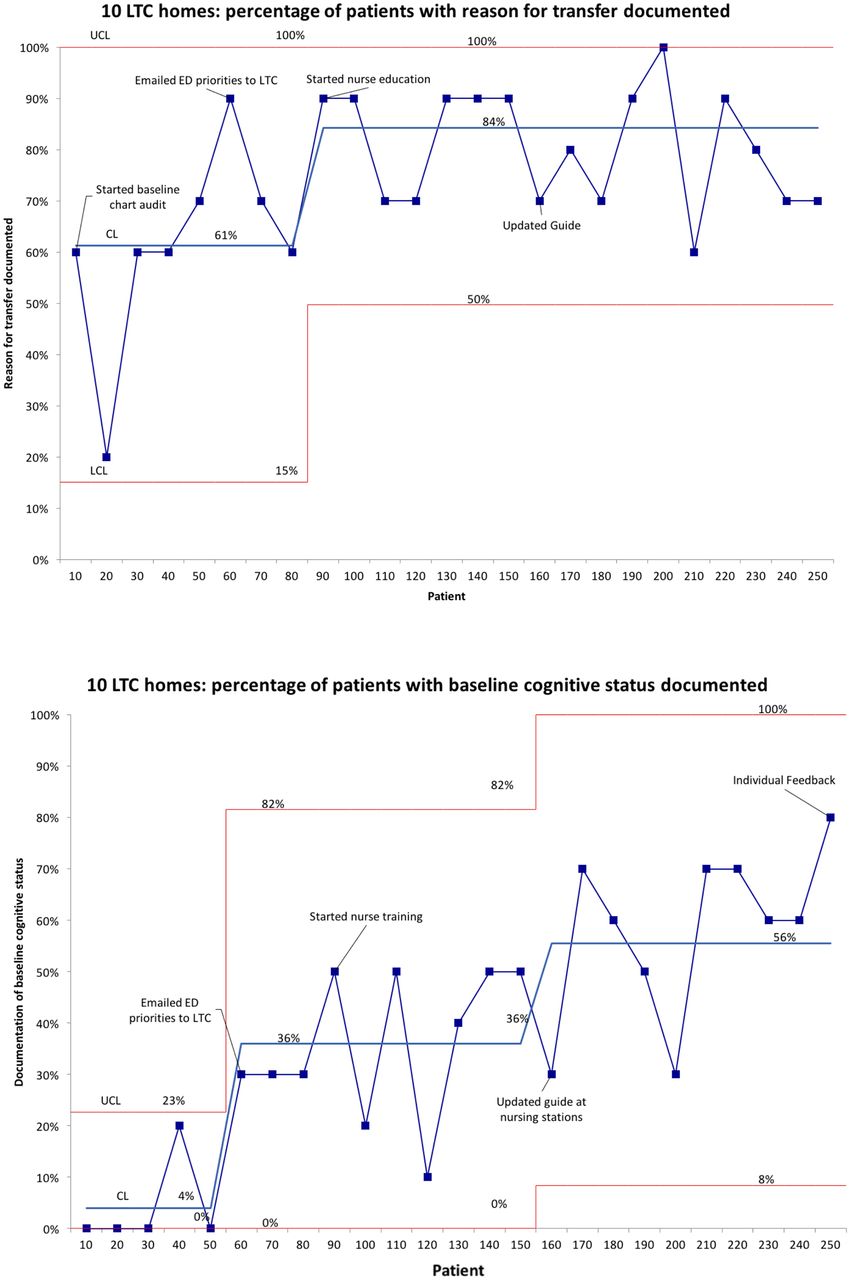
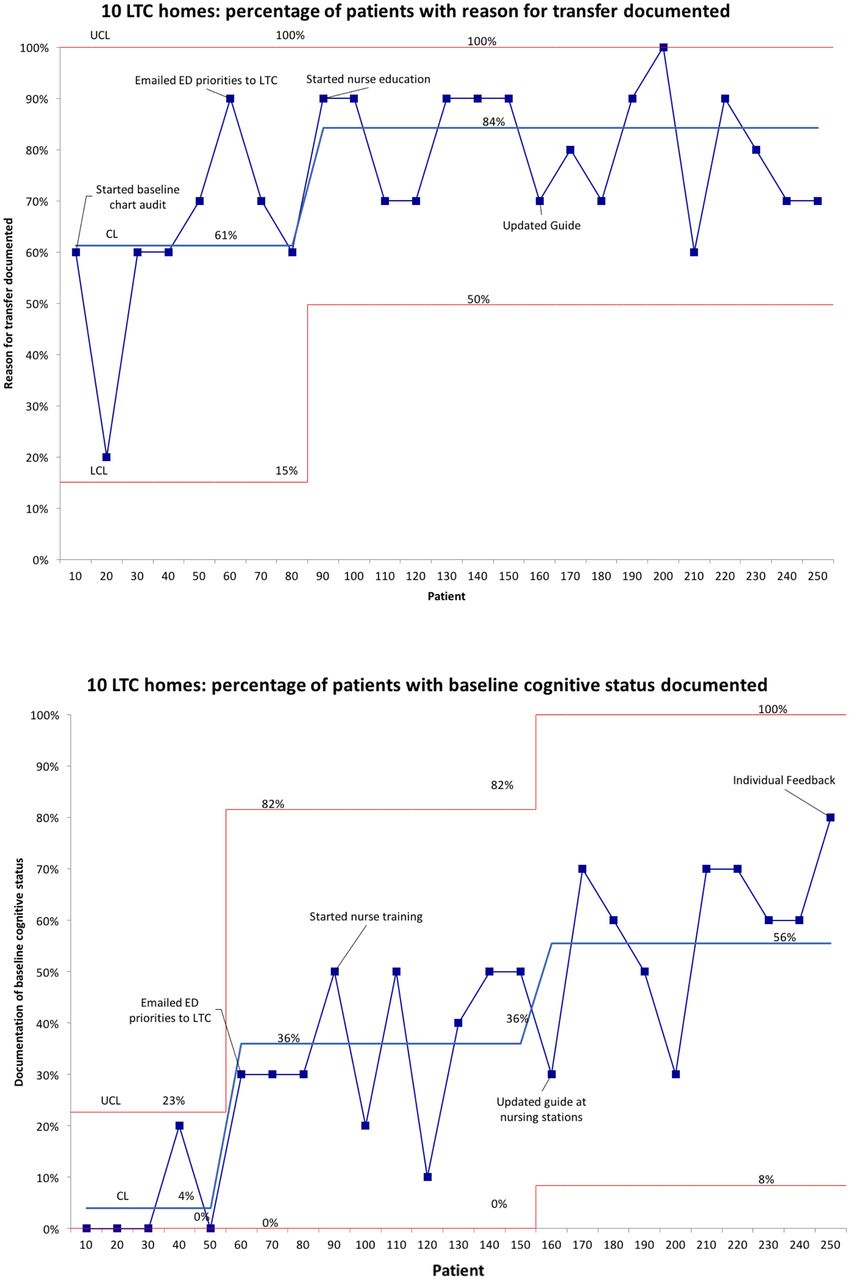
Statistical process control p-charts: outcome measures. CL, centre line; ED, emergency department; LCL, lower control limit; LTC, long-term care; UCL, upper control limit.
By April 2016, documentation of ‘reason for transfer’ increased from 61% to 84% (figure 2) and ‘baseline cognitive status’ increased from 4% to 56% (figure 2), both showing special cause variation.
Improvements in ‘reason for transfer’ were sustained throughout the intervention period, while documentation of ‘baseline cognition’ was still increasing at the end of the study. Throughout the study, there were no significant changes in balance measures—the documentation rate of medications and advance directives. See online supplementary figure 2.
Supplementary Figure 2
![[SP2.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/6/2/e000024/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
Lessons and limitations
In this quality improvement project, we were able to increase documentation of the two most important details—reason for transfer and baseline cognitive status—in LTC transfer reports to the ED. While we did not reach our goal of 90%, we achieved and sustained a documentation rate of over 80% for ‘reason for transfer’, and over 50% for ‘baseline cognitive status’. The analysis of our process measures suggests that improvements were likely attributable to our change ideas in PDSA Series 2 and 3, along with the initial communication of what the ED requested in our baseline survey. The stability of our balance measures shows that documentation of other important items did not decrease throughout the study.
The success of this project may have stemmed from a detailed root cause analysis and broad engagement of relevant stakeholders. The root cause analysis revealed that the ED had not formally requested specific information from LTC homes. As well, there was no standard process or MDS for transfer documentation. We focused on these issues and involved frontline staff in the development of change ideas. The continuous collection of performance data provided ongoing feedback about the project’s progress and allowed us to adapt change idea implementation accordingly.
