Article Text

Abstract
Introduction The imperative to learn when a patient dies due to problems in care is absolute. In 2017, the Learning from Deaths (LfDs) framework, a countrywide patient safety programme, was launched in the National Health Service (NHS) in England. NHS Secondary Care Trusts (NSCTs) are legally required to publish quantitative and qualitative information relating to deaths due to problems in care within their organisation, including any learning derived from these deaths.
Method All LfDs report from 2017 to 2020 were reviewed and evaluated, quantitatively and qualitatively using sequential content and reflexive thematic analysis, through a critical realist lens to understand what we can learn from LfDs reporting and the mechanisms enabling or preventing engagement with the LfDs programme.
Results The majority of NSCTs have identified learning, actions and, to a lesser degree, assessed the impact of these actions. The most frequent learning relates to missed/delayed/uncoordinated care and communication/cultural issues. System issues and lack of resources feature infrequently. There is significant variation among NSCTs as to what ‘learning’ in this context actually means and a lack of oversight combining patient safety initiatives.
Discussion Engagement of NSCTs with the LfDs programme varies significantly. Learning as a result of the LfDs programme is occurring. The ability, significance or value of this learning in preventing future patient deaths remains unclear. Consensus about what constitutes effective learning with regard to patient safety needs to be defined and agreed on.
- Health policy
- Patient safety
- Qualitative research
- Quality improvement
- Hospital Mortality
Data availability statement
Data are available in a public, open access repository. All data used in this study are publicly available from NHS Secondary Care Trusts Quality Accounts.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In order to reduce preventable or potentially preventable hospital deaths effective learning and sharing of learning is required. Health policies and patient safety programmes with statutory reporting requirements are used to drive improvements.
WHAT THIS STUDY ADDS
Statutory reporting can enable patient safety improvements although with variable engagement. Similar problems and learning are found repeatedly, this learning is not obviously shared and an assessment of impact of changes made are not evaluated.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Further research about what constitutes effective learning with regard to patient safety needs to be undertaken. Support for robust implementation and evaluation of patient safety programmes (including LfDs) should be ensured by policy makers.
Introduction
Within higher-income countries, between 0.5% and 8.4% of hospital deaths are preventable or potentially preventable.1 The need to learn, to disseminate learning and to demonstrate that learning has been achieved when a patient dies due to problems in care is highlighted in multiple patient safety reports and inquiries both nationally and internationally.2–5 Bereaved families frequently voice that learning to prevent future harm, in addition to acknowledgement and support for their harm are needed.6–8
In 2017, the Learning from Deaths (LfDs) framework, a countrywide patient safety programme, was launched in the National Health Service (NHS) in England. This was in response to reviews at Southern Health NHS Trust and other NHS Secondary Care Trusts (NSCTs) within England demonstrating a lack of systematic approach and meaningful change occurring in response to unexpected deaths.9–11 Guidance was subsequently published on implementing the LfDs framework at NSCT board level,12 with amendments to statutory regulations, making annual reporting of both quantitative and qualitative information relating to patient deaths a legal requirement in England.13 The quantitative information required included the number of patients who died more likely than not due to problems in care. The qualitative information required included a description of learning, actions taken as a result of learning and an assessment of impact of these actions in relation to deaths due to problems in care. The reporting mechanism was built into the NHS ‘Quality Accounts’ system: where NSCTs are legally required to produce a publicly available annual report about the quality of their services (UK government legislation).14 Guidance was given that NSCT board leadership should ‘share relevant learning across the organisation and with other services’,12 and that NSCTs should ‘engage meaningfully with bereaved families and carers’.8 There was no guidance about the format in which the qualitative data should be presented or suggested methods NSCTs could use to evaluate impact. Lalani and Hogan (2021),15 in their narrative account of the key drivers in the development of the LfDs programme, highlighted the tension arising due to competing goals of developing a learning culture while also increasing accountability through regulation.15
Prior to the introduction of the LfDs framework, there has been a longer standing legal requirement within the UK, that all deaths including NSCT deaths where the cause is unknown, or of unnatural cause are referred to and investigated by a Coroner. Coroners are statutorily required to issue a Prevention of Future Death (PoFD) report to individuals or organisations who are able to action appropriate changes where problems in care are identified as potentially causing or contributing to a death.16 Leary et al17 (2021) review of PoFD reports from 2016 to 2019, found five common learning ‘themes’: A deficit in skill or knowledge, missed/delayed/uncoordinated care, communication/cultural issues, system issues or lack of resources.17 The ‘themes’ identified (inductively) are similar to those identified in many other UK inquiries and reports from organisations investigating deaths due to problems in care.18–20
Historically, recording, investigating, reviewing incidents and superficial learning appear to have been the major focus in patient safety, with less focus on effective learning through action, demonstrating the real impact of this intervention and spreading adoption when impact is found.21 For example, with PoFD reports, NSCTs are expected to respond (within 56 days) explaining how they intend to or have made changes, however, there is no process for following up actions proposed, including decisions to take no action, or for assessing whether any actions taken have resulted in measurable improvements.16 Another example is found in the 2019 Care Quality Commission (CQC) report which reviews the ‘first year’ of NSCTs implementing the LfDs guidance, where four of the five future recommendations in the report focus on the process of investigation.22 Investigating while important does not enable discovery of effective solutions, NSCTs and NHS staff often know what the problems are, but do not have the resources or impetus to fix them.
This study thematically analyses LfDs reports to understand what we can learn from reported ‘learning’, what actions NSCTs are taking in response to this learning, how NSCTs are assessing the impact of these actions and overall engagement with the LfDs programme. In addition, we analyse two non-statutory requirements of the LfDs reports: sharing of learning and engagement with bereaved families/carers. This study does not analyse the quality of reporting, this will be presented in a separate paper.
Method
This is a study of an NHS safety improvement programme positioned through a critical realist lens to identify and understand the real causal mechanisms enabling or preventing engagement with the LfDs programme.23 We undertook a secondary source document analysis using sequential content (for quantitative counts through a qualitative process), ⇓then thematic (for fuller qualitative) analysis of all LfDs reports from NSCTs publicly available Quality Accounts between 2017 and 2020 (ambulance Trusts were excluded as they were not required to report in 2017/2018).24–689 Content analysis as described by Morgan690 (1993) is used to describe and quantify ‘patterns in the data’. Reflexive thematic analysis (TA) as described by Braun and Clarke691 (2021) has been used for its flexible, yet structured approach to find ‘shared meaning’ in the data while enabling researcher consideration of their own impact on data interpretation. Reflexive TA in this study enables evolution of and contextualisation of the content analysis through greater understanding of the causal mechanisms affecting engagement with the LfDs programme. The authors have purposefully used these two different approaches, despite the tensions arising, to provide a fuller explanation of NSCTs empirical reporting, to engage with frontline staff (who embrace quantitative research) and to reveal underlying deeper causal mechanisms impacting engagement with health policy. Our objectives for this study were to derive key understanding for the NHS front-line staff, managers, policymakers and beyond, by analysing LfDs reports.
A deductive approach to content analysis was undertaken, informed by Brummell et al (2021) paper and previous research and enquiries analysing deaths due to problems in care as described in the introduction.1 Content analysis and reflexive TA were sequentially used to analyse: learning, actions taken as a result of learning, an assessment of impact of these actions, how bereaved families had been involved in any learning and if/how learning had been shared. With reflexive TA a deductive then subsequent inductive approach was used to assess NSCT engagement with the LfDs programme. The methodology used was a process of data familiarisation (reading each report twice on separate occasions), systematic data coding (through content analysis), generating initial domains deductively, then developing multidimensional themes inductively through active engagement and immersion in the data, looking both at what was present and what was absent. Finally, these themes were refined by sense checking with the original reports and discussion with the other authors.
Every LfDs report was reviewed by the primary reviewer (ZB) twice, on separate occasions to ensure full data capture. 10% of reports from 2018/2019 and 2019/2020 were identified by random number generation and reviewed independently by a second reviewer (ZH) to ensure accurate and reliable coding for the content analysis. In the case of disagreement, (of which there was only one for each year) ZB re-reviewed the LfDs report for clarification. Reflexive TA was undertaken by ZB only.
Data were captured in Microsoft excel (V.16.15). This study has been reported using Standards for Reporting Qualitative Research, for the content analysis.692
Reflexivity
Reflexivity was undertaken alongside the research methodology, as described by Trainor and Bundon (2021).693 For additional information, see online supplemental page 1.
Supplemental material
Patient and public involvement
This study forms part of a larger programme of work overseen by a public and relatives steering group to improve relevance from the perspective of those affected by deaths in healthcare and to reduce biases from the healthcare staff researchers. The steering group have been involved in the planning, design and development of conclusions, through videoconferencing and email correspondence. The involvement of a steering group member in authoring this paper has significantly and positively influenced the reporting of this study, ensuring focus on reporting family involvement. The reporting of PPI has been undertaken using guidance for reporting involvement of patients and the public 2—short form.694
Results
Quantitative content analysis
The number of NSCTs is reducing year on year due to mergers of NSCTs: 222 NSCTs in 2017/2018, 217 NSCTs in 2018/2019, 213 NSCTs in 2019/2020.