Previous interventions have mostly focused on introducing new, standardised transfer forms to improve documentation quality. These forms were successful when used, but uptake remained low.9–11 Our initial change idea involved modifying forms directly within the EMR, which would have increased usability, streamlined workflow and promoted sustainability. Unfortunately, we did not have support from the EMR company. Future researchers may consider engaging the EMR company earlier with participation from regional healthcare administrators. In this case, instead of designing new forms, we focused on increasing transmission of forms that were already available. The MDS Kardex was autopopulated, meaning that LTC nurses only needed to print it. By minimising extra work, we decreased barriers to adherence with the intervention.
This study had a number of limitations. Ideally, outcome measures should reflect the patient’s ED experience, such as length of stay or unnecessary diagnostic testing. Since these quality and safety measures are multifactorial performance indicators, we selected surrogate outcome measures that would be influenced by changes on a smaller scale. While we were able to show an improvement in documentation, we do not know how this ultimately impacted patient health. We also did not measure LTC and ED staff satisfaction with the new transfer process; there is a future opportunity to test its effectiveness by surveying ED clinicians about whether it has impacted their care, and asking for further feedback from LTC nurses.
Data were collected by non-random sampling, which may have introduced bias into the study. While nurses on the project team attempted to collect each consecutive LTC transfer report, it is possible that some were missed. As well, nurses sampled more heavily from ED charts than inpatient charts; there may have been an undetected difference between patients discharged from ED and those admitted.
While we initially partnered with 10 LTC homes, we had difficulty organising and conducting PDSA cycles at multiple organisations. We chose to focus on the seven homes with the highest number of transfers to LHSC, all of which used the same EMR. Because of the practical aspects of meeting and training nurses at seven homes, PDSA cycles were conducted throughout a 4-month period. Not every home began each PDSA series at the same time, leading to a gradual improvement in outcome and process measures as opposed to an improvement immediately following the implementation of a change idea. This staggered approach helped us develop and modify PDSA at each home.
This project was designed to be scaled across several LTC homes during the same period of time. There are 23 LTC homes in London-Middlesex county, and further work will involve engaging other homes to spread our intervention. While the principles of the intervention—standardising the transfer package and engaging frontline nursing staff—could be applicable to any similar quality improvement project, our change ideas were specifically geared towards the most commonly used EMR in London-Middlesex and would need to be further adapted if used with a different system. In order to ensure sustainability, chart audits will need to occur on a regular basis and results plotted on process control charts to determine if special cause variation has occurred. However, as we have not yet met our goal of 90% documentation of ‘reason for transfer’ and ‘baseline cognitive status’, the next focus will be to continue improving documentation of these important details until these goals are reached.
Conclusion
International research has identified a consistent and significant quality gap in LTC transfer reports to the ED. This study showed that engagement of frontline LTC staff and standardisation of transfer packages led to significant improvements in documentation of ‘reason for transfer’ and ‘baseline cognitive status’ during LTC transfers to the ED.
Acknowledgments
Long-term care homes: Chartwell London, Craigwiel Gardens, Elmwood Place, Henley Place, McCormick Home, Middlesex Terrace, Mount Hope Centre for Long-Term Care, peopleCare Oakcrossing London, Strathmere Lodge, Westmount Gardens. London Health Sciences Centre: James Calvin, Janine Clift, Adam Dukelow, Chantal Forristal, Robin Francis, Leon Petruniak, Tim Rice. South West LHIN: Anita Cole. University of Toronto: Elaine Aimone, G. Ross Baker, Tom MacMillan, Anne Matlow.
Footnotes
Contributors JC was involved in building organisational partnerships, study design, data collection, change implementation, analysis and writing. SG was involved in study design, data analysis and writing. AG and SL provided mentorship on research design and project oversight.
Competing interests None declared.
Patient consent This study involved 11 organisations with independent research ethics policies. The organisations, represented by their executive directors, were asked for written voluntary consent to participate in the study. JRC also signed a confidentiality agreement with each LTC home, since he was exposed to patient information at LTC homes during staff training.
Ethics approval Ethical consideration at LHSC was provided by the Western University Health Sciences REB. The study was exempt from full board review since it was considered ‘quality improvement activity’ under TCPS Article 2.5.
Provenance and peer review Not commissioned; externally peer reviewed.