Through systematic data coding, different types of ‘learning’ and ‘action’ were identified, defined and refined. The most common ‘learning’ and actions undertaken across all NSCTs (as % of all trusts who reported learning: 2017/2018 N=195, 2018/2019 N=191, 2019/2020 N=173) can be found in tables 1 and 2.
The most common learning found across all NSCTs
The most common actions undertaken across all NSCTs
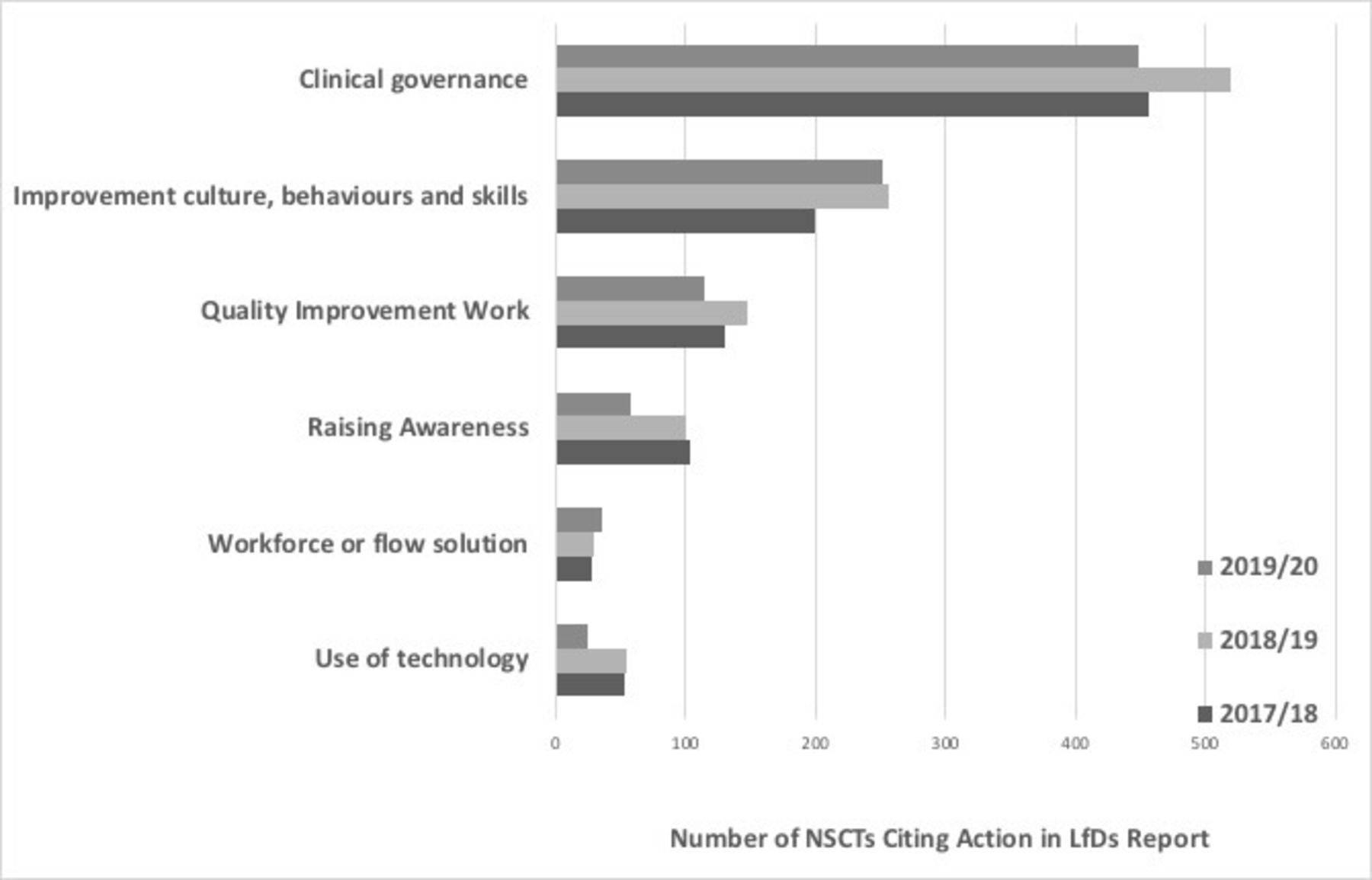
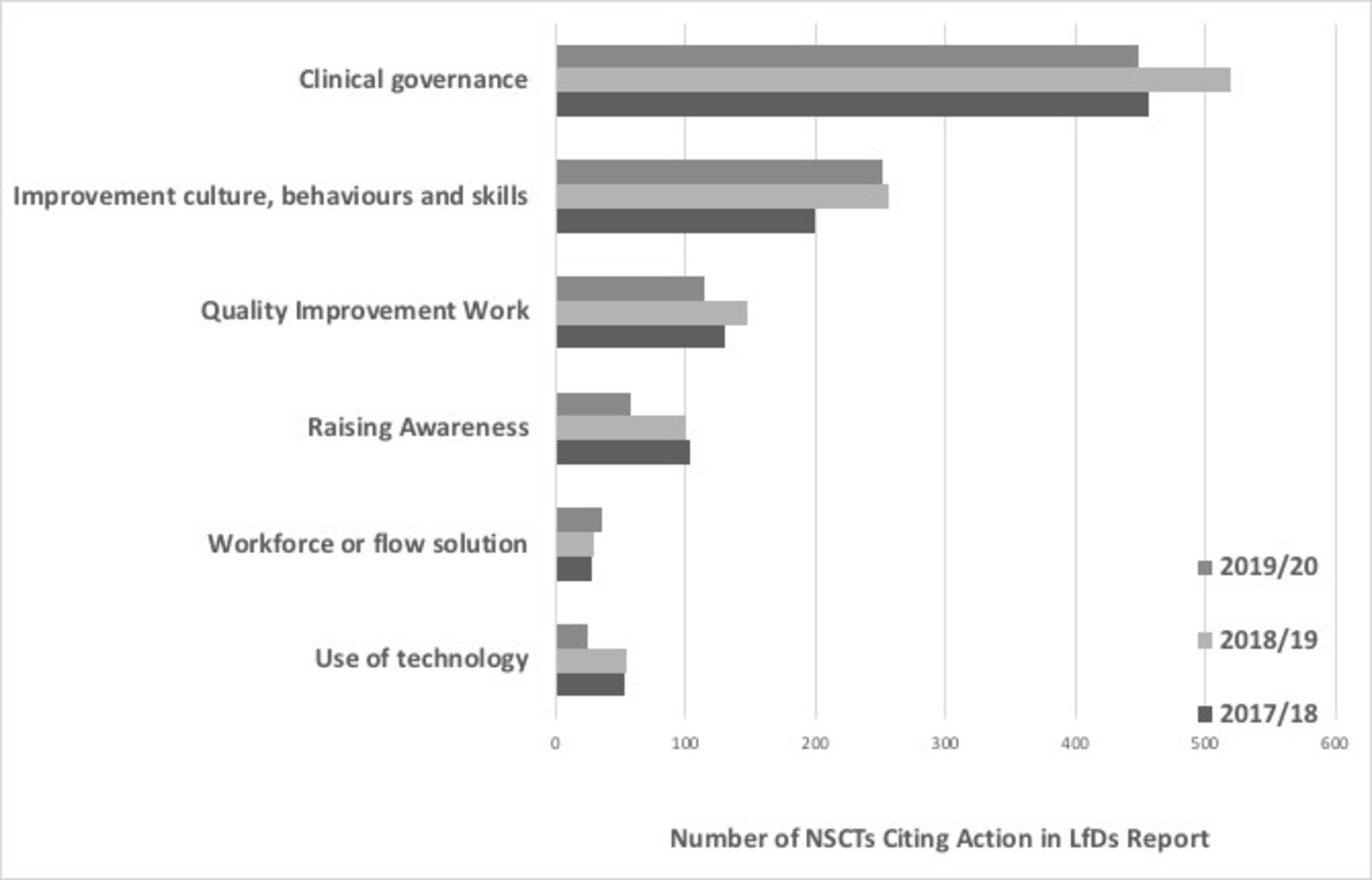
Learning’ and actions undertaken as cited in the LfDs reports were assigned into domains as seen in figures 1 and 2. Domains are also referred to as ‘topics’ or even as ‘themes’ by some researchers.695
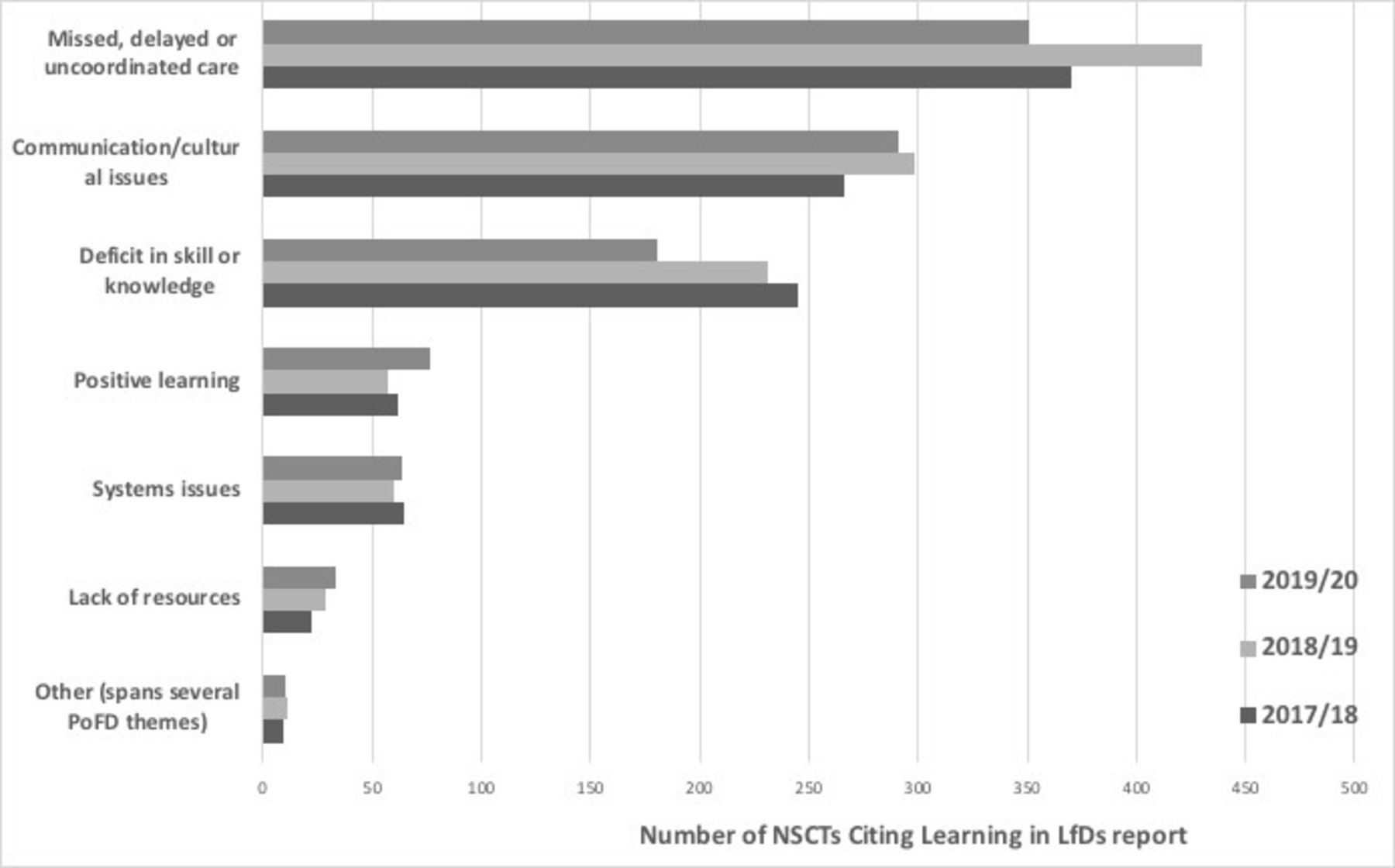
Frequency table of learning domains identified from all NSCTs. LfDs, Learning from Deaths; NSCTs, National Health Service (NHS) Secondary Care Trusts. PoFD; Prevention of Future Deaths
{kind=link}
{kind=link}
Frequency table of action domains identified from all NSCTs. LfDs, Learning from Deaths; NSCTs, National Health Service (NHS) Secondary Care Trusts.
Qualitative content analysis
Very few NSCTs articulate the problem or problems in care that led to the reported ‘learning’ and/or actions. Where the problem or problems were identified, there was a lack of detail about the problem to understand what actually happened to the patient and why. Many NSCTs did not differentiate ‘learning’ from actions or confused ‘learning’ with actions. Some NSCTs described ‘learning’ not followed by actions addressing the ‘learning’. NSCTs did not comment on LfDs ‘learning’ or action from previous years and did not describe the impact of this or how things had changed or improved year on year. Many NSCTs who did not report deaths due to problems in care still reported ‘learning’ and/or actions.
Assessment of impact of actions
NSCTs who published an LfDs report and provided information about an assessment of impact of actions is as follows:
In 2017/2018: 105 out of 220 (47%)
In 2018/2019: 123 out of 214 (57%)
In 2019/2020: 79 out of 202 (39%)
Assessment of impact of action includes NSCTs that have already assessed impact or have a plan to assess impact, but not NSCTs that state they have assessed impact, but have instead provided unrelated information not assessing impact.
Some NSCTs have made efforts to thoroughly assess impact with one even differentiating qualitative and quantitative assessment. Many of NSCTs that did assess impact used audits and/or quality improvement projects to do this:
‘Use of audit data (eg, improvement in TEP (Treatment Escalation Plans) and DNACPR (Do Not Attempt CardioPulmonary Resuscitation) completed from 23% to 78% following introduction of a combined form).’
‘Within the Forensic Services, the Performance Department provides an ‘action plan/Quality Improvement Project (QIP) summary and updated action plan/QIP monitoring sheet’ monthly report that the group monitors and reviews.’
The other major way that impact was assessed was through observing changes in Standardised Hospital-level Mortality Index (SHMI) and/or Hospital Standardised Mortality Ratio (HSMR):
‘The impact of the case record review process and the associated improvement actions can be assessed using the HSMR.’
‘This work has now been completed and the Trust has seen an improvement in both its key headline mortality indicators SHMI and HSMR.’
Some NSCTs did not fully specify how impact had been assessed or quantified, but did note that impact has occurred:
‘The impact of the project has been notable, and we will now update our policy and procedure to reflect our learning.’
‘The Trust believes that by implementing the above actions, patient safety and quality of care has improved.’
‘No further incidents have been reported similar to the cases identified above and it therefore appears that these were isolated cases and/or actions taken have been effective.’
Several NSCTs appear to have misunderstood what is meant by assessment of impact, for example, reiterating the purpose or process of the LfDs programme:
‘Perhaps the most important impact continues to be raising of awareness, among Trust staff, of the importance of reporting deaths through our incident reporting system as a potential learning opportunity.’
‘A key impact is the need to develop our work with mortality reviews during 2018/2019 so that all reviews are consistently undertaken to a high standard.’
Or issued statements that do not entirely make sense:
‘Where the greatest impact is evidenced is through the analysis of themes and trends so amalgamating the learning from mortality reviews with outcomes from other investigations such as complaints, serious incidents, never events and legal claims to identify the full range of issues is proving essential.’
‘It is anticipated that the impact of the actions and learning described above will impact on the care provided to patients in receipt of services across the Trust.’
Or made statements that do not assess impact of their actions despite report headings suggesting they are:
‘The Trust is 98% compliant with all relevant recommendations outlined within the National Institute for Health and Care Excellence (NICE) guideline for sepsis, with the exception of three recommendations which relate to the provision of information leaflets for adults, this work is currently in progress.’
Several NSCTs gave reasons for not including an assessment of impact:
‘An assessment of the impact of the actions taken as a result of the completed reviews will be included in each report to the Board, as the completed reviews are still under review by the services the impact cannot be described at this stage.’
‘It is difficult to determine the impact of lessons from multifactorial events such as these where human factors around decision making and communication are the root cause.’
‘It is not possible to comment on the effect of most these actions in the time period under consideration.’
Or describe the difficulties in assessing impact of actions:
‘This is difficult to quantify as the learning has been gradually developed and shared throughout the year.’
‘It is very difficult to assess the impact resulting directly from mortality reviews due to a number of different factors. These include:
‘Challenges with co-ordinating local (directorate) governance and learning with Trust-wide processes.’
Involvement of bereaved families
Of the NSCTs who published an LfDs report, those that mentioned the involvement of families/carers either in the investigation process or in shared learning or that they engage with families/carers after a patient dies:
In 2017/2018: 37 out of 220 trusts (17%)
In 2018/2019: 80 out of 214 trusts (37%)
In 2019/2020: 90 out of 202 trusts (45%)
Several NSCTs demonstrated significant positive engagement with families, particularly in 2019/2020, often (but not always) through the Medical Examiner (ME) system:
‘Promote and support involvement of patients’ families in investigations.’
‘Improve mortality reviews and embed the new medical examiner process, providing families, carers and staff with opportunities to both raise concerns and highlight examples of good practice and excellent care.’
‘The Trust continues to ensure that our direct contact with any family affected by the death of a loved one is paramount in our processes of LfDs, giving each family the opportunity to contribute to Terms of Reference for an investigation, comment on a draft report and have full disclosure of the report at sign off.’
It is clear that by 2019/2020, several NSCTs have significantly developed their ME system. Many describe in detail the ME process, but omit other statutory requirements. Another way in which NSCTs are supporting bereaved families is through specific roles, such as Family Liaison Officers and Bereavement Liaison Practitioners.
Sharing learning
Of the NSCTs who published an LfDs report, those that have shared or plan to share the learning more widely within their own organisation:
In 2017/2018: 106 out of 220 (48%)
In 2018/2019: 90 out of 214 (42%)
In 2019/2020: 93 out of 202 (46%)
This sharing occurs through a variety of communication mediums: face-to-face meetings, emails, screensavers, newsletters, events, intranet (case studies, safety alerts), for example:
‘The Trust has led two health economy-wide LfD events to ensure learning and improvement is shared across organisational boundaries.’
‘Sharing of the learning from mortality reviews continues both internally and externally, with Trust staff presenting to local GP training sessions.’
Of the NSCTs who published an LfDs report, those that have shared or plan to share the learning outside their organisation, with neighbouring NSCTs, Clinical Commissioning Groups or other national organisations:
In 2017/2018: 17 out of 220 (8%)
In 2018/2019: 28 out of 214 (13%)
In 2019/2020: 20 out of 202 (10%)
Reflexive TA
Through reflexive TA the following themes were identified:
‘What does ‘learning’ mean?’
‘Undertaking a TA’
‘Opportunities to triangulate’
‘Feeling the pressure’
‘Description of the incident/problem’
‘The importance of culture’
Further detail can be found in online supplemental page 2.
Discussion
There is no consensus as to what ‘Learning’ in the context of patient safety actually means. ‘Learning’ or to ‘Learn lessons’ appears as a catch-all term which NSCTs recognise they must do or be seen to be doing following a patient safety incident and is a frequent NSCT quote in broadcast media.696 697 This lack of definition, understanding and consensus of what is meant by effective learning by healthcare organisations may be one of the main barriers to sustained improvement in patient safety. Knowledge sharing and effective learning are complex social activities,698 made even more complicated when undertaken in complex organisations with transient workforces, reduced resources and competing priorities.699 A greater understanding of core concepts in ‘Learning’ such as double-loop learning, and the factors required for successful organisational learning need to be considered when developing healthcare safety policy.15 700
An important issue to highlight with regard to ‘Learning’ is the discord between NSCT intention of ‘learning’ and a lack of effective actions, potentially resulting in public distrust of healthcare professionals and organisations, with the propagation of harm to bereaved relatives. This lack of ‘learning’ is noted by Leary et al17 where they comment that Coroners ‘expressed concern or even frustration that learning or actions from PoFDs was not utilised and that organisations repeatedly appeared before them.’17
In this study and that of Leary et al,17 systems/lack of resources are relatively infrequently cited as being the problems relating to deaths due to problems in care.17 This is at odds with the patient safety literature and of that of healthcare investigation organisations.701 702 Linked to this is the lack of recommendations from NSCTs for improvements that focus on systemic change and redesign rather than individual performance. From the LfDs reports, it is not clear if NSCTs are not able to recognise system failure (which seems more likely) or if systems/lack of resources are not an issue. What is also missing from LfDs reports is the triangulation of data and recognition of overlapping patient safety programmes such as ensuring a ‘just culture’.703 Leadership teams in NSCTs and organisations regulating healthcare should recognise and understand patient safety as a whole, not as a series of discrete policies/programmes. Integrating instead of layering should improve both the success of these policies/programmes and the overall functioning of NSCTs.
Missed/delayed/uncoordinated care and communication/cultural issues are the two major domains cited in ‘learning’. These two domains were also in the top three themes identified by Leary et al17 and align with the three recurring patient safety themes identified by the Healthcare Safety Investigation Branch in their thematic review (2021).17 702 In this study, we found ‘learning’ codes were sometimes overlapping domains, for example, demonstrating both deficits in the skill/knowledge in combination with missed/delayed/uncoordinated care. With regard to the specific ‘learning’ codes derived from this study, there is a reduction in reporting of ‘Problem in recognition and escalation of deteriorating patients’ from 46% in 2018/2019 to 36% in 2019/2020. This may signify an improvement and/or effective learning and/or actions occurring related to this area of practice. This would fit with the increased UK national focus around recognition of the deteriorating patient.704 Perhaps a similar approach could be undertaken for enabling improvement with other frequently raised ‘learning’ codes such as ‘problems with documentation’; through an increased national focus around documentation, clinical coding and integrated electronic health records.705 706
There was an increase in reporting of ‘Lack of/problem with engagement with/support of families/carers’ from 4% in 2017/2018 to 28% in 2019/2020. This could be due in part to NSCTs increasing awareness of the LfDs guidance for NHS trusts on working with bereaved families and carers,8 more likely though is because of the increased establishment of ME Systems supporting the bereaved within NSCTs.707 Further recognition of the need for and provision of training for healthcare staff with regard to bereaved relatives was identified by a few NSCTs. Despite evidence that patient and family engagement improve patient safety, many organisations still have difficulties achieving this.708
In the case of action, this study demonstrates a reduction in reporting of ‘Review and improve process (including governance, risk, pathway, strategy)’ from 67% in 2017/2018 to 57% in 2019/2020 and a reduction in reporting of ‘Implementation programme of training/education’ from 51% in 2017/2018 to 39% in 2019/2020. The reason for these reductions could be that these actions were implemented in 2017/2018 and, therefore, NSCTs have not reiterated these actions in subsequent years. There is some evidence that teaching and training initiatives such as clinical simulation are credible improvement methods.709 There was increased reporting of ‘Work to improve communication/collaboration/shared learning’ from 43% in 2017/2018 to 57% in 2019/2020. This may reflect the increasing understanding in the critical importance of knowledge transfer and knowledge management for patient safety.710 711 Approximately half of all NSCTs did demonstrate shared learning within NSCTs, through a variety of platforms, there was however very limited evidence of shared learning between organisations. Karam et al (2018) found interorganisational collaboration in healthcare to be more challenging than interprofessional collaboration.712 This lack of interorganisational collaboration could reflect the enduring effect of the internal market, despite subsequent changes to amend this.713 714 A lack of system-level thinking as described by Vindrola-Padros et al715 (2020) is evident throughout the LfDs report, in actions implemented and ‘learning’ shared. Clinical governance is the major domain cited as an action in the LfDs reports. The ability of NSCTs to undertake effective governance is variable, affected by multiple factors including communication and relationships between clinicians and managers.716 717
Concerningly assessment of impact of actions reduced significantly in 2019/2020, after an initial rise between 2017/2018 and 2018/2019. Whether this effect was related to resourcing issues for data collection and reporting relating to COVID-19 is unknown. This reduction in assessment of impact could signify a loss of impetus for the LfDs programme. NSCTs appear to need further assistance in meaningfully assessing impact and that the ability to do so would be of global benefit to NSCTs, out with the LfDs programme. Specific guidance for patient safety teams within NSCTs in how to evaluate what are often complex interventions, could be adapted from the UK Medical Research Council and National Institute of Health Research framework for the development and analysis of complex interventions.718
There is ongoing variable NSCT engagement with the LfDs programme. Inconsistencies in LfDs and PoFD reporting raise questions about what real world difference statutory reporting makes. Understanding the real causal mechanisms/factors enabling or preventing engagement with the LfDs programme needs to be understood for success of this and future health policies and legislation. The consequences of not LfDs are multiple: economic,719 reputational, human and moral.
The aspiration of organisational memory does not seem possible in many NSCTs currently.720 721 However, some NSCTs appear to be exceling in patient safety despite similar constraints, having developed a strong patient safety culture through continuous improvement.722 The development of a culture of safety is central to any sustainable efforts towards patient safety improvement.
Conclusions
Engagement of NSCTs with the LfDs programme varies significantly. Some NSCTs are undertaking ‘learning’ and implementing actions. A few NSCTs are assessing the impact of these actions, which actions result in the greatest impact is still unknown. Asking trusts to assess the impact of actions taken, without assessing the impact of a new patient safety programme could be considered hypocritical.
Consensus about what constitutes effective learning with regard to patient safety needs to be defined and agreed on. Further support for implementation of the LfDs programme should be undertaken. This needs to include a more structured reporting framework. Evidence of effective learning, sharing of learning and engagement with bereaved families should be added to the statutory reporting requirements.
The lack of success with the LfDs programme needs to be investigated further.
Limitations
The majority of the analysis was undertaken by one researcher, potentially introducing bias. However, 10% of reports from 2018/2019 and 2019/2020 were reviewed independently by a second researcher to improve accuracy and reliability of coding. The first and second researcher agreed on coding on initial review in 95% of reports.
NSCTs may be undertaking elements of the LfDs programme, but not reporting this in their Quality Accounts as not statutorily required.
This study looks at a programme unique to England, however, the lessons learnt such as what constitutes effective learning, the need for support for implementation of patient safety initiatives and the importance of bereaved family engagement can be applied more globally.
Data availability statement
Data are available in a public, open access repository. All data used in this study are publicly available from NHS Secondary Care Trusts Quality Accounts.
Ethics statements
Patient consent for publication
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors ZB designed and led the study, collected and collated LfDs reports, undertook analysis and interpreted the findings. ZB also wrote the first draft of the paper. DB contributed to planning the study, interpreting the findings and editing the paper. ZH undertook qualitative and qualitative analysis from LfDs reports. SRM contributed to planning the study, interpreting the findings and editing the paper. CV-P contributed to planning the study, interpreting the findings and editing the paper. ZB is the guarantor.
Funding Patient and public involvement in this research was supported by the NIHR UCL Biomedical Research Centre (award number: BRC617/PPI/ZB/104990).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.